
If you're reading about regenerative medicine for back pain, you're probably already tired of the usual cycle. Rest helps for a few days. Physical therapy helps somewhat, then progress stalls. Medication dulls the pain but doesn't change why your back keeps flaring. Surgery may feel too big, too risky, or plainly not right for the problem you've been told you have.
That frustration is valid. Many people with chronic back pain aren't looking for a miracle. They want a treatment path that makes sense, matches the actual pain generator, and gives them a realistic chance to move better without jumping straight from pills to an operation.
Understanding Regenerative Medicine for Chronic Back Pain
Regenerative medicine for back pain is a category of treatments that tries to support tissue repair instead of only blocking pain signals. That difference matters. Traditional care often focuses on calming inflammation, reducing muscle spasm, or avoiding movement long enough for symptoms to settle. Regenerative care asks a different question: is there a damaged structure that isn't healing well on its own?
For some patients, the answer may involve a disc, a ligament, a tendon attachment, a facet joint capsule, or another soft tissue structure that keeps sending pain signals because it remains irritated or mechanically stressed. In that setting, regenerative treatment is meant to work like a cellular repair crew. Rather than covering the alarm with more medication, the goal is to send targeted biological signals into the area and encourage a more organized healing response.
Why patients start looking beyond standard care
This growing interest isn't coming out of nowhere. A PubMed-indexed review discussing intradiscal biologics notes that discogenic low back pain affects an estimated 26% to 42% of adults with chronic back pain, and that the 2019 to 2022 period marked a shift toward pooled evidence and broader clinical discussion of biologic treatments as alternatives to surgery or long-term medication in selected cases (systematic review and meta-analysis on biologic injections).
That doesn't mean regenerative medicine is right for every sore back. It means more clinicians and patients are asking a reasonable question: if the problem is tissue degeneration or poor healing, should treatment try to influence healing itself?
A practical overview of regenerative medicine services can help frame the concept, but the key point is simple. This is not one treatment. It's a family of treatments with different biological roles and different best-use scenarios.
Practical rule: The better the diagnosis, the more useful regenerative treatment becomes. Vague back pain rarely responds well to a vaguely chosen injection.
What regenerative medicine is not
It isn't a shortcut around diagnosis. It isn't a guarantee that damaged tissue will fully regenerate. And it doesn't replace the basics, such as movement restoration, strength, sleep, load management, and a rehab plan that respects how the spine works.
Patients do best when they understand the trade-off. Regenerative medicine for back pain can be appealing because it is usually less invasive than surgery and more targeted than long-term medication. But it also requires patience. Healing biology moves slower than a numbing injection.
A good mindset is this: not miracle care, not hype, but a structured attempt to improve the environment for healing.
A Look at Common Regenerative Therapies
