
Your baby feeds for what feels like all day, yet still seems unsettled. Nursing hurts. Bottles take forever. Your older child chews strangely, gags on textures, or struggles with certain sounds. Or maybe you're an adult dealing with jaw tension, crowded teeth, clenching, headaches, snoring, and sleep that never feels restorative.
Those problems can look unrelated. They often aren't.
A restrictive tongue tie can start as an infant feeding issue, then continue to influence oral posture, swallowing, jaw mechanics, airway function, and sleep across the lifespan. That's why tongue tie complications deserve a much broader discussion than a quick look under the tongue. The key question isn't just whether a frenulum exists. Everyone has one. The question is whether it restricts function.
More Than Just a String Understanding Ankyloglossia
Ankyloglossia, commonly called tongue tie, is a congenital restriction of the lingual frenulum, the band of tissue that connects the underside of the tongue to the floor of the mouth. When that tissue is tight, short, or poorly positioned, the tongue can't lift, extend, or shape itself the way it should.
A simple way to picture it is this. Think of a sail tied too tightly to a mast. The sail is still there. It may even look intact. But it can't fully open, catch wind, and do its job. The tongue works the same way. It's a large, powerful muscle group, and a small tether can limit the whole system.
Why function matters more than appearance
Some tongue ties are obvious. Others are subtle. A child may stick the tongue out a little and still have major restriction during feeding, speech, or rest posture. That's why a visual check alone often misses the actual issue.
In practice, I care less about how dramatic the frenulum looks and more about what the tongue can do:
- Lift to the palate so it can support nasal breathing and a stable swallow
- Cup and seal during infant feeding
- Move side to side to manage food safely
- Rest up instead of sitting low in the mouth
- Coordinate with the jaw and lips without strain or compensation
Clinical reality: A tongue tie isn't important because it's visible. It's important when the body has to compensate for it.
Those compensations can start early. A baby may clamp with the gums because the tongue can't move upward well. A child may use the jaw, lips, or neck muscles to make speech sounds. An adult may carry chronic tension because the tongue never developed a healthy resting posture.
Why diagnosis is more common now
Tongue tie isn't rare. Prevalence in newborns is estimated at 4.8% to 10.7%, and the American Academy of Pediatrics noted a nearly 10-fold increase in diagnoses from 1997 to 2012 in its discussion of changing recognition and breastfeeding impact, available through the AAP report on the rise in tongue tie diagnoses.
That doesn't mean every baby suddenly developed a new condition. It means clinicians, lactation professionals, dentists, and airway-focused teams have become more alert to how restricted tongue motion affects feeding and development. Increased recognition is not the same thing as overreaction. It often reflects better functional assessment.
The First Challenge Infant Feeding and Maternal Pain
The first tongue tie complications usually show up in the feeding chair at 2 a.m. A parent says the baby is always hungry, always on the breast, or constantly losing suction on the bottle. The other parent says feeds sound noisy. Everyone is exhausted, and many families have already been told to “just keep trying.”
That advice often misses the mechanics.
A baby needs the tongue to lift, extend, seal, and create organized pressure to transfer milk effectively. If the tongue can't do that, the latch becomes shallow and unstable. The baby may click, slip, gulp air, tire quickly, or feed for long stretches without effectively feeding.

What this looks like during a real feed
The pattern is often recognizable:
- Shallow latch that causes pinching instead of deep, rhythmic feeding
- Clicking or popping sounds when suction breaks repeatedly
- Long feeds with poor transfer because the baby works hard but inefficiently
- Fussiness, reflux-like behavior, or gas from swallowing excess air
- Early fatigue at the breast or bottle followed by frequent re-feeding
For the nursing parent, the experience can be just as significant. The infant's restriction often shows up as maternal nipple pain, trauma, cracked skin, engorgement from poor removal, and stress around every feed. Over time, ineffective milk transfer can also reduce stimulation to the breast and contribute to supply concerns.
The evidence-supported complication
The strongest evidence around infant tongue tie points to feeding dysfunction. The Mayo Clinic notes that tongue tie prevalence is 4% to 11%, that 75% of affected infants are asymptomatic, and that for babies with functional impairment, tongue tie is linked to poor latch, maternal nipple pain, and ineffective milk transfer in its overview of tongue tie symptoms and causes.
