
Your baby is finally asleep. You can barely breathe through your nose. Your head feels packed with pressure, your mouth is dry from breathing all night, and the bottle of Afrin in the medicine cabinet suddenly looks like rescue.
Then the next thought hits. Can I use Afrin while breastfeeding, or will it affect my baby or my milk supply?
That concern is reasonable. New parents are often asked to weigh their own comfort against infant safety, even when they're sick, sleep-deprived, and trying to keep feeding on track. With Afrin and breastfeeding, the most useful question usually isn't a simple yes or no. It's this: what kind of medication is this, how much of it gets into your system, and what trade-offs matter most right now?
Afrin and Breastfeeding The Dilemma for New Parents
A common real-life scenario goes like this. A breastfeeding parent catches a cold, can't sleep because of nasal blockage, tries to push through for a day or two, then gets tempted by a fast-acting nasal spray. Relief matters. So does protecting feeding, especially if supply still feels fragile or the baby is nursing often.

That tension is part of early postpartum life. When breathing is poor, sleep gets worse. When sleep gets worse, pain, stress, and recovery often feel harder too. That's one reason broader support matters. If you're navigating healing, feeding, and body recovery at the same time, this overview of the benefits of timely postpartum care can be helpful.
Sometimes congestion concerns overlap with feeding mechanics too. If your infant seems to struggle at the breast beyond your temporary illness, it may help to look at common infant feeding problems separately from medication questions.
A miserable parent still deserves treatment. The goal is to choose the treatment with the lowest meaningful risk.
The reassuring part is that Afrin is not in the same category as many oral cold medicines. That difference is what drives most of the guidance. Once you understand why, the recommendations make a lot more sense and feel less arbitrary.
Understanding Afrin A Local Fix Not a Systemic Drug
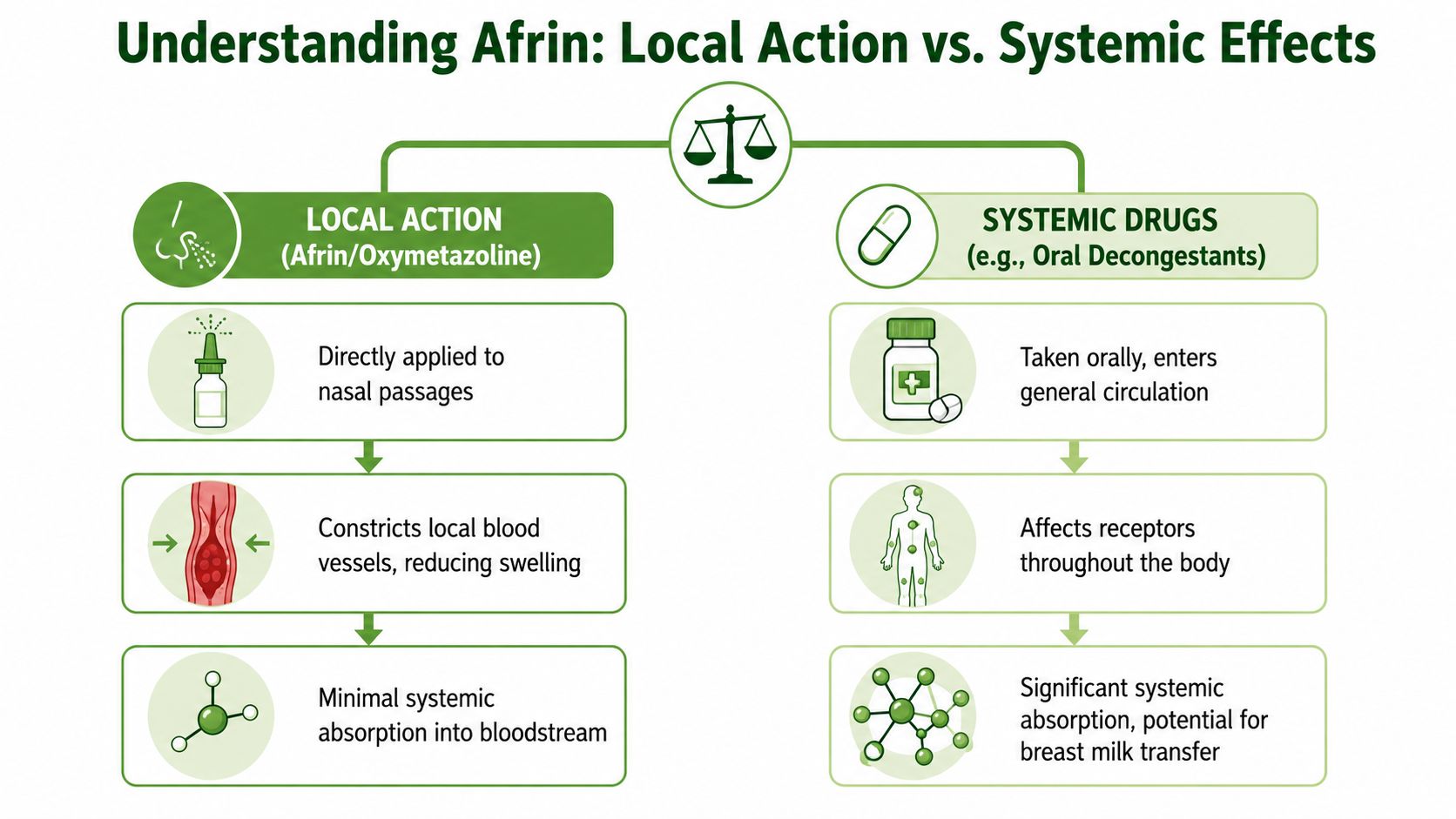
Afrin's active ingredient is oxymetazoline. It's a topical nasal decongestant, which means you spray it directly where the swelling is. That sounds simple, but it's the key reason its breastfeeding risk profile is different from pills such as pseudoephedrine.
