
You may be reading this because a dentist told you to “just watch” your wisdom teeth, while a friend told you to remove all four immediately, and now your jaw already feels tight when you wake up. Or maybe the teeth are out, the gums look healed, and yet your bite feels off, your temples ache, or your sleep has gotten worse.
That confusion is common. Most advice about the wisdom teeth timeline focuses on one event, the extraction. Real life is broader. Wisdom teeth begin developing long before they show up, and their effects can continue long after the sockets close.
A complete timeline includes growth inside the jaw, eruption or impaction in the late teen years, the decision about monitoring versus removal, early healing after surgery, and the longer period when the jaw muscles, bite, airway, and sleep patterns adapt. That last part gets missed far too often.
Wisdom teeth are not just a tooth problem. In the right patient, they can contribute to gum inflammation, crowding, bite changes, jaw guarding, headaches, facial pain, and sleep disruption. In other patients, removal helps. In some, it solves one issue but uncovers another that was already brewing under the surface.
Clinical reality: A mouth can look “healed” before the jaw system feels normal again.
That’s why the most useful approach is root-cause thinking. Instead of asking only, “When do wisdom teeth come in?” or “How long is recovery?” ask better questions. Is there enough space? Is the joint already overloaded? Is muscle tension building? Is nasal breathing poor? Is sleep quality changing?
Your Complete Wisdom Teeth Timeline From Growth to Recovery
The full wisdom teeth timeline starts years before pain. Third molars begin as developing structures deep in the jaw during childhood, then typically try to erupt in late adolescence or early adulthood. For some people they emerge uneventfully. For many others, they become trapped, partly erupt, or press into neighboring teeth.
That matters because wisdom teeth problems rarely stay isolated. A partially erupted tooth can trap debris and inflame the surrounding gum. An impacted tooth can affect the tooth in front of it. A sore back molar can also change how a person chews, clenches, or holds the jaw.
The timeline is bigger than surgery
A practical way to think about it is in stages:
Development inside the jaw
Wisdom teeth form before you can see them. During this phase, imaging often gives the first clue about whether there’s enough room.Eruption or impaction
In the late teens and early twenties, the tooth may come in normally, partly break through the gum, or stay stuck in bone or soft tissue.Decision-making
Good care matters during decision-making. Some people need monitoring. Others need removal because the tooth is damaging gum, bone, or the neighboring molar.Initial recovery
After extraction, the visible healing begins. Bleeding settles, swelling rises and falls, and the gum gradually closes.Functional recovery
This stage is easy to overlook. The jaw muscles, bite pattern, and sleep posture may need more time to settle, especially if there was pre-existing TMJ strain.
What works and what doesn't
What works is early evaluation, thoughtful imaging, and attention to symptoms beyond the tooth itself. What doesn’t work is treating every case as routine, or assuming that once the extraction site closes, the problem is over.
If your jaw already clicks, locks, aches, or feels tired when chewing, your wisdom teeth timeline deserves a wider lens. The same is true if snoring, mouth breathing, or unrefreshing sleep started around the same period as eruption or recovery.
How Wisdom Teeth Develop and Erupt
Wisdom teeth are your third molars, and they’re the last permanent teeth to arrive. Their development starts long before they become visible. In childhood, they begin as tooth buds within the jawbone. Over time, the crown forms, roots develop, and the tooth slowly moves toward the surface.
Individuals often first hear about wisdom teeth when a panoramic X-ray shows them angling forward, sitting sideways, or lingering under the gums. That’s often the first sign that the eruption path may not be straightforward.
When they usually appear
Wisdom teeth typically erupt between ages 17 and 21, and if they haven’t erupted by age 25, they generally remain impacted, according to this overview of wisdom tooth eruption and impaction. The same source notes that about 80% of young adults have at least one wisdom tooth retained within the jaw.
Those numbers explain why so many late teens and young adults get mixed messages. Wisdom teeth are common. Trouble with wisdom teeth is also common. But “common” doesn’t mean every case should be handled the same way.
