
Feeding can take over the whole day before anyone realizes it. A baby eats a little, falls asleep, wakes hungry again, coughs, fusses, arches, spits up, then wants to feed again. Parents start timing every ounce, every latch, every diaper, every cry.
By the time families ask for help, they're often carrying more than a feeding concern. They're carrying doubt. Is this normal? Am I missing something? Why does everyone keep saying “just give it time” when feeding feels harder every week?
That stress makes sense. Feeding is supposed to nourish a baby, but it also shapes sleep, growth, bonding, and the overall rhythm of family life. When it isn't going well, the problem can feel both urgent and strangely invisible.
The Silent Struggle of Infant Feeding Challenges
Many parents arrive at this point after trying all the usual advice. Different bottles. Different positions. More burping. Less burping. Faster nipple. Slower nipple. Shorter feeds. Longer feeds. None of it fully explains why the baby still seems uncomfortable, inefficient, or exhausted.
That experience is common, not unusual. Feeding problems are estimated to affect one in three to four infants and young children, and can occur in up to 25% of normally developing children, according to this review on pediatric feeding problems. That matters because many families blame themselves long before they realize how often clinicians see this pattern.
When feeding stress becomes the center of the day
A common story sounds like this:
- The baby starts hungry and eager to feed.
- A few minutes later, the latch slips, milk dribbles, or the baby begins clicking, coughing, or pulling off.
- The parent adjusts everything and tries again.
- The feed stretches on, everyone gets frustrated, and the baby still doesn't seem satisfied.
Sometimes the issue is obvious. Sometimes it isn't. A baby can look healthy from the outside and still work too hard to feed well.
Parents often describe the same feeling: “Feeding shouldn't be this hard, but I can't prove why.”
That's where structured evaluation helps. Instead of treating every feeding struggle as random fussiness, clinicians look for patterns. Oral function. Swallowing coordination. Breathing. Positioning. Caregiver stress. History of reflux-like symptoms. Possible structural issues such as those discussed in tongue-tie complications in infants.
Relief usually starts with a better question
The most useful question isn't “How do I get my baby to eat more?” It's “What is making feeding inefficient, stressful, or uncomfortable?”
That shift changes everything. It moves the conversation away from blame and toward cause. It also opens the door to solutions that fit the underlying problem, not just the visible symptom.
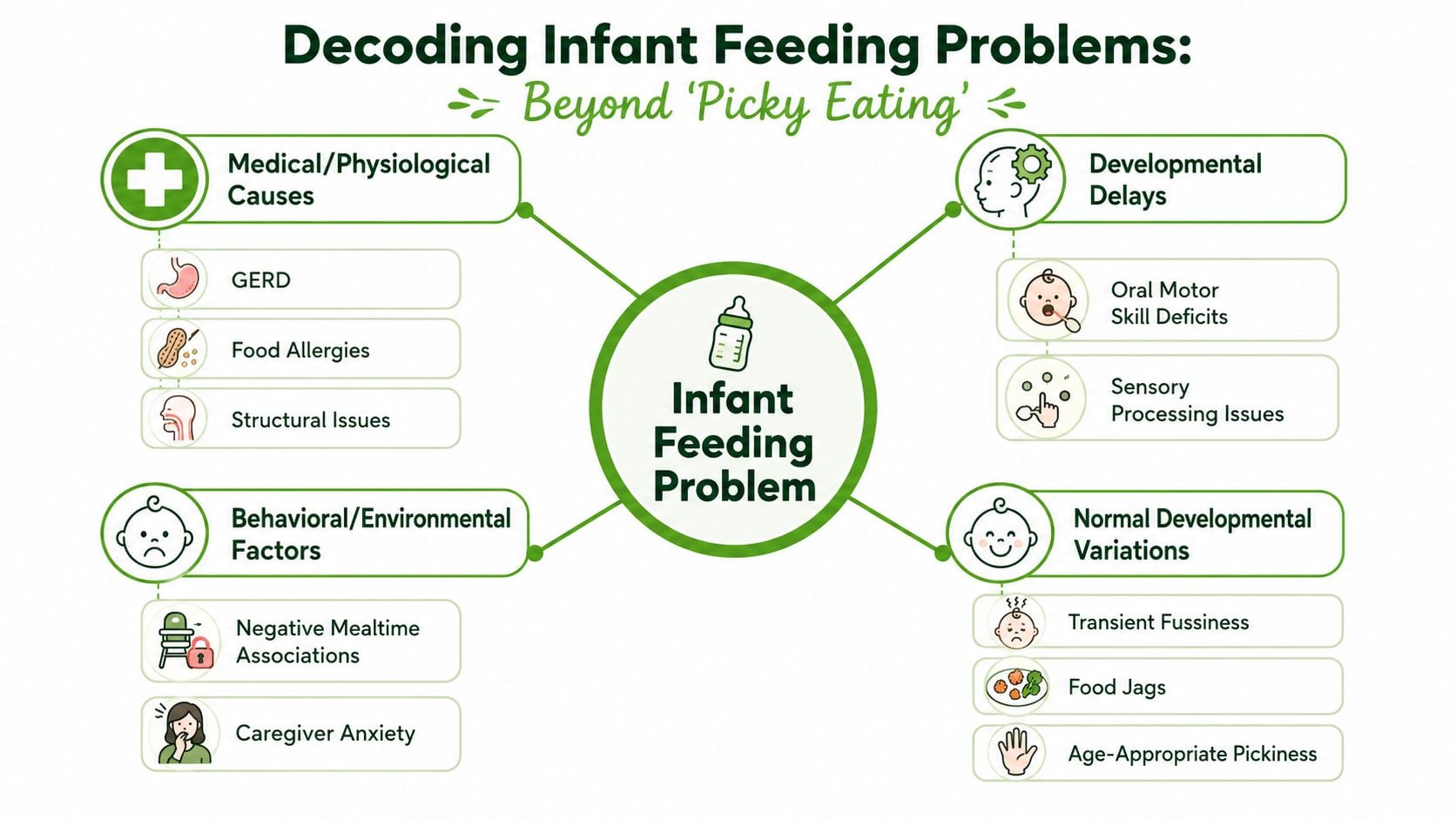
