
You wake up with a headache that feels bigger than “just stress.” Your jaw is tight. Your teeth may feel sore. Maybe your temple throbs by lunch, and by evening you're wondering whether this is a migraine, a sinus issue, a neck problem, or something dental.
That confusion is common.
A lot of people search for treatment for TMJ migraines after trying pain relievers, massage guns, soft foods, nightguards bought online, or migraine remedies that only partly help. The problem is that jaw-related pain and migraine can overlap so closely that it's easy to treat the wrong thing, or to miss that both are happening at the same time. Relief usually starts when the diagnosis gets more precise.
The Hidden Connection Between Your Jaw and Headaches
The jaw and the head don't operate as separate systems. They share anatomy, muscles, and nerve pathways. When the jaw joint and surrounding muscles become irritated, the pain can travel into the temples, face, behind the eyes, and into the neck. For some people, that jaw irritation can feed into migraine pathways rather than staying “local” to the joint.
A useful way to think about it is a faulty electrical circuit. One overloaded line doesn't just affect one room. It can trigger surges elsewhere. In the same way, a problem in the temporomandibular joint, the chewing muscles, or clenching patterns can aggravate the broader pain network that also drives migraine symptoms.
Why this overlap matters
This isn't a minor issue. A major clinical study published in 2025 found that patients with temporomandibular disorder who also had migraine symptoms had higher disability and psychological distress than TMD patients without migraine symptoms, which points to a heavier overall disease burden in the overlap group (clinical study on TMD and migraine burden).
That finding matches what many specialists see in practice. When jaw pain and migraine coexist, patients often feel like they're chasing symptoms instead of solving a pattern.
Clinical takeaway: If your headaches keep returning and your jaw is tight, sore, clicking, or tired, it's reasonable to ask whether the jaw is participating in the pain cycle, not just reacting to it.
There's another reason this matters. People often experiment with home remedies for facial pain before they get a proper diagnosis. Some can be harmless. Some can distract from the root cause. If you're curious how folk approaches get interpreted in dental pain, this look at the science behind garlic and tooth pain is a good example of why symptom relief and root-cause care aren't always the same thing.
Clenching is one of the most common pieces of the puzzle. If that sounds familiar, this overview of headaches caused by jaw clenching explains how muscle overload in the jaw can spill into temple and head pain.
Getting the Right Diagnosis for Lasting Relief
The biggest mistake in TMJ-related headache care is assuming every jaw-associated headache is the same. It isn't. Some people have migraine with jaw tension. Some have TMD-referred pain that feels like a migraine. Some have both, and those patients usually need a blended plan.
Most online advice skips that distinction. It jumps straight to “wear a splint” or “take an anti-inflammatory.” That can delay the right care.

What a careful differential diagnosis looks for
A thorough evaluation usually includes:
- Pain pattern: Where the pain starts, where it spreads, how long it lasts, and whether it's linked to chewing, waking, stress, menstrual cycles, light sensitivity, or nausea.
- Jaw function: Clicking, popping, locking, limited opening, deviation, or pain with chewing.
- Muscle findings: Tenderness in the masseter, temporalis, neck, and related facial muscles.
- Behavioral clues: Clenching, grinding, nail biting, gum chewing, side sleeping pressure, or daytime jaw bracing.
- Headache features: Whether symptoms fit classic migraine more than referred jaw pain.
Quick self-check questions
These questions don't diagnose you, but they help frame the conversation:
- Does chewing make the headache worse? That leans more toward a jaw contribution.
- Do you wake up with facial tightness or tooth soreness? Overnight clenching may be involved.
- Do light, sound, or nausea come with the headache? That raises the index of suspicion for migraine features.
- Does pressing on your temple or jaw muscles reproduce the pain? Referred muscular pain is possible.
- Are you taking pain relievers frequently? That can complicate the picture.
An important gap in patient education is the risk of misclassification. Mayo Clinic's patient guidance highlights that most existing content on “TMJ migraine” treatment focuses on simple fixes, but rarely explains the risk of treating the wrong headache syndrome or of medication overuse when jaw pain and migraine overlap (Mayo Clinic guidance on TMJ diagnosis and treatment).
Some medications can help both jaw pain and migraine, but they aren't used the same way. If you self-treat too often without clarifying the diagnosis, you can make the headache pattern harder to untangle.