The crowded party problem
A simple analogy helps. Wisdom teeth are like late arrivals to a crowded party. By the time they try to enter, the room is already full. The first and second molars are in place. The jaw has largely matured. If space is limited, those last molars don’t slide in neatly. They lean, twist, stay half-covered by gum, or remain buried.
That space problem is tied to human evolution. Modern jaws are often smaller than those of earlier ancestors, while the total number of teeth hasn’t changed in the same way. The result is a mismatch between tooth count and available room.
Wisdom teeth often aren't “bad teeth.” They’re teeth trying to erupt into a jaw that may not have enough space left for them.
What eruption can look like
Not every wisdom tooth behaves the same way. Common patterns include:
Normal eruption
The tooth comes in upright, meets a partner tooth, and can be cleaned.Partial eruption
Part of the tooth breaks through the gum, but a flap of tissue remains over it. This setup often irritates the gum and traps food.Impaction
The tooth stays stuck against bone, gum, or the tooth in front of it.Asymmetry
One may erupt while another stays trapped. Upper and lower teeth don't always follow the same schedule.
What matters most isn’t just whether the tooth erupts. It’s whether it erupts functionally, without damaging neighboring structures or triggering inflammation that spills over into the rest of the jaw system.
Common Signs That Point to Wisdom Tooth Removal
A wisdom tooth doesn’t need removal just because it exists. It needs serious attention when it starts creating a clear biological problem. The challenge is that the first signs are often brushed off as “normal teething” or temporary soreness.

Pain is one clue, but not the only one. In practice, the more important question is whether the wisdom tooth is creating a pattern of recurring inflammation, structural damage, or functional strain.
Signs that deserve prompt evaluation
Look for these patterns:
Repeated gum swelling behind the last visible molar
This often happens when a tooth is only partly erupted and the tissue around it keeps getting irritated.Pain with chewing or wide opening
Back-tooth inflammation can make people shift their bite or tighten the jaw muscles without realizing it.Bad taste, trapped food, or difficult cleaning
These are common with partially erupted teeth, especially when a gum flap holds debris.Pressure on the tooth in front
Impacted wisdom teeth can push against the second molar and create damage that isn’t easy to see without imaging.Jaw stiffness or one-sided chewing
A sore wisdom tooth often changes how the muscles work. Over time, that can feed into TMJ irritation.
Why impacted teeth aren't harmless
Impacted wisdom teeth can tilt the neighboring second molar forward, called mesial inclination, which increases the risk of periodontitis by 2 to 4 times because plaque is easier to retain, based on Cleveland Clinic’s explanation of impacted wisdom teeth and extraction complexity.
That’s one of the reasons “wait until it really hurts” isn’t always a wise strategy. Some damage develops unnoticed. The tooth in front may carry the burden long before the wisdom tooth becomes dramatically painful.
For a balanced discussion of when removal is necessary and when monitoring may be reasonable, this guide on whether everyone needs their wisdom teeth removed is useful.
Removal is a treatment decision, not a reflex
There’s a difference between a fully erupted tooth that can be cleaned and an impacted tooth that threatens the neighboring molar. There’s also a practical difference in the procedure. According to the same Cleveland Clinic source, simple extractions for erupted teeth may take 15 to 30 minutes, while impacted cases can take 45 to 90 minutes and may require incisions and bone removal.
Decision point: Remove wisdom teeth because they’re causing current harm or have a strong likelihood of causing it. Don’t remove or retain them on autopilot.
A patient with recurring gum infections, progressive damage to the second molar, or increasing jaw compensation usually needs action. A patient with symptom-free, cleanable, well-positioned wisdom teeth may need observation instead. Good care means separating those groups carefully.
Your Hour-by-Hour Wisdom Tooth Recovery Timeline
At 2 a.m., the pattern is familiar. A patient wakes with a throbbing jaw, sleeps propped up on pillows, and is not sure whether the pressure, stiffness, and ear-area ache are normal healing or the start of a bigger problem. That uncertainty is one reason a clear recovery timeline matters. After wisdom tooth removal, the socket heals on one schedule, while the jaw muscles, bite, and sleep quality can follow another.