That last point matters. A visible tie alone doesn't automatically explain every feeding problem. But when feeding is painful, transfer is poor, and the tongue can't perform normally, the restriction becomes clinically meaningful.
Feeding failure is not a parenting failure. Very often, it's a mechanical problem asking for a mechanical assessment.
What helps and what usually doesn't
What works is a hands-on functional evaluation. That includes observing a feed, checking tongue lift and extension, looking at jaw compensation, and making sure other issues aren't being missed. Families often benefit from an IBCLC, a provider who evaluates oral restriction, and follow-up support rather than a one-step answer.
A practical resource for parents trying to understand that support network is Bornbir's guide to tongue tie support, which explains how lactation guidance fits into the process.
What doesn't work as well is guessing from photos, treating every fussy baby as reflux, or assuming a baby will “grow out of” poor oral mechanics. If a release is being considered, the evaluation should address function and feeding goals. For families seeking procedural information, an infant tongue tie release overview can help clarify what that step involves.
Growing Pains From Picky Eating to Speech Problems
Some children seem to leave the infant feeding stage behind, but the oral restriction doesn't disappear. It changes jobs. Instead of interfering with latch, it starts interfering with how a child manages solids, clears the mouth, and coordinates more precise tongue movements.
That can look behavioral on the surface. Often it isn't.
Why solids become frustrating
A well-functioning tongue does more than push food back to swallow. It helps collect food from the cheeks, move it side to side for chewing, shape a safe bolus, and clear the mouth efficiently. When mobility is limited, children may struggle with textures that require more control.
Common patterns include:
- Gagging on mixed or textured foods because the tongue can't organize the bolus smoothly
- Pocketing food in the cheeks when a proper tongue sweep is limited
- Messy chewing with jaw compensation instead of coordinated oral control
- Avoidance of certain textures that feel hard to manage rather than disliked
Parents sometimes hear “picky eater” when the better description is “mechanically inefficient eater.” That difference matters. If the child can't move food comfortably, repeated pressure to eat often increases stress without fixing the underlying limitation.
Speech isn't just about knowing the sound
Speech requires speed, precision, and repeated tongue contact in very specific places. A child may know exactly what sound they want to make but still struggle to produce it cleanly if the tongue can't lift or dissociate from the jaw.
Sounds that often require refined tongue placement include:
| Sound group | Why it may be hard with restriction |
|---|---|
| T, D, N, L | These sounds depend on tongue tip elevation toward the palate or upper gum ridge |
| S, Z | These need controlled airflow and stable tongue shaping |
| R | This often requires complex elevation and shaping that restricted tongues may avoid |
| Connected speech | Rapid transitions expose compensation even when single sounds seem possible |
Not every child with a tongue tie will have a speech disorder. Some adapt well. Others produce understandable speech but with effort, jaw movement, facial tension, or inconsistent articulation that becomes more noticeable in longer conversation.
A child can compensate enough to be understood and still work much harder than necessary to eat and speak.
The pattern clinicians watch for
When I hear a history that includes feeding trouble in infancy, texture aversion later, open-mouth posture, messy chewing, and speech concerns, I don't treat those as isolated boxes. I look for one functional thread running through them.
A useful evaluation asks questions like these:
- Can the tongue lift without the jaw lifting with it?
- Does the child manage solids with control or with workarounds?
- Is speech limited by language development, motor planning, or restricted range of motion?
- Are there signs of low tongue posture between meals and between words?
That broader lens keeps families from chasing one symptom at a time. A speech referral may help. Feeding therapy may help. But if a tethered tongue sits at the center of the pattern, treatment planning needs to account for the whole mechanism.
The Adult Domino Effect Dental Crowding and Jaw Pain
Adults rarely walk into a clinic saying, “I think my tongue posture changed my facial growth.” They usually come in with symptoms that feel more immediate. Jaw clicking. Clenching. Neck tightness. Facial fatigue. Headaches. Teeth that shifted after orthodontics. A bite that never feels settled.
The tongue may still be part of the story.
The tongue as an internal support system
At rest, the tongue is supposed to sit broadly against the palate. That resting posture helps support balanced swallowing and stable oral mechanics. When a tongue is tethered low, the body loses that internal support. Over time, the lips, chin, jaw, and neck often pick up the extra workload.