What Are Infant Feeding Problems Really
An infant feeding problem isn't just “my baby is fussy at meals.” It means feeding is harder, less efficient, less comfortable, or less safe than it should be. Sometimes the problem is mild and temporary. Sometimes it reflects a larger issue involving latch, swallowing, digestion, airway coordination, sensory response, or growth.
The spectrum matters
It helps to think of feeding difficulty like a volume dial, not an on-off switch.
At the lower end, a baby may have brief periods of fussiness, need some position changes, or go through a short adjustment phase. At the higher end, feeding can become prolonged, draining, painful, or inconsistent enough to affect intake, growth, family stress, and the baby's willingness to eat.
A useful distinction is whether feeding still works with ordinary support, or whether the baby seems to struggle despite repeated adjustments.
What counts as more than normal variation
Normal newborn behavior can include cluster feeding, brief sputtering during a letdown, occasional spit-up, or some inconsistency during growth spurts. Those patterns can be messy without being pathological.
Infant feeding problems move into a different category when you see concerns like these:
| Pattern | More likely normal | More concerning |
|---|---|---|
| Duration | Variable feed length during a busy day | Feeds regularly feel drawn out and effortful |
| Comfort | Brief fussing, then settles | Repeated distress, arching, pulling away |
| Coordination | Occasional unlatch | Frequent clicking, gulping, coughing, dribbling |
| Recovery | Baby relaxes after eating | Baby seems tired, irritated, or still hungry |
That doesn't mean every concerning sign points to a serious diagnosis. It means the feeding process deserves a closer look.
The system has to work together
Feeding depends on several functions happening at once:
- Oral function: latch, seal, tongue movement, jaw stability
- Swallow timing: moving milk safely and efficiently
- Breathing: staying organized while sucking and swallowing
- Digestive comfort: tolerating feeds without pain or repeated distress
- Regulation: staying calm enough to feed
If one part of that system is inefficient, the rest often gets strained. A baby may compensate for a while, but compensation isn't the same as ease.
Practical rule: If feeding only works when a parent constantly rescues the process, the problem probably isn't just temperament.
That's why “try another bottle” sometimes helps and sometimes doesn't. A bottle change can improve flow, but it won't fix poor tongue control, swallowing discoordination, or airway-related stress. The right vocabulary helps parents describe what they're seeing with much more precision, and that leads to better care.