What to expect at a specialist visit
A useful consultation should include hands-on examination, not just a quick glance. The clinician should check jaw range of motion, palpate the chewing muscles, look at bite strain patterns, ask about sleep and stress, and decide whether imaging or referral is needed.
That visit should also answer a practical question: Are we treating a primary migraine disorder, TMD-referred pain, or a mixed case? If that answer stays vague, the treatment plan usually stays vague too.
Building a Foundation with Conservative Treatments
For most patients, the best early strategy isn't one magic tool. It's combined conservative care. In patients who have both migraine and temporomandibular disorder, the most evidence-aligned approach is a combination of custom oral appliances or splints, trigger-avoidance, and physical therapy with home stretching and exercises used together (combined conservative care for comorbid migraine and TMD).
That matters because jaw pain usually has more than one driver. Muscle overload, joint strain, airway issues, posture, clenching habits, and central pain sensitivity can all contribute. A plan that addresses only one of those often stalls.
Splints help when they're designed for your bite and diagnosis
A custom oral appliance isn't the same as a generic boil-and-bite guard. The goal isn't just to put plastic between the teeth. A well-designed appliance can reduce overload on the jaw system, protect teeth from grinding forces, and give irritated muscles a chance to settle.
But splints aren't “always yes.” The wrong design, wrong fit, or wrong wear schedule can create new problems. They work best when prescribed for a specific reason and followed closely.
Physical therapy treats mechanics, not just pain
Physical therapy is often where patients start noticing how connected the jaw is to the neck, shoulders, tongue posture, and breathing pattern. Good TMJ-focused therapy usually includes mobility work, gentle stretching, soft tissue treatment, posture correction, and a home program.
Consistency matters more than intensity. Tiny daily corrections often outperform aggressive self-treatment.
If you want a safe starting point for movement-based care, these TMJ headache relief exercises can help you understand the kind of controlled mobility work clinicians often recommend.
What usually works best: A splint without exercises may protect the teeth but leave the muscles dysfunctional. Exercises without habit correction may help briefly but not hold. Combining approaches is usually more durable.
Functional retraining often gets overlooked
Some patients keep relapsing because the underlying habit loop never changes. Mouth breathing, low tongue posture, poor swallowing mechanics, daytime clenching, and forward head posture can keep reloading the same tissues.
That's where orofacial myofunctional therapy can be useful. It focuses on retraining how the muscles of the face, tongue, and jaw work during breathing, chewing, and swallowing. It isn't a replacement for structural care. It's a way to reduce the forces that keep sabotaging it.
A practical conservative plan often includes:
- Custom appliance care for joint unloading or clenching control
- Targeted physical therapy for mobility, muscle calm, and neck support
- Home stretching done gently and consistently
- Trigger reduction such as limiting gum chewing, tough foods, and daytime bracing
- Functional retraining when breathing or oral posture issues are part of the pattern
One example of this approach is Pain and Sleep Therapy Center, which offers TMJ treatment plans that may include orthotic therapy and cold laser therapy as part of broader root-cause care.
Comparing Your TMJ Migraine Treatment Options
Not every treatment is trying to do the same job. Some options calm muscle tension. Some protect the joint. Some reduce inflammatory load. Some aim to improve tissue healing. Others help patients stop repeating the mechanics that started the problem.
That's why a side-by-side view helps.
Comparison of TMJ Migraine Treatment Approaches
| Treatment Category | Primary Goal | Invasiveness | Best For |
|---|---|---|---|
| Conservative self-care | Reduce irritation and prevent flare-ups | Low | Early symptoms, mild flare-ups, support between visits |
| Custom oral appliance | Reduce overload, protect teeth, improve jaw stability | Low | Clenching, grinding, joint strain, bite-related muscle overuse |
| Physical therapy and home exercises | Improve jaw motion, reduce muscle guarding, support neck-jaw mechanics | Low | Muscle-driven pain, limited opening, postural contribution |
| Medication management | Reduce pain, calm inflammation, address migraine or muscular symptoms | Low to moderate | Short-term symptom control or mixed migraine-TMD cases |
| Regenerative or injection-based care | Target joint irritation or tissue healing when conservative care plateaus | Moderate | Persistent symptoms, joint degeneration, selected structural cases |
| Lifestyle and behavior change | Lower daily load on the system | Low | Nearly everyone, especially clenchers and stress-related flare patterns |
The trade-offs that matter
A few decision rules help patients think clearly:
- If the problem is mostly mechanical, pills alone usually won't solve it.
