
You wake up with pain at your temples, maybe behind one eye, maybe across your forehead. You drink water, blame stress, take an over-the-counter pain reliever, and push through the day. By evening, your jaw feels tired, your neck is tight, and the headache never fully leaves.
That pattern is common. It also sends many people down the wrong path for months or years. They get treated for “sinus headaches,” “regular tension headaches,” or migraines, while the underlying driver sits much lower in the system. The jaw muscles, the jaw joints, and in many cases, the way they breathe during sleep.
Headaches caused by jaw clenching often hide in plain sight. People don’t always realize they clench because much of it happens at night. Others know they tighten their jaw during work, driving, or exercise, but they don’t connect that habit to temple pain, ear pressure, or morning headaches. Once you understand that link, the treatment approach changes. Instead of chasing the pain, you start looking for the source.
That Persistent Headache Might Not Be What You Think
A familiar story walks into clinic settings every week. Someone has had recurring headaches for a long time. The scans are unremarkable. Medication helps for a few hours. Massage helps briefly. A new pillow helps a little. Nothing explains why the pain keeps returning.
Then a few details surface. They wake with sore cheeks. Their partner hears grinding at night. Their teeth feel sensitive in the morning. Their jaw clicks when they chew a bagel or yawn.
That combination matters. Jaw clenching, also called bruxism, can overload the chewing muscles and create pain in exactly the areas where many people feel “headaches.” A key study on temporomandibular disorder, often aggravated by clenching, found headaches were more common in people with TMD symptoms at 27.4% compared with 15.2%, a 12.2% higher incidence according to this review of bruxism and headaches.
Why people miss the real cause
Most patients don’t think “jaw” when the pain is in the temples, forehead, or behind the eyes. They think dehydration, screen time, poor sleep, sinus pressure, or migraine. Those are reasonable guesses, but they can keep you focused on symptom relief instead of pattern recognition.
A more useful first question is this: what else shows up with the headache?
- Morning jaw fatigue means the muscles may have been working all night.
- Ear fullness or temple soreness can come from nearby jaw structures, not the ear or sinuses.
- Pain with chewing or talking points away from a primary headache disorder and toward a mechanical trigger.
- Neck and shoulder tightness often travels with chronic jaw tension.
For many patients, the turning point is a broader evaluation. If you want a good overview of diagnosing headache root causes, that resource gives a helpful framework for thinking beyond the pain location alone.
A headache that keeps returning deserves a source-based workup, not repeated guesswork.
Relief starts when the question changes
Instead of asking, “What can I take when this starts?” ask, “What is repeatedly loading the same tissues?”
That’s where jaw clenching becomes more than a dental habit. It becomes a mechanical, muscular, and sometimes sleep-related reason your head hurts.
How Jaw Muscles Trigger Headaches
The fastest way to understand this is to think about what happens after overworking any muscle group. If you do too many squats after a long break, your legs feel sore, tight, and inflamed. Jaw muscles respond the same way. The difference is that they can work while you sleep, and the pain often shows up in your head instead of feeling limited to the jaw.
The two muscles most often involved are the masseter and temporalis. They’re built for chewing, speaking, and stabilizing the jaw. They are not meant to stay switched on for hours.