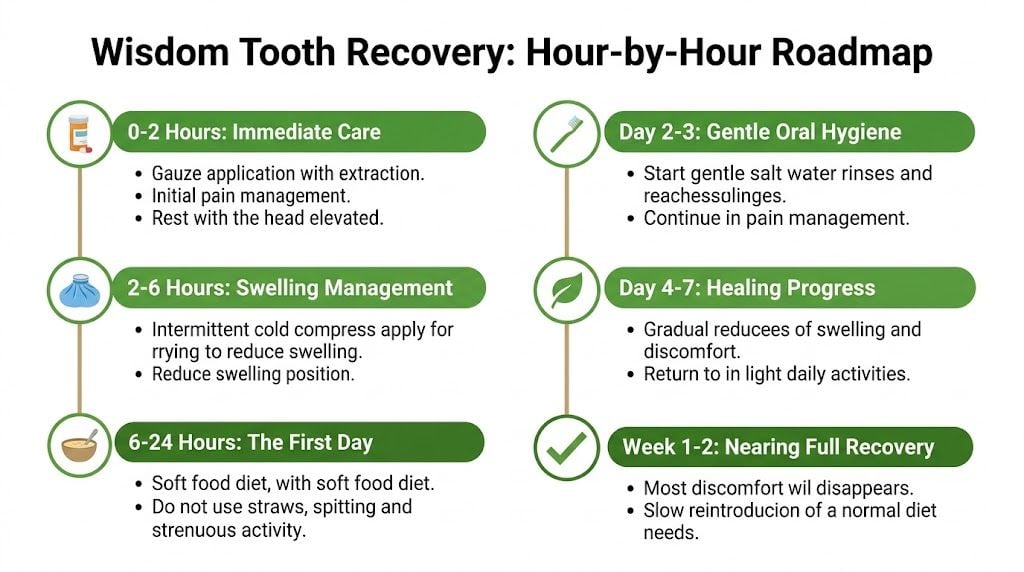
Hours 0 to 24
The first day is about protecting the blood clot and keeping inflammation from escalating. The clot covers the extraction site and gives the body a stable base for repair. If that clot gets disrupted early, pain usually rises fast and recovery gets harder.
Keep activity light. Take medications exactly as prescribed. Avoid anything that creates suction or repeated pressure in the mouth.
A good first-day checklist looks like this:
Protect the clot
Bite on gauze as directed. Avoid straws, spitting, forceful rinsing, and smoking.Get ahead of swelling
Use ice during the early post-op period if your surgeon recommended it.Choose foods that do not disturb the site
Yogurt, applesauce, lukewarm soups, mashed foods, and smoothies without a straw are common early options.Keep your head raised
That often helps with pressure and overnight comfort.Limit jaw strain
Long conversations, wide yawning, heavy chewing, and daytime clenching can aggravate sore muscles around the TMJ.
If you want extra practical guidance on managing wisdom tooth removal pain, that resource gives a patient-friendly overview that fits well with standard post-op instructions.
Days 2 to 7
This is often the hardest stretch. Swelling usually peaks around 48 hours after surgery, according to this detailed healing timeline for wisdom tooth sockets. Day two can feel worse than day one, even when healing is on track.
Jaw stiffness often shows up here too. Some of that comes from swelling. Some comes from muscle guarding after keeping the mouth open during the procedure. In patients who already clench, grind, or have TMJ tenderness, that guarded pattern can spill into the temples, cheeks, ears, and even the neck. Sleep can suffer for the same reason. People wake more often when they cannot find a comfortable jaw position.
Oral hygiene needs a careful restart during this window. The goal is cleanliness without disturbing the socket.