- If migraine biology is active, jaw-only care may help but won't fully control the headaches.
- If the joint is inflamed or structurally irritated, advanced options may deserve discussion after a solid conservative trial.
- If habits keep reloading the jaw every day, even a technically good treatment can fail.
Cost and convenience matter too, but the bigger question is fit. The right treatment for TMJ migraines depends on whether the main driver is muscle, joint, clenching, migraine, airway, or a mix.
When to Consider Advanced Therapies for TMJ Pain
Some patients do the basics well and still feel stuck. They've adjusted diet, started stretching, used a custom appliance, and worked on triggers, yet the jaw remains inflamed or the headaches keep cycling. That's usually the point where advanced, non-surgical options become worth discussing.
Regenerative injections and phenotype-specific care
Recent clinical literature increasingly discusses injection-based and regenerative approaches for TMD-related pain, including platelet-rich plasma and platelet-rich fibrin, with growing evidence supporting their use in conditions such as TMJ osteoarthritis. The same literature also reinforces that phenotype-specific care matters, meaning the right advanced therapy depends on the type of TMJ problem you have (review of regenerative approaches for TMD-related pain).
PRF and related treatments are best understood as biologic support, not magic. They may be reasonable when the joint itself is part of the problem and foundational care hasn't produced enough change. They are less compelling when the main driver is untreated clenching, neck mechanics, or a primary migraine disorder that still needs neurologic management.
Cold laser and targeted symptom modulation
Another option some clinics use is cold laser therapy, also called photobiomodulation. The idea is to apply light energy in a controlled way to support tissue recovery and reduce irritation. It isn't surgery, and it doesn't immobilize the jaw. It's usually considered an adjunct, not a stand-alone cure.
For readers who want a technical primer on how low-level laser therapy is used more broadly, this overview of LLLT for aesthetic clinics is a useful starting point for understanding the modality itself.
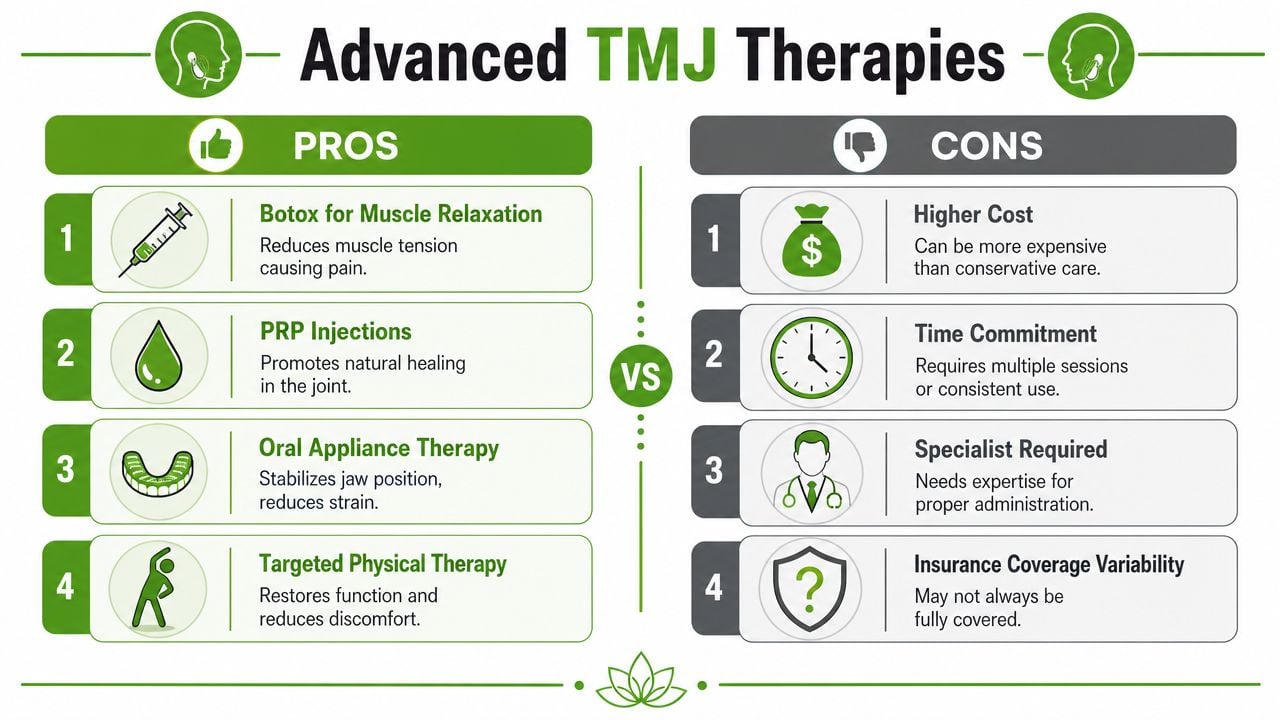
A short visual overview helps make these options less abstract:
Medication and Botox need context
Medication can still play a role in advanced care, but the details matter. The Migraine Disorders evidence summary reports that 25 mg of amitriptyline for two months reduced spontaneous pain by 63% in people with chronic TMD, compared with a 16% reduction in the placebo group. The same source notes that botulinum toxin type A is FDA-approved for chronic migraine but remains off-label for TMD-related pain, and the National Institute of Dental and Craniofacial Research states it is approved for some medical conditions like migraines but not for TMDs (Migraine Disorders evidence summary on migraine and TMD).