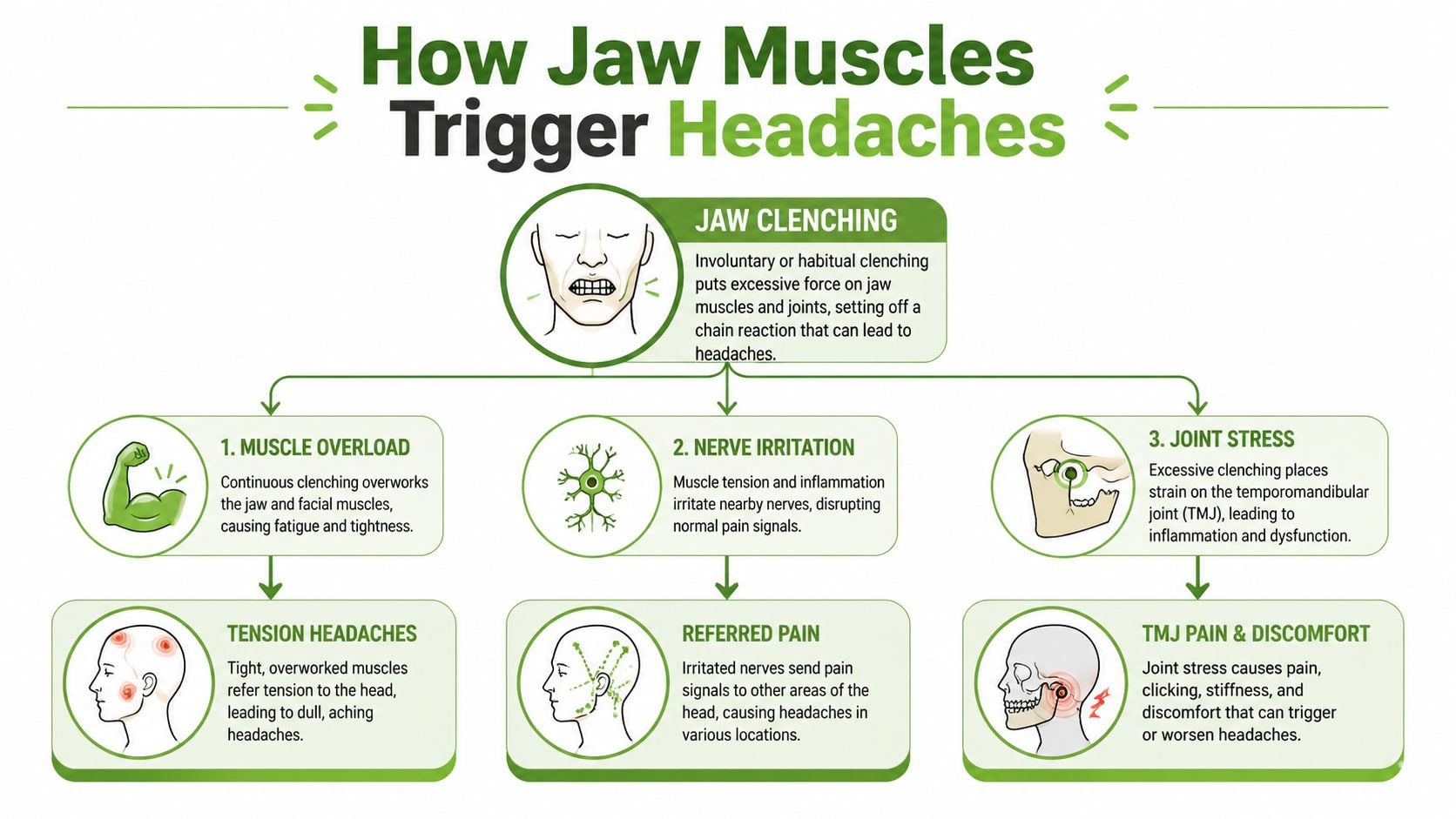
What clenching does to muscle tissue
When you clench, those muscles contract without the normal rhythm of chewing and release. That creates prolonged tension. During sleep-related bruxism, sustained isometric contractions can reach up to 250% of maximal voluntary force, causing microtrauma and inflammation in the temporalis tendon and related attachment sites, with pain radiating through the trigeminocervical complex to the frontal and temporal areas according to this clinical review on sleep-related bruxism.
That matters because the temporalis sits right where many people point when they say, “My headache starts here.”
Referred pain is why the headache feels confusing
A clenching headache doesn’t always feel like jaw pain. Muscles can create referred pain, which means the brain interprets the pain in a nearby or connected area rather than exactly where the problem starts.
With the jaw, that often means:
- Temple pain from a strained temporalis muscle
- Forehead pressure from irritated muscle and tendon structures
- Pain at the base of the skull or upper neck because the jaw and neck systems compensate for each other
- One-sided head pain when one side clenches harder than the other
That’s why headaches caused by jaw clenching are so often mislabeled.
Practical rule: If your headache comes with jaw tiredness, cheek tension, or pain when opening wide, the jaw deserves attention even if the pain feels “in your head.”