Different regenerative therapies do different jobs. One treatment may make sense for an irritated ligament. Another may be used when a disc is the likely pain source. Lumping them together causes confusion, and it often leads patients to compare treatments that aren't trying to do the same thing.
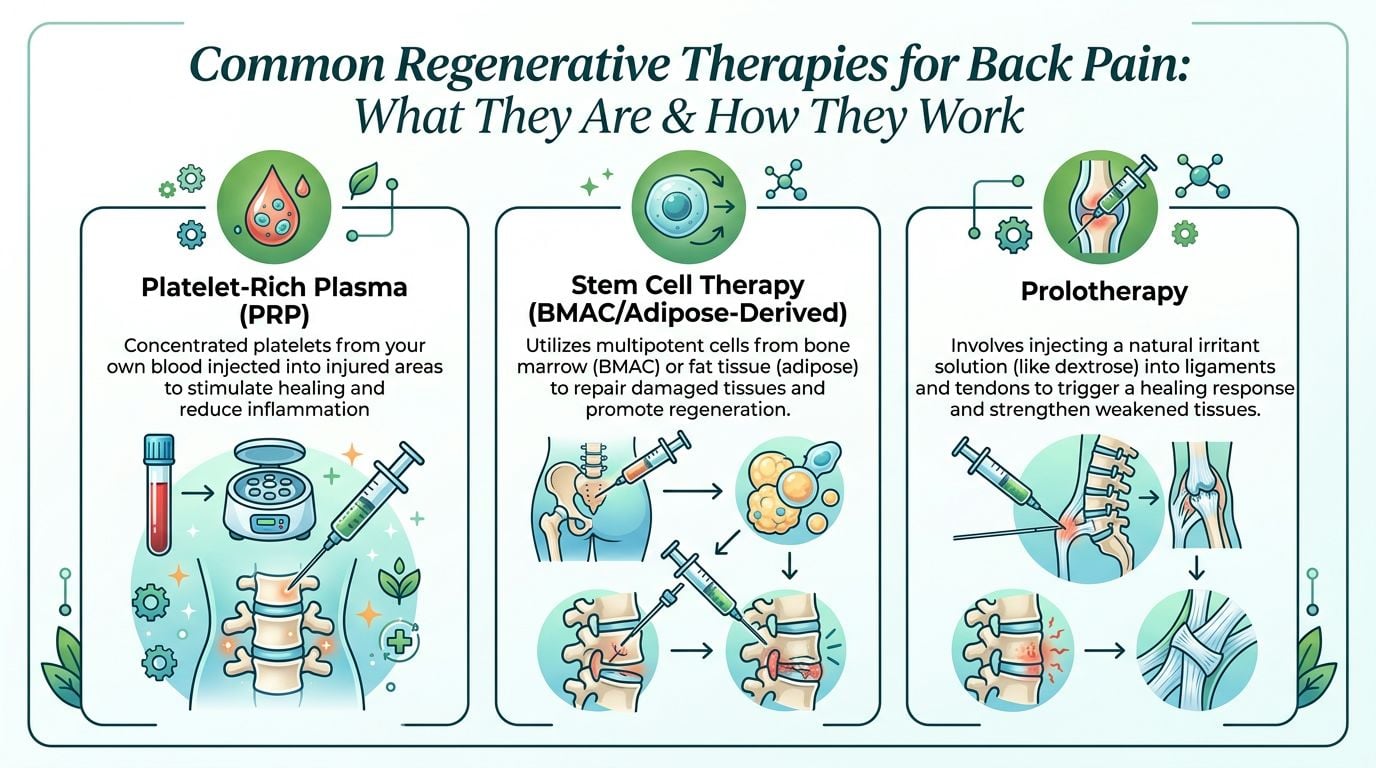
PRP and PRF
Platelet-rich plasma, or PRP, is made from your own blood. A sample is drawn, processed, and concentrated so the final injectate contains a higher level of platelets than routine blood. Those platelets release growth factors that may help influence the local healing environment.
A review of biologic therapies notes that PRP uses concentrated growth factors from a patient's own blood to stimulate matrix synthesis, and that PRP and prolotherapy are considered biologically plausible options in early-to-moderate degenerative conditions when standard conservative care has failed (review of biologics for low back pain).
Platelet-rich fibrin, or PRF, is closely related in concept. It's also derived from the patient's own blood, but it forms a fibrin matrix that may allow a slower release of signaling factors. In practice, clinicians may use PRP or PRF depending on the target tissue and the treatment strategy.
These treatments are often discussed for:
- Disc-related pain: especially when imaging and the clinical story suggest early or moderate degeneration
- Ligament or tendon support: when tissue laxity or chronic strain appears to be driving pain
- Joint-related irritation: including some mechanically painful areas around the spine
Prolotherapy
Prolotherapy is different from PRP because it doesn't rely on blood products. It uses an irritant solution, commonly dextrose-based, to trigger a local healing response in connective tissue.
That may sound counterintuitive until viewed as rebooting a stalled repair process. In some chronically painful tissues, the body doesn't seem to mount a strong enough healing response to finish the job. Prolotherapy aims to restart that response.
It is commonly considered when the problem appears to involve:
- Ligament laxity
- Tendon or attachment point pain
- Mechanical pain patterns where instability or poor soft tissue support seems to contribute
Stem cell-based therapy and related cell procedures
When people say "stem cell therapy," they're often referring broadly to treatments involving mesenchymal stem cells, or MSCs, or cell-based preparations derived from bone marrow or adipose tissue. In spine care, the interest is strongest around disc-related degeneration because these cells may influence inflammation and matrix repair signaling.
Cell-based procedures are usually reserved for more specific situations than PRP or prolotherapy. They aren't a casual next step for generic low back pain. They tend to fit a narrower group of patients with a clearer structural diagnosis.
For patients comparing options for joints and spine more broadly, this overview of regenerative medicine for joint pain can help clarify how target tissue changes the treatment choice.
Cold laser therapy
Cold laser therapy, also called low-level laser therapy, isn't an injection. It uses light energy with the goal of influencing inflammation, circulation, and tissue recovery. It doesn't replace a precisely placed injection when the problem is inside a disc or ligament, but some clinicians use it as part of a broader healing plan.