That doesn't mean Botox is never discussed in jaw cases. It means patients should understand exactly what problem is being treated and what isn't formally approved.
If symptoms remain severe despite careful non-surgical care, some patients also ask whether surgery is next. This overview of TMJ disc displacement surgery can help clarify when structural intervention enters the conversation and when it doesn't.
Advanced care should be an escalation based on findings, not frustration alone.
Daily Habits to Manage TMJ Migraines and Prevent Flare-Ups
The day-to-day habits matter more than commonly realized. A joint and muscle system that gets irritated all day won't stay calm just because you had one good appointment.
One misconception needs to be corrected early. Immobilizing the jaw is not helpful. The AAFP reports that TMJ immobilization has shown no benefit and may worsen symptoms through muscle contracture and reduced synovial fluid production. First-line care instead emphasizes jaw rest, soft diet, and passive stretching, along with other supportive measures, and the same review notes that naproxen is the only NSAID with proven benefit for TMD pain while muscle relaxants may be added when a muscular component is present (AAFP review of TMD management).
Daily habits that usually help
- Eat with the joint in mind: Choose softer foods during a flare. Cut food into smaller bites. Pause on bagels, jerky, thick sandwiches, gum, and hard candies if they trigger symptoms.
- Keep the jaw position neutral: Lips together, teeth apart, tongue resting lightly on the palate if that's comfortable for you. Many people clench during computer work without noticing.
- Use heat thoughtfully: A warm compress over the jaw muscles can help relax a flare driven by tightness.
- Support posture: Raise screens to eye level, keep shoulders relaxed, and avoid a prolonged forward-head position.
- Reduce one-sided loading: Don't chew on one side only. Don't hold the phone between shoulder and ear. Don't rest your chin in your hand for long periods.
Gentle movement beats guarding
A sore jaw often makes people want to “freeze” it. That usually backfires. Gentle controlled movement helps maintain circulation, muscle balance, and joint nutrition.
Practical rule: Rest the jaw from strain, not from all motion.
Simple nasal breathing, unclenching reminders, and brief jaw relaxation breaks during the day can lower the background load that feeds both TMJ pain and headache flare-ups.
Your Treatment Roadmap and When to See a TMJ Specialist
Patients don't need a dozen treatments at once. They need the right sequence.