That matters during development, because form follows function. If the tongue can't rest where it belongs, the palate may develop differently, the dental arches may lack support, and orthodontic stability can become harder to maintain. By adulthood, the visible result may be crowding, a high palate, bite imbalance, or persistent muscular overactivity.
How compensation turns into pain
A restricted tongue doesn't only limit movement. It changes movement patterns.
Adults with longstanding restriction often show some combination of the following:
- Jaw-assisted swallowing, where the mandible helps do what the tongue should do
- Lip and chin recruitment, especially during speech or saliva swallows
- Neck and floor-of-mouth tension, because nearby muscles stay overactive
- Clenching or bracing, particularly when the bite feels unstable
- TMJ irritation, when the joint absorbs years of compensation
These aren't cosmetic issues. They can drive day-to-day symptoms. The patient may describe sore masseters in the morning, tension headaches by afternoon, and facial pain after prolonged talking or chewing. Standard splints may reduce overload in some cases, but if oral posture and tongue function remain unaddressed, the relief is often incomplete.
Why braces alone may not solve it
Orthodontics can align teeth. It doesn't automatically normalize tongue posture. If the tongue continues to rest low or thrust forward, the forces acting on the teeth and jaws may remain dysfunctional. That's one reason some adults finish treatment with straighter teeth but persistent tension, relapse, or a sense that the mouth still isn't functioning naturally.
A practical comparison helps:
| Approach | What it addresses | What it may miss |
|---|---|---|
| Bite-only focus | Tooth position, occlusion, appliance therapy | Rest posture, swallow mechanics, muscular compensation |
| Functional oral approach | Tongue posture, swallow, breathing, muscle balance | May still require dental or orthodontic coordination |
Tongue tie complications become a lifespan issue, not just a pediatric one. The original restriction may be small. The cumulative compensation often isn't.
The Critical Link to Airway Sleep and Breathing
The tongue is one of the most important airway muscles in the body. When it rests up against the palate, it supports nasal breathing and helps keep the oral cavity organized. When it sits low and back, the mouth opens more easily, nasal breathing becomes less stable, and the airway can become more vulnerable during sleep.