Uncovering the Root Causes of Feeding Issues
The most common mistake in infant feeding problems is treating the symptom as the diagnosis. “The baby is fussy.” “The baby spits up.” “The baby takes forever to eat.” Those descriptions are useful, but they don't tell you why feeding is breaking down.
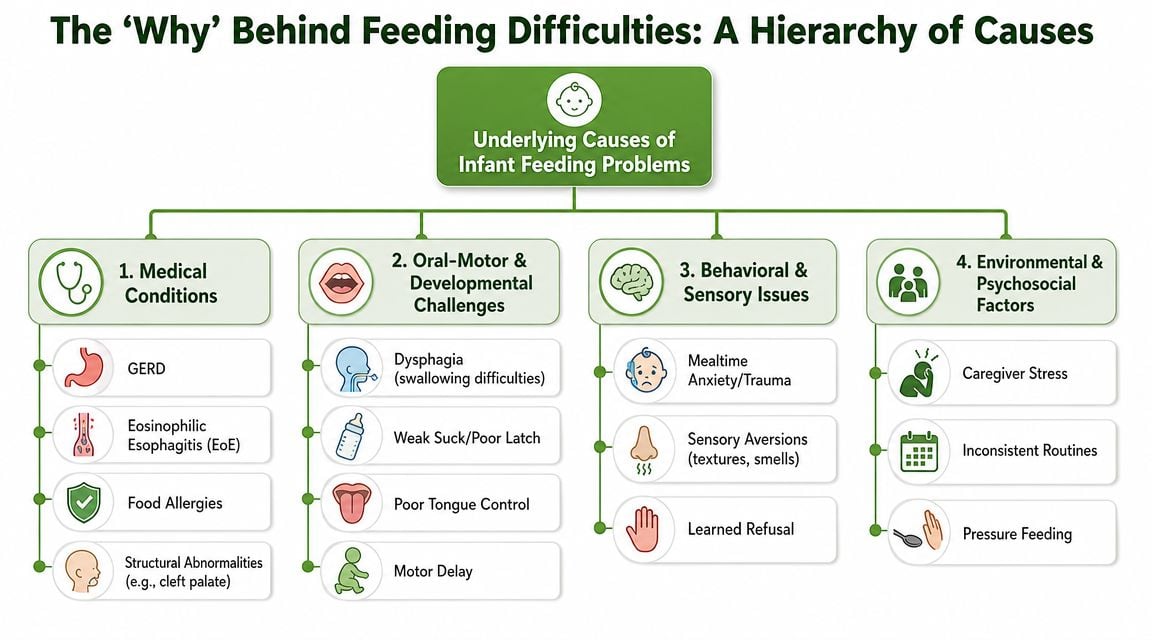
Structural and oral function causes
Some infants can't feed efficiently because the mechanics are off. The issue may involve tongue mobility, lip seal, palate shape, jaw support, or the ability to maintain suction. Parents often notice clicking, leaking milk, slipping off the breast or bottle, or a baby who seems to work hard without transferring well.
A structural finding matters most when it changes function. That's an important trade-off in practice. A visible oral restriction doesn't always explain severe feeding symptoms, and a baby can have major feeding trouble even when the mouth looks fairly typical at first glance.
Swallowing, airway, and coordination problems
Other babies have trouble coordinating suck, swallow, and breathing. These infants may cough, choke, sputter, sound wet after feeding, or fatigue quickly. Some feeds look fine for a few minutes and then fall apart when the baby tires.
Root-cause thinking is essential. A family may be told to thicken feeds, slow the pace, or use a different nipple. Those strategies can be useful, but they work best when they match the underlying problem. If the underlying issue involves swallowing safety or aerodigestive coordination, the plan often needs specialty input.
A feed that looks “messy” may actually be a baby protecting their airway, losing coordination, or tiring from the effort of breathing and eating at the same time.
Medical causes that mimic simple feeding fussiness
Medical issues can also drive feeding resistance. Reflux, allergy, gastrointestinal discomfort, structural differences, neuromuscular conditions, prematurity, and cardiac or respiratory disease can all affect how feeding feels and functions. In cause-directed management, clinicians may use laboratory work such as CBC, inflammatory markers, albumin or protein, iron studies, and ferritin, while nutrition support can include adjusting caloric density and treating reflux, allergy, or swallowing disorders, as described in this clinical review of infant feeding difficulty.