Why local treatment matters
Think of the difference this way. A pill is like putting dye into a whole swimming pool. It circulates everywhere. A nasal spray like Afrin is more like watering one specific plant. Some of it may still get beyond the target area, but much less reaches the rest of the body.
That concept is called systemic absorption. The less medication that reaches the bloodstream, the less is available to move into breast milk.
LactMed notes that oxymetazoline has very limited systemic absorption and says “very little should reach the infant through breastmilk” because it is locally administered and only minimally absorbed into maternal blood, making it preferable to oral systemic decongestants during lactation, as summarized in the National Library of Medicine LactMed entry on oxymetazoline.
Why this principle shows up across breastfeeding medicine
This isn't unique to Afrin. In breastfeeding care, clinicians often look first at route of administration. A medicine used on the skin, in the nose, or as a local anesthetic often behaves very differently from a swallowed medication.
The same general principle appears elsewhere in family medicine. The American Academy of Family Physicians notes that topical and local anesthetics may be used safely in breastfeeding, and it also lists ibuprofen and acetaminophen as preferred analgesics because they fit a lower-risk exposure profile for lactation.
A short video may help if you want a visual explanation of nasal breathing and congestion management:
What Afrin actually does
Afrin constricts swollen blood vessels in the nasal passages. That reduces tissue swelling and can open the airway quickly. For a parent who hasn't slept and just wants to breathe, that speed is the appeal.
But fast relief isn't the whole story. Afrin works best as a short-term tool, not an all-purpose answer for every type of congestion.
Does Afrin Get Into Breast Milk What the Research Says
The best available answer is careful rather than absolute. Direct breastfeeding studies on oxymetazoline are limited, so no responsible clinician should pretend there's perfect milk-level data. Even so, the practical conclusion is still fairly reassuring because the drug is used locally and not absorbed much into the bloodstream.
That's why many lactation recommendations favor Afrin over oral decongestants when a breastfeeding parent needs short-term nasal relief. The logic is pharmacologic, not casual. If very little medication enters maternal circulation, very little is available to enter milk.
The risk many parents miss
With decongestants, the most clinically important problem often isn't infant exposure. It's milk-supply suppression.
The British Breastfeeding Network notes that oral decongestant tablets, powders, and drinks should be avoided because they can significantly affect supply, while nasal sprays containing xylometazoline or oxymetazoline are considered effective and do not cause wakefulness nor reduce milk supply, as explained in its guidance on decongestants during breastfeeding.
That changes the conversation. Many parents spend all their energy worrying about whether a medicine will reach the baby, when the more immediate issue may be whether the medicine interferes with breastfeeding itself.
When I counsel families on Afrin and breastfeeding, I frame the decision around the real-world risk. For most short-term users, the bigger concern is not milk transfer. It's choosing the wrong decongestant category.
What that means in practice
If your choices are an oral systemic decongestant versus a brief course of topical oxymetazoline, the topical option usually makes more sense for breastfeeding. It targets the nose rather than the whole body.
Still, “lower risk” doesn't mean “use freely.” Afrin can solve one problem and create another if it becomes a habit. The main complication is rebound congestion, which is a local nose problem rather than a breast milk problem.
Safer Alternatives for Relief While Breastfeeding
Afrin can be useful, but it shouldn't be the only tool in the conversation. The better question is often: what level of treatment matches the kind of congestion you have? A stuffy nose from a short viral illness isn't the same as chronic allergy, sinus irritation, or ongoing mouth breathing.