That link is easy to miss because the symptoms don't always start in the mouth. They show up as snoring, restless sleep, dry mouth, fatigue, poor concentration, headaches on waking, and a sense that sleep never fully restores energy.
How low tongue posture changes breathing
A tethered tongue often can't maintain an ideal resting position. The body then adapts. The lips may part. The jaw may drop. Mouth breathing becomes the path of least resistance. Once that pattern takes hold, it can influence facial muscle use, swallowing, and nighttime airway behavior.
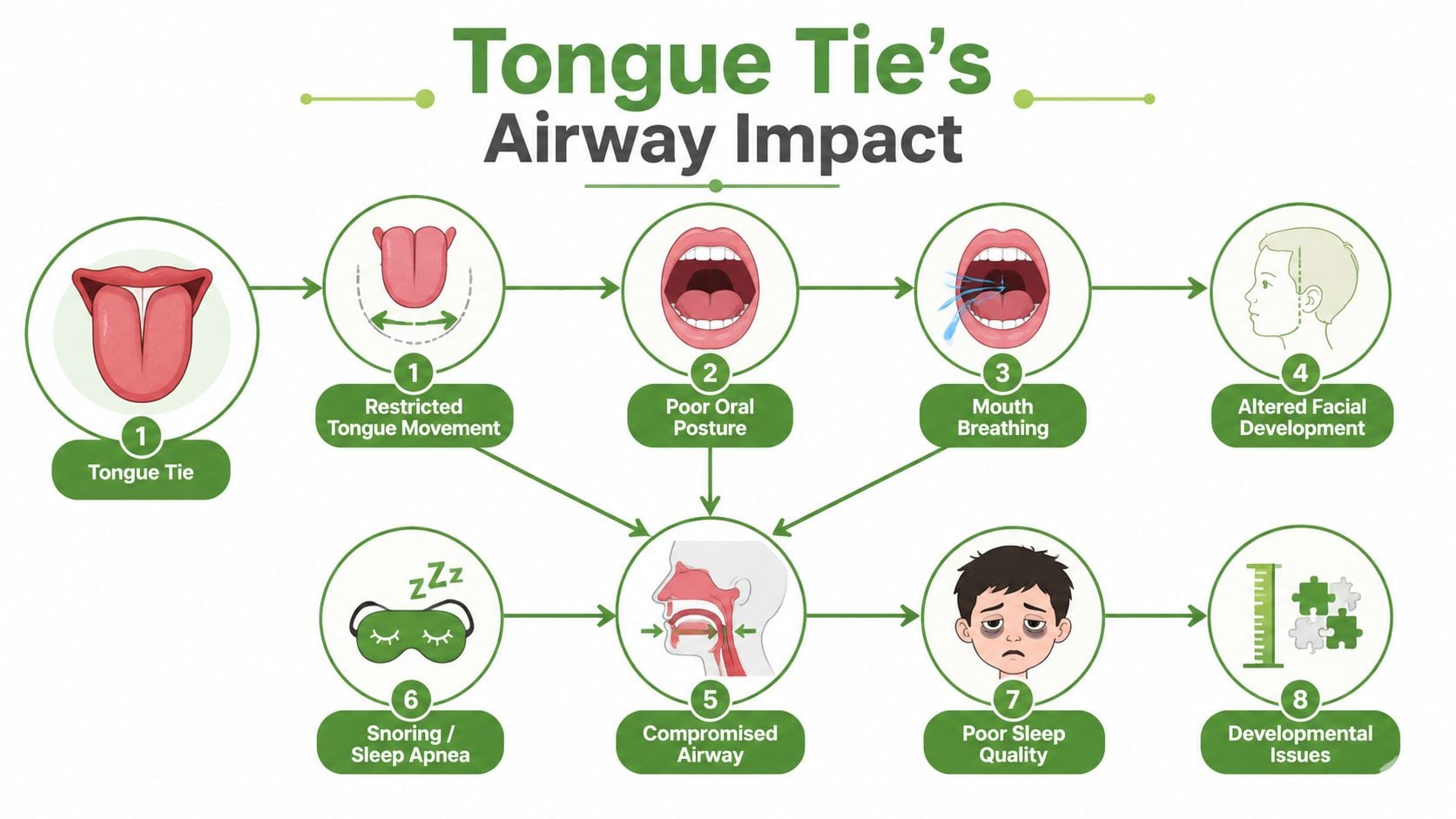
The chain often looks like this:
- Restricted tongue motion leads to low oral rest posture
- Low rest posture makes nasal breathing harder to maintain consistently
- Chronic mouth opening changes how the jaw and soft tissues behave
- A vulnerable airway during sleep contributes to snoring and sleep-disordered breathing
- Poor-quality sleep amplifies pain sensitivity, fatigue, and daytime dysfunction
Why this matters in both children and adults
In children, disrupted breathing can affect sleep quality, behavior, attention, and growth patterns. In adults, the same functional problems may show up as snoring, upper airway resistance, fragmented sleep, and obstructive sleep apnea. Not every person with a tongue tie develops a sleep disorder, but airway-focused clinicians ignore tongue posture at their own risk.
The tongue is not a bystander in sleep medicine. It helps determine whether the airway is supported or compromised.
For clinicians who want a broader procedural overview of airway management concepts, it's reasonable to explore advanced airway techniques as background. In everyday practice, though, the bigger point is simpler. The airway isn't just about the nose, tonsils, or throat. Oral posture matters.
When a sleep workup belongs in the conversation
A tongue tie evaluation should expand when any of these are present:
- Snoring or noisy sleep
- Frequent mouth breathing
- Dry mouth on waking
- Daytime fatigue despite adequate time in bed
- Morning headaches or jaw soreness
- Observed pauses, gasps, or restless sleep
If that pattern sounds familiar, an airway review may be warranted alongside oral functional care. Patients looking into the broader symptom picture can review sleep apnea causes and symptoms to see how disrupted breathing commonly presents outside the bedroom.
Getting a Proper Diagnosis What to Look For and Who to See
A proper tongue tie diagnosis doesn't start and end with someone lifting the tongue for two seconds and saying yes or no. It requires a functional assessment. That's true for infants, children, and adults.