Joint stress adds another layer
Some patients have mostly muscle overload. Others also have stress in the jaw joints themselves. When the bite force rises and the jaw doesn’t move well, the joint capsule and surrounding tissues can become irritated. That can add ear-area pain, clicking, catching, or a sense that the bite feels “off” after waking.
A few patterns make clenching more likely to trigger headaches:
- Nighttime episodes that leave you sore in the morning
- Daytime concentration clenching during computer work, driving, or exercise
- Stress-based tightening where the shoulders rise and the jaw locks at the same time
- Poor oral resting posture with the teeth touching when they should be apart
The small habit that matters all day
Healthy jaws spend most of the day in a relaxed resting position. Lips can be closed, tongue can rest gently against the palate, but the teeth should not stay together. Constant tooth contact keeps the elevator muscles of the jaw active.
That sounds simple, but it’s clinically important. Many patients reduce symptom intensity once they learn to interrupt daytime clenching. It doesn’t fix every case. It does reduce one major source of repeated loading.
The key point is this. Your head may hurt because your jaw muscles never get to rest.
The Critical Link to TMJ and Airway Connection
A common pattern looks like this: the headache is worst in the morning, the jaw feels tight before breakfast, and a standard nightguard only helps part of the problem. In that situation, I do not stop at the jaw joint alone. I also look at how the patient is breathing during sleep.
The temporomandibular joints sit just in front of the ears and coordinate every opening, closing, chew, and word. Repeated clenching loads the joint surfaces, the disc, and the muscles attached around them. Once that system is irritated, pain does not always stay local. It can spread into the temples, around the ear, behind the eye, or into the back of the head.
The missing piece is often the airway
Many articles treat nighttime clenching as a stress habit. Clinically, that is only part of the picture. In some patients, clenching happens during sleep because the body is trying to stabilize the jaw or reopen space for breathing when the airway becomes less stable.
That matters because it changes the treatment plan. If sleep-disordered breathing is driving the clenching, a guard may protect teeth but still leave the headache cycle in place.
The sequence often works like this:
- breathing becomes less stable during sleep
- the jaw and facial muscles brace or thrust forward
- the TMJ and surrounding muscles absorb repeated load
- sleep gets lighter and more fragmented
- the patient wakes with headache, jaw soreness, or both
This relationship has been discussed in clinical reviews of sleep bruxism and airway disorders, including this overview of jaw clenching headaches and airway issues.
Signs the problem may be bigger than the bite
A jaw-focused exam should widen if headache patterns travel with poor sleep or breathing symptoms. The clues are often simple:
- Morning headaches with dry mouth
- Snoring, mouth breathing, or nasal blockage
- Unrefreshing sleep
- Frequent waking or restless sleep
- Jaw pain that is worse on waking than later in the day
Chewing symptoms can add another clue. If meals trigger discomfort along with headache, this article on common causes of chewing pain can help separate bite strain and jaw overload from a tooth-specific problem.
Why a single-tool approach often falls short
Interdisciplinary care becomes necessary at this stage. Some patients need joint and muscle treatment. Others also need screening for mouth breathing, nasal resistance, or sleep apnea. Tongue posture, lip seal, and daytime oral rest posture can also influence how much strain the jaw carries over 24 hours. For readers who want to understand that side of care, myofunctional therapy for mouth breathing explains how breathing patterns and oral muscle function connect.
The practical point is straightforward. Jaw clenching can be the symptom you notice first, while the deeper driver is a mix of TMJ overload and disrupted breathing during sleep. Treating the root cause usually means looking at both.
Is Your Jaw the Source of Your Headaches
You wake up with pressure at your temples, your jaw feels tight when you start talking, and breakfast makes the pain more obvious. That pattern deserves a closer look at the jaw, especially when routine headache advice has not solved the problem.
Patients ask this every day. How can you tell whether the headache is coming from the jaw or from something like tension headache or migraine?
Symptoms alone do not give a final diagnosis, but the pattern is often very informative. Headaches related to clenching or TMJ problems usually have a mechanical pattern. They flare with chewing, wide opening, long conversations, or first thing in the morning. In practice, morning pain matters even more when it shows up with poor sleep, snoring, dry mouth, or daytime fatigue, because nighttime clenching is often part of a bigger breathing problem rather than an isolated jaw habit.