A common trap is assuming every uncomfortable feed is reflux, or every poor latch is only a tongue issue. Babies often show the same outward behaviors for very different reasons.
Family and environment are part of the cause
Feeding happens in a relationship, not in isolation. Research on infant feeding difficulty found significant associations with maternal overweight or obesity, lower maternal education, lack of adequate partner support, and mixed feeding methods. The most common complaint was difficulty latching (53.7%) in this study on infant feeding difficulties and associated factors.
That doesn't mean caregivers cause the problem. It means the feeding system includes the baby, the parent, the routine, the level of support, and the accumulated stress around meals.
Consider how these factors interact:
- Physical strain: A baby with weak oral coordination may feed poorly.
- Emotional strain: The parent becomes anxious because every feed is unpredictable.
- Behavioral fallout: The baby starts associating feeding with pressure, discomfort, or repeated interruption.
Once that cycle forms, “just keep trying” usually doesn't solve it. Families need an approach that separates symptom from cause, then matches treatment to the underlying driver.
Key Signs and Red Flags to Watch For
Parents often sense that something is off before they can explain it clearly. That instinct matters. The goal isn't to diagnose your baby at home. It's to notice patterns that deserve a closer look.
For a quick visual summary, this checklist helps organize what to watch: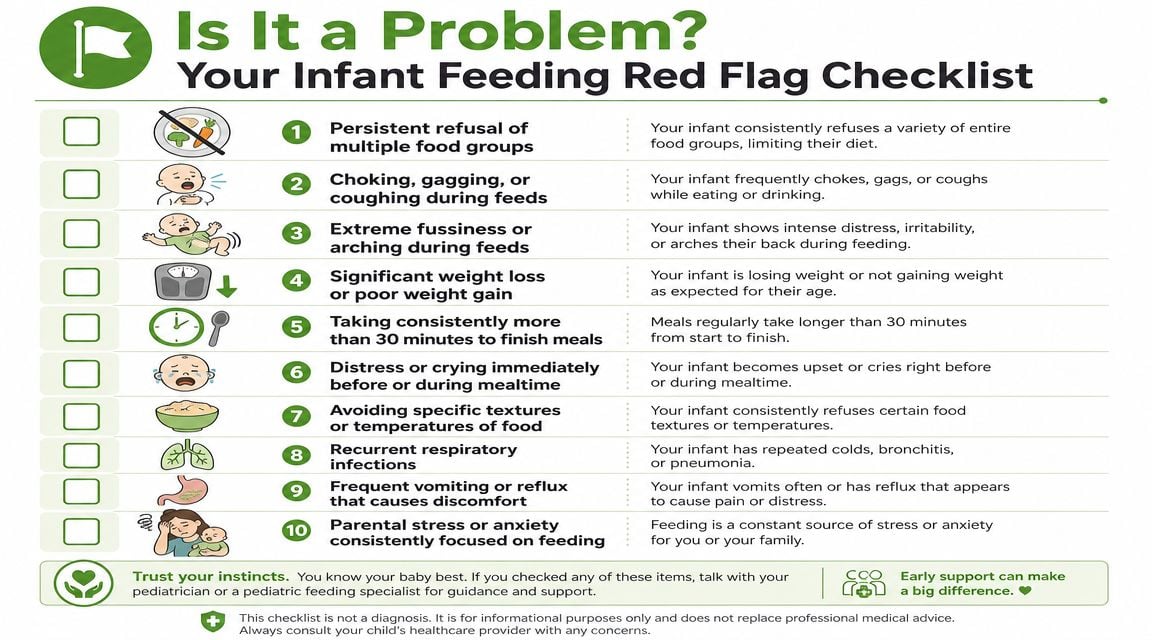
Signs that deserve attention
One red flag has a particularly clear clinical threshold. A feeding duration over 30 minutes is a key diagnostic marker when assessing infant feeding disorders, especially if stressful mealtimes and faltering growth are also present, according to BMJ Best Practice guidance on infant feeding disorder. Long feeds aren't just inconvenient. They can signal inefficient intake, excessive effort, or an underlying medical issue.