The first question is not “Is there a frenulum?” The first question is “What is this tongue unable to do, and what is the body doing to compensate?”
What a meaningful evaluation includes
A thorough assessment usually looks at several layers at once:
- Mobility testing for elevation, extension, lateral movement, and tongue-palate contact
- Rest posture to see whether the tongue sits up or low in the mouth
- Swallow pattern to identify thrusting, jaw assistance, lip compensation, or neck recruitment
- Feeding or chewing function when the complaint involves nursing, bottles, or solids
- Speech movement patterns if articulation or fatigue with speaking is a concern
- Airway clues such as mouth breathing, snoring, or chronic open-mouth posture
A good evaluator also asks when the symptoms started and how they evolved. Infant latch trouble, childhood texture aversion, orthodontic crowding, adult clenching, and sleep complaints may all belong in the same timeline.
Who should be on the team
No single provider sees every piece equally well. The best care usually comes from a coordinated group.
- Lactation consultant or IBCLC for infant feeding assessment, latch mechanics, and milk-transfer concerns.
- Dentist or physician familiar with tethered oral tissues for diagnosis, procedural planning, and oral structural evaluation.
- Orofacial myofunctional therapist for rest posture, breathing, swallowing, and retraining patterns.
- Speech-language pathologist when articulation, oral motor planning, or feeding skills need deeper therapy support.
- Airway-focused providers when mouth breathing, snoring, or sleep-disordered breathing are part of the picture.
A quick procedure without a functional workup can leave the original problem only partly solved.
Red flags that deserve more than reassurance
A referral is worth pursuing when symptoms persist despite standard advice. Examples include ongoing painful feeds, poor transfer, recurrent clicking on the bottle or breast, chronic open-mouth posture, gagging with textures, speech effort, jaw tension, or sleep symptoms that don't fit a simple explanation.
The most helpful diagnosis connects structure to function. If the provider only describes what the frenulum looks like, the evaluation isn't finished yet.
Modern Treatment Release and Retrain for Lasting Results
Treatment works best when it respects two facts at the same time. First, restriction can be real. Second, the body may have spent months or years building compensation around it. That's why the most reliable approach is release and retrain, not release alone.
Release is one step, not the whole plan
A frenotomy or frenectomy aims to free tongue motion by releasing the restrictive tissue. When selected appropriately, it can improve access to movements that were previously blocked. But access isn't the same thing as skill.