Signs that point toward clenching or TMJ involvement
Look for clusters of symptoms, not one clue in isolation.
- You wake with the headache, or it is strongest in the morning.
- Your jaw feels tired, sore, or stiff when you begin eating or speaking.
- You notice clicking, popping, or shifting in front of the ear.
- Hard, chewy, or large bites trigger pain.
- Your temples or cheek muscles feel tender when you press on them.
- You feel ear pressure or fullness even though the ear exam is normal.
- The headache gets worse with wide opening or side-to-side jaw movement.
- You have signs of clenching, such as tooth wear, a scalloped tongue, or cheek biting.
Chewing pain can confuse the picture because tooth problems and jaw overload can feel similar. If meals reliably trigger symptoms, this guide on common causes of chewing pain can help you sort out whether the source is more likely a tooth, the bite, or the jaw muscles.
Headache type comparison
| Symptom | Clenching/TMJ Headache | Tension Headache | Migraine |
|---|---|---|---|
| Typical timing | Often on waking, or after chewing, talking, or clenching | Often builds with stress or prolonged posture | Often comes in episodes and may not relate to jaw use |
| Pain location | Temples, around the ears, behind the eyes, back of head | Diffuse, band-like pressure | Often one-sided, but location varies |
| Jaw soreness | Common | Less common | Not a defining feature |
| Clicking or deviation | Common | Uncommon | Uncommon |
| Worse with jaw movement | Often | Usually no | Usually not the main trigger |
| Ear fullness or facial tightness | Common | Less typical | Can occur, but less often with a mechanical trigger |
| Nausea or light sensitivity | Possible, but not the main pattern | Usually mild or absent | More consistent with migraine |
The pain pattern often follows jaw muscles and joint mechanics
Jaw-related headaches often spread beyond the joint itself. Tight temporalis and masseter muscles can send pain into the temples, around the ear, behind the eyes, and sometimes toward the back of the head. That is why people are sometimes told they have a sinus, ear, or “stress” headache when the jaw is contributing more than anyone realized.
Jaw movement is one of the most useful home clues. If the pain changes when you clench, chew, yawn, or open wide, the jaw has moved higher on the list of possible causes.
When headache pain rises and falls with jaw function, the jaw deserves a proper exam.
When to seek a specialty evaluation
Primary care is often the right starting point, especially for a new, severe, or unusual headache. A more targeted TMJ and airway evaluation makes sense when the story keeps circling back to jaw use, sleep, and morning symptoms.
Consider that evaluation if:
- headaches keep returning despite standard headache treatment
- pain is linked to chewing, talking, clenching, or waking
- you grind, clench, or show visible tooth wear
- sleep feels poor, restless, or unrefreshing
- snoring, mouth breathing, or dry mouth are part of the picture
- you have been given a nightguard, but the headaches keep coming back
A good workup looks at the muscles, joints, bite, and airway together. That is the difference between temporary symptom control and treatment that matches the actual driver. If you want to see what that kind of care can include, this overview of TMJ treatment options that address both joint strain and related causes is a useful next step.
Evidence-Based Treatments for Lasting Relief
Lasting relief starts with a better question. What is making the jaw work so hard, especially during sleep?
For some patients, the main problem is muscle overuse. For others, it is joint irritation, an unstable bite relationship, daytime clenching habits, or sleep-disordered breathing that keeps the nervous system on alert and the jaw braced at night. That is why a pill, a store-bought guard, or a few massage sessions often help for a short time but do not change the pattern.

What often gives short-term relief only
These options can still be useful. They just need to be put in the right role.
- Over-the-counter pain relievers can reduce pain intensity during a flare, but they do not stop repeated nighttime loading of the jaw muscles.
- Soft foods for a few days can calm an irritated joint or sore chewing muscles, but they do not address why the strain keeps returning.
- Boil-and-bite or drugstore nightguards may protect teeth from wear, but they are not designed around your joint position, muscle pattern, or breathing status during sleep.