Other signs to track include:
- Breathing-related symptoms: coughing, choking, gulping, noisy breathing, or a wet-sounding voice or cry after feeds
- Oral inefficiency: clicking, losing suction, milk leaking from the mouth, repeated unlatching
- Behavioral distress: crying before feeds, arching, fighting the bottle or breast, shutting down early
- Fatigue: falling asleep quickly from effort, then waking hungry soon after
- Digestive discomfort: frequent vomiting, obvious pain with feeds, repeated refusal after a few swallows
If food allergy is part of the picture, especially when symptoms appear after exposure to specific foods, parents may also want a basic emergency-awareness reference such as What to do for nut allergy symptoms, while still speaking with their child's clinician about the bigger feeding picture.
What to write down before an appointment
A short log is often more useful than a vague memory. Try documenting:
- How long feeds take
- What your baby sounds like during feeds
- Whether the same problem happens with breast, bottle, or both
- What happens right after feeding
- Any pattern with positions, flow rates, or times of day
If you suspect latch or oral restriction may be part of the story, parents often find it helpful to compare what they're seeing with common signs described in how to tell if baby has tongue tie.
Later in the evaluation, families sometimes benefit from seeing feeding mechanics discussed in a more visual format. This video gives a useful overview:
Don't wait for a feeding problem to become dramatic. Persistent, low-grade struggle still counts.
How Specialists Diagnose and Manage Feeding Problems
A good feeding evaluation is part detective work, part pattern recognition. Specialists don't just ask whether a baby eats. They ask how the baby eats, how hard the baby works to do it, and what happens before, during, and after the feed.
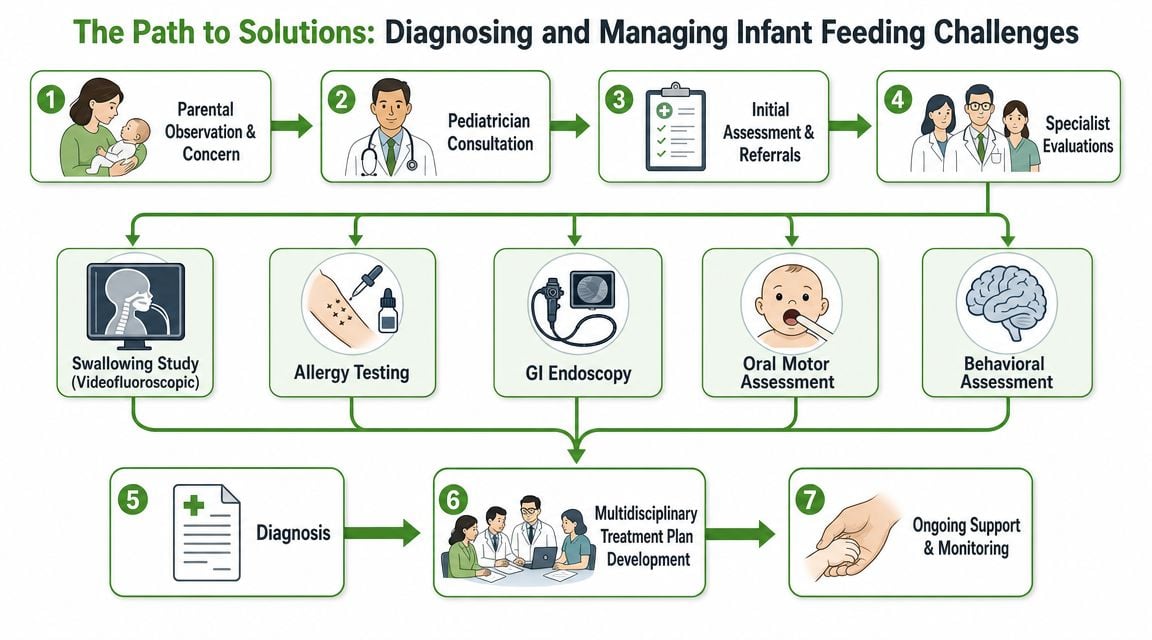
What a thorough assessment looks for
A structured workup usually includes observation of feeding mechanics and a broader medical review. Depending on the history, the team may look at:
- Latch and oral seal
- Tongue and jaw function
- Pacing and nipple flow
- Posture and positioning
- Signs of aspiration or swallow discoordination
- Growth trajectory and intake pattern
- Evidence of reflux, allergy, or gastrointestinal pain
- Airway concerns during feeds
A multidisciplinary approach becomes valuable. Lactation consultants, speech-language pathologists, ENTs, pediatricians, GI specialists, occupational therapists, and dental or oral-function providers may all see different pieces of the same problem.