Start with the lowest-risk options
For many breastfeeding parents, the first step is simple support that doesn't rely on medication at all.
- Saline spray or saline rinse can loosen mucus and moisten irritated nasal tissue.
- Humidified air may make nighttime breathing more comfortable when the room is dry.
- Steam from a shower can give short bursts of relief, especially before sleep.
- Hydration and rest won't instantly decongest the nose, but they support recovery and feeding better than pushing through exhaustion.
If congestion is tied to poor breathing habits, ongoing mouth breathing, or upper airway irritation, targeted breathing exercises for nasal congestion can also help some people reduce that sense of constant blockage.
When short-term relief is the main goal
Afrin fits here. It's a targeted option for severe blockage when you need to sleep, feed, or function. The limitation is duration. It's not a good long-term maintenance strategy.
For aches, fever, or general cold discomfort that comes along with congestion, the American Academy of Family Physicians notes that ibuprofen and acetaminophen are preferred analgesics in breastfeeding, and it also emphasizes that topical and local anesthetics may be used safely in breastfeeding, which reinforces the same route-and-absorption principle used in medication decisions for nursing parents, in the AAFP review on medication safety in breastfeeding.
When symptoms keep dragging on
If you need ongoing treatment beyond brief rescue relief, steroid nasal sprays are often the more logical category to discuss with your clinician. Mayo Clinic notes that these can be used longer term, while Afrin is for short-term relief only. That's an important distinction because many people don't have a one-night problem. They have recurring congestion.
Here's a practical comparison:
| Option | How It Works | Breastfeeding Safety | Best For |
|---|---|---|---|
| Saline spray or rinse | Moistens nasal passages and helps clear mucus | No medication exposure concern | Dryness, mild congestion, frequent use |
| Humidifier or steam | Loosens secretions and soothes irritated tissues | No medication exposure concern | Temporary comfort, bedtime relief |
| Afrin (oxymetazoline) | Shrinks swollen nasal blood vessels locally | Generally favored over oral decongestants for short-term use because exposure is expected to be low | Severe short-term blockage |
| Steroid nasal spray | Reduces nasal inflammation over time | Often a better option to discuss for longer-duration symptoms | Allergy or persistent inflammatory congestion |
| Oral decongestant products | Work through systemic circulation | Less appealing in lactation because supply effects matter | Usually not first choice while breastfeeding |
Practical rule: If the problem is temporary and intense, a local rescue option may be enough. If the problem keeps returning, think beyond Afrin and ask what's driving the congestion.
Practical Tips for Using Afrin Safely
If you and your clinician decide Afrin makes sense, use it like a short-term bridge, not a daily solution.
The main rule