That makes it better understood as an adjunct than a stand-alone answer for every patient. It may help calm tissue irritation and support recovery, especially when paired with activity modification and rehab.
Some regenerative tools are meant to signal repair. Others are meant to create better conditions for repair. That's why matching the therapy to the pain generator matters more than chasing the newest acronym.
Evaluating the Evidence for Back Pain Relief
Many articles become vague. They talk about promise, innovation, and healing potential, but they don't answer the fundamental question: what does the evidence say, and how should you interpret it?
The honest answer is that the evidence is encouraging in selected patients, but it isn't uniform. Study quality varies. Treatment methods vary. Patient selection varies. Even the meaning of the word "success" varies.
What success means in the literature
A useful evidence benchmark comes from a 2022 review summarized by Medical News Today. In that review, stem cell injections for lower back pain showed a 6-month success rate of 53.5%, but that dropped to 40.7% under worst-case analysis. Functional improvement looked different depending on how researchers calculated outcomes, with 44.1% to 74.3% of patients achieving at least a 30% improvement in function (review summary of stem cell injections for lower back pain).
Those numbers aren't contradictory. They show why patients need to ask a sharper question than "Does it work?" A better question is, what outcome are we measuring?
Here's a simple way to think about it:
| Outcome type | What it means for you |
|---|---|
| Pain reduction | Your pain score goes down |
| Functional improvement | You can sit, walk, bend, sleep, or work better |
| Worst-case analysis | Researchers assume less favorable outcomes for missing data or other uncertainties |
A treatment can improve pain without changing your daily function enough to feel life-changing. It can also help function even if pain doesn't vanish. In clinic, that distinction matters a lot.
Where the promise seems strongest
The best current signal is in carefully selected patients, especially those with discogenic pain that fits the imaging, exam, and symptom pattern. That doesn't mean every degenerated disc should be injected. Many abnormal MRI findings are not the true pain source.
What the literature suggests is more modest and more useful. Some biologic treatments may help when:
- The diagnosis is specific
- Conservative care has plateaued
- The pain generator is mechanically and clinically plausible
- The provider uses image guidance and a structured plan
What evidence still doesn't settle
There are still important gaps. Studies differ in cell source, processing methods, dose, target selection, and follow-up methods. That makes broad conclusions harder than marketing materials suggest.
Clinical reality: regenerative medicine for back pain isn't "proven" in the same way as a standard, highly uniform drug trial. But it also isn't fair to dismiss it as empty hype when selected patients do show meaningful gains.
The safest interpretation is this. The field shows real potential, especially for disc-related pain in carefully screened patients, but outcomes depend heavily on diagnosis, technique, and expectations. If someone promises guaranteed relief, they're not accurately summarizing the evidence.
Your Step-by-Step Treatment and Recovery Journey
Most patients feel less anxious once they know what the process looks like. Regenerative care isn't one dramatic day. It's a sequence. The consultation matters. The procedure matters. The recovery phase matters just as much.