What usually improves during the first week
By about the one-week mark, the sharpest edge of recovery has usually passed. The same source notes that sutures are often ready for removal around this stage, and pain is commonly much more manageable with NSAIDs. That does not mean the jaw is fully settled. It means the tissue injury is calming down.
| Time period | What usually feels normal | What deserves a call |
|---|---|---|
| Day 1 | Oozing, numbness wearing off, soreness | Bleeding that does not settle |
| Day 2 to 3 | Peak swelling, limited opening, fatigue | Pain that worsens, foul taste, bad odor, fever, or trouble swallowing |
| Day 4 to 7 | Gradual easing of swelling and soreness | Pain increasing instead of easing, worsening jaw lock, or new asymmetry in opening |
One practical point gets missed here. A socket can be healing normally while the jaw is still overworking. If chewing shifts to one side, if you start waking with clenched teeth, or if ear pressure and temple pain are replacing tooth pain, the problem may be muscular and joint-related rather than infectious.
Weeks 2 to 4
By this point, the mouth often looks better than it feels. The same source explains that the socket commonly fills with granulation tissue during weeks two to three. That is normal repair tissue.
Patients usually start testing more foods during this period, and that is where setbacks happen. The gums may appear closed enough for regular eating, but deeper tissues still do not like forceful chewing, hard edges, or constant pressure from crunchy foods. For meal ideas that are less likely to irritate healing sites, this guide on foods to eat after wisdom teeth removal can help.
This is also the stage when hidden compensation patterns stand out. If the bite feels off, if one side of the face gets tired faster, or if headaches show up at night, do not assume it is just part of healing. Sometimes the extraction solved the dental problem, but exposed an underlying jaw-joint or airway issue that had been simmering in the background.
Weeks 6 to 8 and beyond
The gum surface can look healed before the deeper repair work is finished. Full epithelial closure is achieved by about weeks 6 to 8, as noted earlier. Dry socket can also prolong recovery if the clot breaks down too soon.
Red flag: Pain that intensifies after an initial improvement needs attention. Normal recovery trends downward.
I tell patients to judge recovery by function, not only by appearance. Can you chew without guarding? Can you open comfortably? Are you sleeping through the night without jaw tension, facial pressure, or waking with soreness? Those answers matter because wisdom tooth recovery does not end at gum closure. In some patients, the lasting issue is not the extraction site. It is the strain the surgery revealed in the TMJ, facial muscles, and nighttime breathing pattern.
Beyond Recovery The Hidden Link to TMJ and Chronic Pain
The part most patients never get warned about is this. A wisdom tooth can be gone, the gum can look healed, and the jaw can still be in trouble.

That happens because the extraction is only one event inside a larger mechanical system. During healing, people often chew differently, clench more, keep the mouth from opening fully, or tense the neck and face to protect the area. Those compensations can outlast the dental wound.
How the jaw gets pulled into the process
Several pathways can drive post-extraction TMJ problems:
Muscle guarding
Sore tissue leads people to brace the jaw. That can overload the masseter, temporalis, and pterygoid muscles.Bite adaptation
Swelling or altered chewing can make the bite feel “off,” even if the teeth themselves are fine.Joint sensitivity
If the TMJ was already unstable, inflamed, or overloaded, surgery can aggravate symptoms that were previously mild.Nerve irritation
Some patients develop a persistent ache pattern that feels broader than tooth pain alone.
According to this discussion of wisdom tooth recovery and TMJ complications, up to 25% of wisdom tooth removal patients may develop TMJ disorders, and the risk is 2 to 3 times higher for adults over 25. The same source notes that myofascial tension can emerge weeks 2 to 6 post-op, which fits what many patients report when the initial swelling has faded but facial tension is building.
Symptoms people often mislabel as “normal healing”
These signs deserve a closer look if they persist:
- Temple headaches that started after recovery
- Jaw clicking or catching that wasn't there before
- Pain near the ear when chewing
- Morning facial fatigue or clenching
- Neck tension linked with bite discomfort
For readers trying to sort out whether their symptoms sound like a joint problem rather than routine soreness, this article on how to know if you have TMJ disorder offers a helpful symptom framework.
If the pain pattern has moved beyond the tooth and into the muscles, joints, or nerves of the face, a broader understanding of orofacial pain becomes important.