Published clinical discussion suggests frenotomy is generally low risk, with an overall complication rate of about 1%, while moderate-to-severe complications were estimated at 13.9 per 100,000 infants in a national review. Reported issues can include poor feeding, pain, bleeding, and scarring, as summarized in this review of tongue tie release disadvantages and complications.
That risk profile is reassuring, but it doesn't support casual treatment. A release should be done for clear functional reasons, by an experienced provider, with follow-up when symptoms continue.
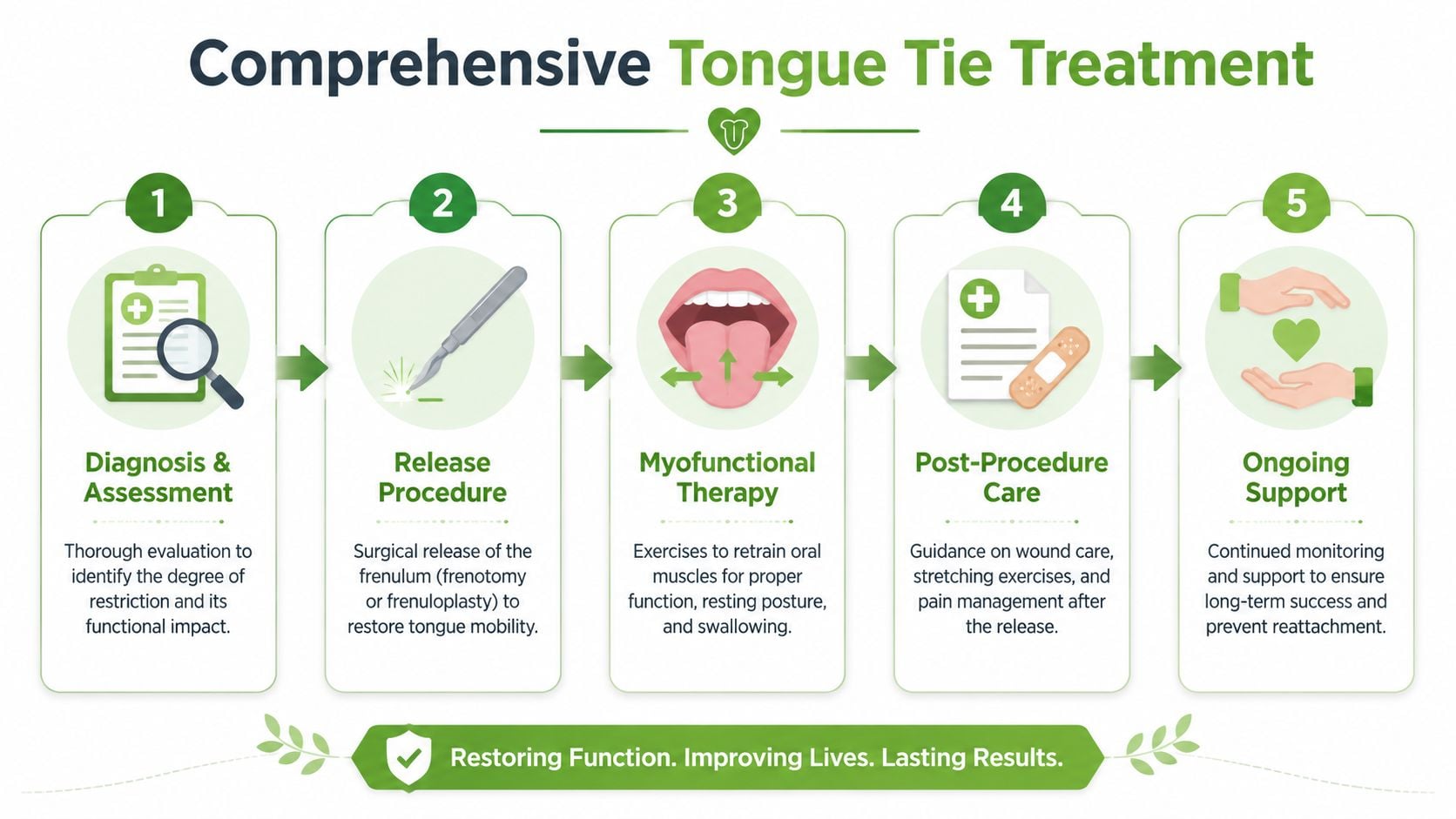
Retraining is where function changes
Once the restriction is reduced, the patient still has to learn how to use the tongue differently. That's the role of myofunctional therapy and structured follow-up. Think of it as physical therapy for the mouth and airway.
Retraining often targets:
- Tongue-to-palate rest posture
- Nasal breathing habits
- Efficient swallow mechanics
- Reduced jaw and lip compensation
- Wound care and movement practice during healing
This step matters because old movement patterns don't disappear automatically. A baby may still need feeding support after release. A child may still need speech or chewing therapy. An adult may need help unlearning clenching, low tongue posture, and maladaptive swallowing.
A simple clip versus a comprehensive plan
The difference is easy to summarize:
| Treatment style | What happens | Likely limitation |
|---|---|---|
| Procedure-only care | Restriction is released | Function may remain inefficient if patterns don't change |
| Integrated care | Release, exercises, feeding or therapy follow-up, airway review when needed | Requires coordination, but addresses the full problem |
For patients who need that rehabilitative piece explained in more detail, orofacial myology is the discipline focused on restoring oral posture, breathing, and swallowing patterns after release or alongside conservative care. One clinical option families may encounter is Pain and Sleep Therapy Center, which offers tongue tie evaluation, release, and myofunctional support within a broader TMJ and airway framework.
The right treatment plan doesn't chase anatomy alone. It restores function in a way the whole body can keep using.
If tongue tie complications may be affecting feeding, speech, jaw comfort, or sleep, Pain and Sleep Therapy Center offers evaluation focused on root-cause function rather than a quick visual check. The clinic works with infants, children, and adults to assess tongue mobility, oral posture, airway factors, and compensation patterns so families and referring providers can make informed next-step decisions.