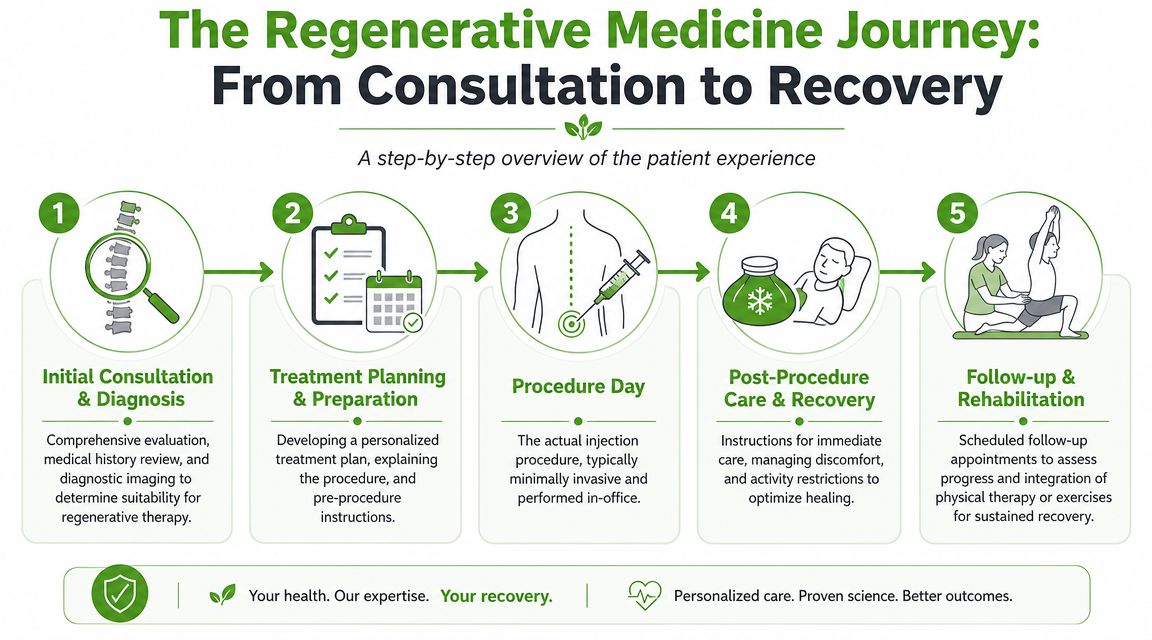
Step 1 and Step 2 evaluation before injection
The first visit should feel more like an investigation than a sales meeting. A good clinician will ask how your pain behaves. Does it worsen with sitting, extension, rotation, coughing, lifting, or getting out of bed? They will review prior treatment, imaging, past injuries, sleep, work demands, and what your body can no longer do comfortably.
Then comes treatment planning. This part often determines whether the rest of the journey makes sense. Some patients need more diagnostic clarity before anyone should discuss regenerative medicine for back pain. Others may learn that their symptoms fit muscle-driven pain, stenosis, or a surgical problem better than a regenerative one.
A thoughtful plan usually includes:
- Target selection: exactly which structure is being treated and why
- Guidance method: how the clinician plans to place the treatment accurately
- Rehab strategy: what movement, therapy, or exercise will support healing afterward
- Recovery expectations: what may improve first, and what may take longer
Step 3 procedure day
Procedure day is usually less dramatic than patients expect. Most regenerative treatments are performed in an office or procedure setting, often with image guidance so the injectate reaches the intended structure.
What you feel depends on the target tissue. Some injections are mainly pressure and soreness. Others can be more uncomfortable for a short time because irritated spinal structures are sensitive. A good team prepares you for that instead of pretending you'll feel nothing.
The procedure is only one part of treatment. Precision matters, but so does what you do with the healing window that follows.
Step 4 and Step 5 recovery and rebuilding
The first stretch after treatment is often the most misunderstood. Many patients expect immediate relief because that's what happens with a numbing injection or steroid. Regenerative treatment usually doesn't behave that way. It's trying to influence healing, so the timeline is different.
You may have soreness, stiffness, or a temporary flare before things begin to settle. Activity is often modified, not stopped completely. Later, clinicians usually reintroduce mobility work, stability training, and graded loading so the healing tissue is challenged without being irritated.
This is also where supportive options can fit in. Some patients ask about light-based therapies as part of a broader pain recovery plan. A practical primer on red light therapy for pain relief can help you understand where it may serve as an adjunct rather than a substitute for diagnosis and targeted treatment.
A typical journey often feels like this:
- Clarify the pain source so you know what is and isn't being treated.
- Receive the procedure with a clear explanation of immediate aftercare.
- Protect the area briefly while early healing signals develop.
- Rebuild capacity with guided movement and progressive exercise.
- Reassess objectively based on function, not only pain at rest.
Patients who do best usually treat the process as a partnership. The injection starts the process. Your movement habits, rehab, pacing, and follow-up help determine where it goes.
Comparing Regenerative vs. Traditional Treatment Paths
Most patients aren't choosing between "treatment" and "no treatment." They're choosing between paths that solve different problems. That is why the right comparison isn't emotional. It's practical.