Why airway matters during feeding
Breathing and feeding are tightly linked. Babies have to coordinate sucking, swallowing, and respiration in a very small space. If breathing is strained, feeding often becomes strained too. A baby may compensate by breaking suction, pausing often, becoming frantic, or tiring fast.
In infants with severe feeding difficulty and airway concerns, targeted multidisciplinary care can make a real difference. In one case series, 15 of 20 infants with severe feeding difficulties and airway concerns learned to feed orally after targeted management, as described in this report on multidisciplinary neonatal feeding care.
That kind of care may include:
- adjusting nipple flow
- paced feeding
- posture changes
- cue-based feeding
- swallow evaluation
- aerodigestive assessment
- oral motor therapy
What works and what often doesn't
Some interventions help because they target mechanism. Others help only temporarily, or make things harder if used without a clear diagnosis.
| Approach | When it can help | When it falls short |
|---|---|---|
| Bottle or nipple changes | Flow mismatch, pacing issues | Structural or swallow problems remain unaddressed |
| Positioning changes | Reflux-like discomfort, coordination support | Won't fix deeper oral dysfunction alone |
| Oral function therapy | Weak latch, poor seal, disorganized movement | Needs accurate assessment and follow-through |
| Procedure-based care | When a restriction clearly affects function | Not every feeding problem is solved by a procedure |
When tongue restriction is clearly affecting function, one option families may discuss is infant tongue-tie release. In practice, that conversation works best when it sits inside a broader assessment of latch, sucking pattern, body tension, and airway, not as a stand-alone answer.
Pain and Sleep Therapy Center is one example of a clinic that evaluates infant feeding through oral function and airway-focused care, alongside collaborative pediatric support. That kind of model can be useful when parents need more than a quick look at the mouth.
The right treatment plan should make feeding easier for the baby and less stressful for the parent. If it only changes the equipment, it may not be addressing the whole problem.
Your Practical Next Steps as a Parent
If feeding has become a source of dread, don't wait for reassurance from friends or internet forums to be enough. Seeking help isn't overreacting. It's a practical response to a problem that affects nutrition, comfort, and family well-being.
Bring useful observations, not just worry
Parents often think they need a diagnosis before making an appointment. You don't. What helps most is clear observation.
Bring notes on:
- Feed length: when feeds feel efficient and when they drag on
- Behavior: arching, crying, coughing, falling asleep, pulling away
- Pattern: whether symptoms change by time of day, position, bottle, or caregiver
- Recovery: how your baby acts after eating
- Your stress level: because feeding pressure changes the whole experience
That last point matters more than many families expect. If the household now revolves around trying to get one more ounce or one more latch, the feeding problem has already become a family issue.
Ask direct questions
You don't need fancy language. Plain questions are often best.
Try asking:
- What do you think is making feeding inefficient?
- Do you see an oral function problem, a swallowing issue, a medical issue, or a combination?
- Should my baby be evaluated for airway or aspiration concerns?
- What should we change first, and what result should we expect?
- At what point do we add another specialist?
Support progress at home without turning meals into a battle
Most families need a plan that lowers pressure while keeping feeding safe and organized. That may include paced feeding, better positioning, more realistic feed timing, and caregiver coaching so every meal doesn't become a test.
As babies grow into more independent eating, some families also like practical resources on setup and posture that can foster child's mealtime independence. It's not a treatment for infant feeding problems, but the broader idea is useful: mealtime works better when the environment supports regulation instead of adding stress.
The most important mindset shift is simple. Don't chase random fixes. Match the solution to the cause. A baby who struggles with oral coordination needs a different plan than a baby with reflux, allergy, airway concerns, or a feeding relationship that has become tense and exhausting.
Getting help early usually shortens the path. It gives you a clearer explanation, a more focused plan, and a better chance of making feeds calmer, safer, and more effective.
If feeding feels harder than it should, Pain and Sleep Therapy Center offers evaluation for infant oral function, tongue-tie, and airway-related factors that can affect breastfeeding and bottle feeding. The goal is to identify what's driving the struggle and build an individualized plan with the right next steps for your baby and your family.