- Occasional massage or manual therapy can relax tight muscles, though the tension often returns if the trigger is still active.
If you need short-term symptom support while you sort out the cause, this guide to fast migraine headache relief may help as general context. Jaw-driven headaches still need their own workup, because treatment for migraine and treatment for clenching are not interchangeable.
Custom appliances have a role, but they are not the whole plan
A well-made oral appliance can reduce tooth damage, decrease muscle overload in some patients, and give the jaw a more stable position at night. That can be a meaningful part of care.
The trade-off is that a custom device only works well when it is based on a real diagnosis. If clenching is being driven by airway resistance, fragmented sleep, or significant joint inflammation, the appliance may help protect tissues without fully solving the reason the jaw is active. That is why I caution patients against expecting any guard to be a complete answer.
A good summary of non-surgical TMJ treatment options shows how appliances fit into a broader plan rather than standing alone.
Therapy works better when it changes function
Patients often improve more steadily when treatment retrains the habits and mechanics feeding the problem.
Orofacial myofunctional therapy focuses on tongue posture, lip seal, swallowing pattern, nasal breathing, and resting muscle tone. Those details matter. A low tongue posture, open-mouth posture, or chronic mouth breathing can keep the jaw, face, and neck working harder than they should.
Breathing retraining, including Buteyko-based methods in selected cases, can help patients who overbreathe, mouth breathe, or show signs of poor breathing mechanics. In practice, this matters most when headaches, clenching, dry mouth, snoring, and unrefreshing sleep show up together. That combination often points to a bigger picture than “stress.”
Joint treatment matters when the joint is the generator
Some headaches keep returning because the TMJ itself is irritated or unstable. In that situation, muscle treatment alone may not hold for long.
Selected patients may benefit from joint-focused care such as guided rehabilitation, cold laser therapy, or regenerative injections such as Prolotherapy or PRF. These are not first-line treatments for every person with jaw pain. They make more sense when the exam shows that joint strain keeps reactivating the surrounding muscles and headache pattern.
Pain and Sleep Therapy Center is one example of a practice model that evaluates TMJ problems, facial pain, and sleep-related breathing issues together. That matters because a patient can have both joint dysfunction and airway-related clenching, and each problem can keep the other active.
Later in the care pathway, education also matters. This video gives a helpful visual overview for patients trying to understand how TMJ symptoms and treatment fit together.
Why root-cause care lasts longer
The best treatment plans are layered and selective. They protect the teeth if needed, calm irritated muscles, support the joint when it is unstable, and look carefully at sleep and breathing when the history points there.
That last step is the one many headache articles miss. If the body is struggling to maintain airflow at night, clenching can act like a stabilizing response. In those cases, symptom control alone rarely lasts. Relief tends to hold better when the plan addresses the jaw and the airway together.
The right treatment plan should explain why you clench, not just reduce the damage it causes.
Simple At-Home Strategies to Reduce Jaw Tension
Clinical treatment matters, but what you do all day also shapes the outcome. The jaw responds to repetition. Small habits repeated for hours can keep symptoms active, even with good in-office care.
These home strategies are safe, practical, and worth using while you pursue a proper diagnosis.
Reset your daytime resting posture
Daytime clenchers often don’t notice it until they’re asked to check. Start there.
Use this simple resting position:
- Tongue up with the tip resting gently on the palate
- Teeth apart instead of touching
- Lips together without strain
- Jaw relaxed with no forward thrusting
Put reminder notes on your monitor, dashboard, or phone if needed. “Teeth apart” is enough.
Use heat and gentle movement during flares
When the jaw muscles are tight, a warm compress can help them let go. Apply gentle warmth to the cheeks and temple area for a short period, then follow with slow opening and closing movements that stay within a comfortable range.
Avoid aggressive stretching. The goal is to reduce guarding, not force range.
For hands-on self-care, this guide on how to massage your jaw can help you target the right areas without overdoing it.
Reduce mechanical strain for a few days
During a flare, the jaw needs less work.
Try this short-term adjustment:
- Choose softer foods such as soups, eggs, yogurt, or cooked vegetables
- Skip gum and chewy snacks
- Cut large foods into smaller bites
- Avoid very wide opening when yawning, singing, or biting into thick sandwiches
These steps won’t cure the problem, but they can calm an irritated system.