The biggest practical danger with Afrin is rebound congestion. Your nose can start to feel more blocked when the spray wears off, which pushes you to use it again. That cycle is what causes trouble.
For many patients, basic nasal mechanics matter just as much as medicine. Learning how to breathe through your nose can make short-term relief strategies work better and reduce the urge to keep reaching for spray after spray.
A safer way to use it
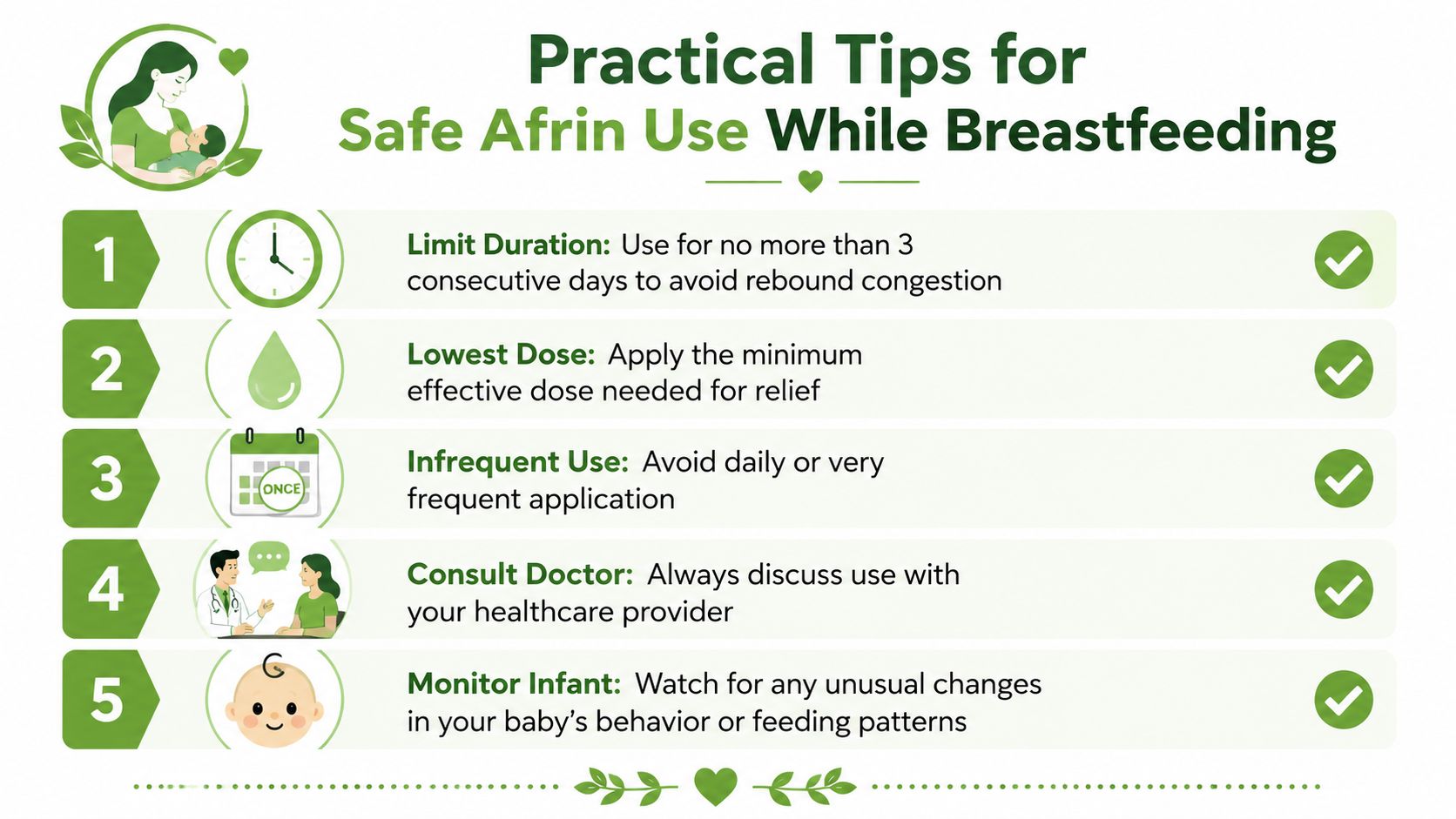
- Keep it brief. Don't stretch Afrin into an ongoing routine. If you feel you need it beyond a short window, the plan needs to change.
- Use the minimum that works. More spray doesn't create a healthier result. It mainly increases the chance you'll lean on it.
- Time it strategically. Many parents prefer using it right after a feeding so there's more time before the next nursing session.
- Watch your pattern. If your nose seems to “need” Afrin every day, that's a warning sign for rebound rather than healing.
- Avoid switching to oral decongestants casually. Independent breastfeeding guidance reports that oral decongestants can reduce milk supply even after a single dose, while LactMed states oxymetazoline is preferred over oral pseudoephedrine during breastfeeding because very little should reach the infant through milk, and the British Breastfeeding Network says oxymetazoline nasal sprays are effective and should not reduce milk supply when used briefly, as summarized in this breastfeeding guidance on decongestants and breastfeeding.
When to Seek Professional Medical Advice
Some situations deserve more than self-treatment. If your congestion doesn't improve, keeps returning, or seems tied to allergy, sinus infection, chronic mouth breathing, or sleep disruption, it's time to ask for a more personalized plan.
Call sooner in these situations
- Your baby is especially vulnerable. Mayo Clinic notes that medication exposure through milk matters most for premature babies, newborns, and infants with kidney or other health issues, as discussed in its review of breastfeeding and medications.
- You notice feeding changes. If your baby seems unusually sleepy, irritable, or feeds differently after you start a medication, check in.
- You think your milk supply has shifted. Even if Afrin itself isn't the likely cause, any supply concern in early lactation deserves attention.
- You can't stop using the spray. That often points to rebound congestion or an untreated underlying issue.
What to ask your clinician
Bring the actual product name and active ingredient. Ask whether your congestion sounds viral, allergic, or structural. Ask whether a longer-term option makes more sense than repeated Afrin use.
That conversation is especially worthwhile if you're caring for a newborn and trying to protect sleep, feeding, and recovery at the same time.
If nasal blockage, mouth breathing, poor sleep, TMJ tension, or airway-related symptoms keep showing up in your life, Pain and Sleep Therapy Center offers evaluation focused on root causes, not just temporary symptom relief. Their team helps adults and families look at breathing, sleep, oral posture, and related pain patterns in a more complete way.