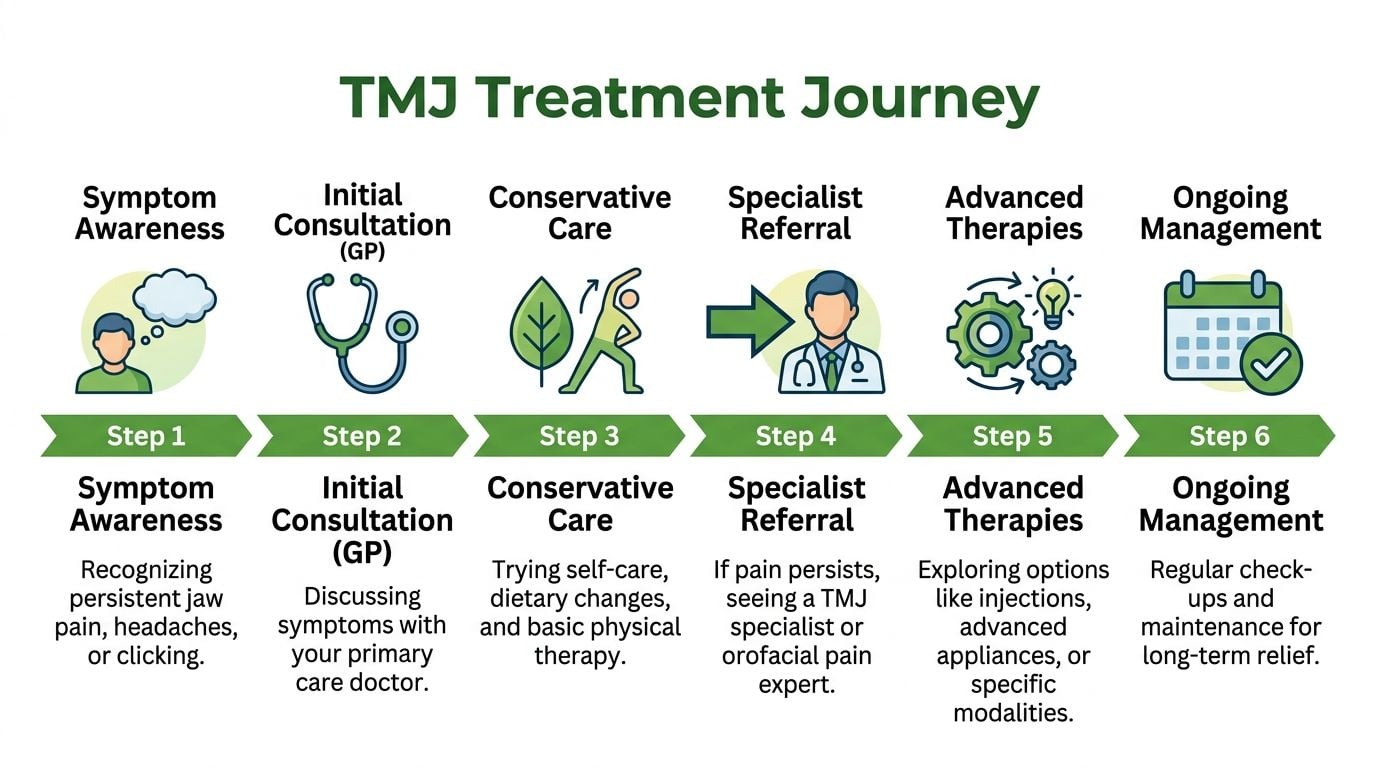
The usual roadmap starts with a careful diagnosis, followed by foundational conservative care aimed at the actual driver of pain. If the findings point to muscle overload, treatment focuses there. If the joint is inflamed or structurally involved, the plan shifts. If migraine remains active in parallel, that piece needs direct attention too. Good care is phased because the jaw and headache system rarely improve from guesswork.
A practical sequence
Notice the pattern
Track when the headaches occur, what the jaw feels like, and whether chewing, stress, sleep, or clenching seem involved.Get a differential diagnosis
Don't assume every temple headache is “TMJ” and don't assume every throbbing headache is “just migraine.”Start with conservative care
This often includes a custom appliance when appropriate, targeted exercises, trigger reduction, and behavior change.Reassess the response
If symptoms improve but don't resolve, the next step may be more specific physical therapy, medication coordination, or functional retraining.Escalate selectively
Persistent joint-driven cases may justify discussion of regenerative therapies, cold laser, or other advanced care.
When you shouldn't wait
Make an appointment with a TMJ-focused clinician or orofacial pain specialist if you have:
- Jaw locking or catching
- Pain that keeps returning despite self-care
- Headaches that disrupt work, sleep, or daily function
- Pain with chewing or reduced jaw opening
- Frequent use of pain relievers without a clear diagnosis
- A bite that suddenly feels different after symptoms begin
The most effective treatment for TMJ migraines starts when someone stops asking, “What can I take for this?” and starts asking, “What exactly is generating this pain?”
If you're dealing with jaw pain, facial tension, clenching, or headaches that seem connected, Pain and Sleep Therapy Center offers evaluation and treatment for TMJ disorders, facial pain, and related sleep-breathing issues. A thorough assessment can help clarify whether you're dealing with migraine, TMD-referred pain, or both, and what phased treatment approach makes sense next.