Check your neck and screen posture
Jaw tension rarely lives alone. Forward head posture often travels with neck tightness and increased jaw muscle activity. If you work at a screen, bring it to eye level, keep your shoulders relaxed, and let your tongue rest up instead of bracing the jaw.
A relaxed jaw is easier to maintain when the neck isn’t fighting to hold the head forward all day.
Build a short evening routine
Nighttime clenching is involuntary, but the body still responds to pre-sleep conditions. A simple evening routine can help lower general muscle tone:
- warm compress
- nasal breathing practice
- jaw and neck relaxation
- no gum, heavy chewing, or late jaw-intensive meals
Think of these as ways to lower the load, not replace an evaluation if symptoms persist.
Your Questions About Jaw Clenching Headaches Answered
A common pattern looks like this. You wake with pressure at the temples, your jaw feels tired before breakfast, and by midday the pain has turned into what seems like another “normal” headache. In many patients, that pattern points back to overnight jaw activity, and sometimes to strained breathing during sleep that keeps the jaw and facial muscles active for hours.
Can jaw clenching really cause headaches every day
Yes. Daily headaches can happen when the jaw muscles are loaded so often that they never fully settle down. I am more suspicious of jaw-driven headaches when they show up in the morning, worsen with stress or chewing, or come with jaw soreness, tooth wear, ear pressure, or facial fatigue.
Are over-the-counter nightguards enough
They can protect teeth. That is useful, but it is not the same as diagnosing why the clenching is happening.
If the main issue is mild grinding without joint irritation or sleep disruption, a simple guard may help limit dental damage. If headaches are tied to TMJ strain, a bite imbalance, nasal obstruction, mouth breathing, or sleep-disordered breathing, a store-bought guard usually leaves the main driver untouched. In some cases, it can even make symptoms harder to interpret because the teeth are covered while the muscles keep overworking.
Will treatment fix the problem permanently
That depends on the cause. Habit-driven daytime clenching often improves with muscle-focused care, bite awareness, and changes in head and neck posture. Cases tied to joint instability, poor tongue posture, chronic mouth breathing, or sleep apnea usually need a broader treatment plan and follow-up over time.
A realistic goal is stable relief, fewer flares, better sleep, and less strain on the jaw system.
Why do I only get the headache in the morning
Morning headaches often mean the jaw has been under load overnight. That can come from sleep bruxism, repeated arousals from restricted breathing, or both.
This connection gets missed all the time. During sleep, the body may tense the jaw and facial muscles as part of a response to airway resistance. In that situation, the headache is not just a jaw problem. It is a jaw-and-sleep problem, and treatment works better when both are evaluated.
Why does my doctor think it’s sinus pressure
Because the pain patterns overlap. Jaw muscle pain and TMJ irritation can show up in the temples, cheeks, around the ears, and behind the eyes. That can feel very similar to sinus pressure, especially if congestion is also present.
If sinus treatment has not changed the pattern, and you also notice jaw tenderness, clicking, limited opening, clenching, or chewing pain, the jaw deserves a closer look.
What makes an interdisciplinary approach different
It examines the full chain that can keep headaches going. That includes the jaw muscles, TMJ function, tooth contact, tongue posture, nasal breathing, sleep quality, and airway stability.
That matters because isolated treatment often gives partial relief. A guard may protect teeth but miss airway strain. Physical therapy may calm muscles but not address nighttime breathing. Sleep treatment may improve rest but leave joint loading untreated. The best plan depends on what your exam shows.
Can children or teens have similar problems
Yes. Younger patients can have jaw tension, mouth breathing, poor oral posture, unrestful sleep, and headache patterns linked to the same jaw-airway relationship. The evaluation should match the child’s age and symptoms, but the connection is real and worth checking early.
Recurring headaches with jaw tightness and poor sleep are worth a targeted evaluation. Pain and Sleep Therapy Center evaluates how the jaw, TMJ, bite, and sleep-breathing patterns interact so treatment can focus on the source of the problem rather than temporary symptom control.