Recovery of the socket and recovery of the jaw are not always the same timeline.
What doesn’t work is repeatedly telling patients that everything is fine because the extraction site looks closed. What works is evaluating the whole functional picture: bite loading, jaw range of motion, muscle tenderness, headache pattern, and whether sleep quality changed along the way.
How Wisdom Teeth Impact Airway Breathing and Sleep
Wisdom teeth and sleep aren’t usually discussed together, but they should be. The back of the mouth is shared territory. Teeth, tongue posture, soft tissue, and jaw position all influence how comfortably a person breathes, especially during sleep.
In some patients, impacted wisdom teeth add to posterior crowding. According to this review of delayed sleep concerns after wisdom tooth removal, impacted wisdom teeth can be a factor in 30 to 50% of Obstructive Sleep Apnea cases due to airway crowding. That doesn’t mean wisdom teeth are the only cause of disordered breathing. It means they can be one part of a crowded, poorly functioning system.
Why sleep symptoms may change after removal
The same source notes that removal can initially improve breathing, but 15 to 20% of patients experience rebound TMJ strain affecting sleep posture by month 3 if underlying issues like poor nasal breathing aren’t addressed. These considerations reveal shortcomings in the standard dental timeline.
A patient may report that snoring improved for a short period after surgery, then jaw tightness crept in, side sleeping became uncomfortable, and fatigue returned. That pattern makes sense when jaw mechanics and airway function are linked.
Clues that the airway deserves attention
Consider a broader evaluation if any of these show up around your wisdom teeth timeline:
- Snoring that starts or worsens
- Mouth breathing during sleep
- Waking with a dry mouth or sore jaw
- Morning headaches
- Fatigue that doesn’t match your time in bed
These aren’t always “just stress” or “just healing.” Sometimes they point to a system under strain. A crowded posterior mouth, low tongue posture, poor nasal breathing, and jaw guarding can all reinforce one another.
A patient can recover from surgery and still sleep poorly if the underlying breathing pattern and jaw posture never stabilize.
What works is connecting the dots early. If a person already has airway concerns, chronic congestion, clenching, or facial pain before wisdom tooth treatment, those details should shape the plan. Monitoring sleep-related symptoms for months, not just days, often reveals the actual outcome.
Next Steps for a Healthy Jaw and Restful Sleep
A good wisdom teeth timeline doesn’t end when the stitches come out. It ends when the mouth is stable, the jaw is functioning comfortably, and sleep hasn't been compromised in the process.
That means looking beyond the tooth. If you’re deciding whether to remove wisdom teeth, ask whether there’s enough space, whether the neighboring molar is at risk, and whether your jaw already shows signs of strain. If your teeth are already out, ask a different set of questions. Has your bite changed? Are your muscles staying tight? Are headaches, clicking, or sleep problems showing up after the dental site healed?
When a deeper evaluation makes sense
Seek more specialized follow-up if you notice:
- Persistent jaw pain after the gums look healed
- Clicking, locking, or limited opening
- Temple headaches or facial tension that appeared after surgery
- Snoring, mouth breathing, or morning fatigue that worsened around recovery
- A sense that your bite never settled back to normal
What tends to help
Root-cause care is usually more effective than chasing one symptom at a time. That may include CBCT imaging when anatomy needs closer evaluation, PRF when tissue healing or inflammation remains a concern, and orofacial myofunctional therapy when oral posture, swallowing, or breathing mechanics are contributing to ongoing dysfunction.
The key is timing. The earlier you identify whether the problem is dental, muscular, joint-related, airway-related, or a mix of all four, the easier it is to avoid a long cycle of partial fixes.
If your wisdom teeth timeline has turned into jaw pain, headaches, facial tension, snoring, or poor sleep, Pain and Sleep Therapy Center offers the kind of deeper evaluation many patients need. Their team focuses on TMJ disorders, orofacial pain, airway breathing, and sleep-related issues with a root-cause approach that may include advanced imaging, regenerative options, and personalized therapy plans to help you move beyond “the tooth is out” and toward lasting comfort.