Three paths and three different goals
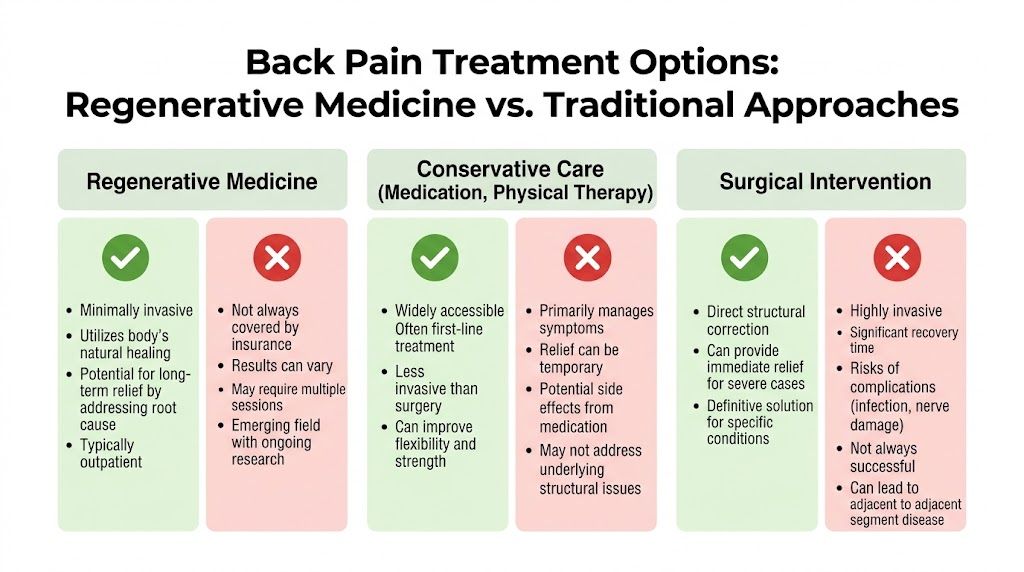
Conservative care, regenerative treatment, and surgery sit on a spectrum. None is automatically superior. Each has a different purpose.
| Treatment path | Main goal | Best fit |
|---|---|---|
| Conservative care | Reduce symptoms and improve movement | Early care, flare-ups, broad nonspecific pain |
| Regenerative medicine | Support healing in a specific painful structure | Persistent pain with a clear target and failed standard care |
| Surgery | Correct a structural problem directly | Severe compression, instability, or cases with clear surgical indication |
Conservative care usually includes physical therapy, activity modification, sleep support, anti-inflammatory strategies, and sometimes medication or standard injections. It is often the right first move because many back pain episodes improve without advanced procedures.
Regenerative medicine fits in the middle. It is typically less invasive than surgery, but more targeted than general rehab or medication. The trade-off is that it depends heavily on precision and patient selection. It also may not be covered the way standard care is.
Surgery remains essential for some conditions. If you have major instability, significant nerve compression, progressive neurologic deficit, or a problem that clearly requires structural correction, biologic treatment isn't a substitute.
What the comparison means in real life
One clinical comparison often cited in discussions of discogenic pain found that at 12 months, 67% of patients treated with intradiscal MSCs achieved clinically meaningful improvement on the Oswestry Disability Index, compared with 8% in the control group (clinical review summarizing MSC outcomes for chronic low back pain). That kind of result helps explain why some patients look to regenerative medicine when physical therapy and medication haven't delivered enough progress.
Still, this doesn't make regenerative care the default answer. It means it may be a strong option for a specific subset of people.
A simple way to weigh the trade-offs:
- Choose conservative care first when the diagnosis is still broad, symptoms are improving, or basic movement deficits haven't been addressed.
- Consider regenerative care when pain has persisted, the target structure is clearer, and you want an option between symptom management and surgery.
- Seek surgical evaluation when symptoms suggest compression, instability, or another problem that biologic treatment won't fix.
Some clinics also integrate adjunctive regenerative tools into broader musculoskeletal care. For example, Pain and Sleep Therapy Center offers regenerative approaches such as prolotherapy, PRF injections, and cold laser therapy as part of a non-surgical care model for appropriate patients.
The best treatment path is the one that matches the anatomy, the severity, and your goals. Not the one that sounds most advanced.
How to Choose a Provider and Make an Informed Decision
Provider choice changes everything in regenerative medicine for back pain. The treatment itself may be promising, but results are tied to diagnosis, technique, imaging guidance, and honesty about who should not be treated.
A strong consultation should leave you better informed, not more pressured. If you walk out with a package price but still don't understand your diagnosis, that's a problem.
Questions worth asking
Use these questions early. A qualified provider should be comfortable answering them in plain language.
- What exactly are you treating: Ask which structure they believe is causing pain. A disc, facet capsule, ligament, sacroiliac region, and muscle-driven pain pattern are not the same problem.
- How did you reach that diagnosis: You want to hear about history, exam findings, prior response to treatment, and imaging correlation. Not just "your MRI shows wear and tear."
- Will you use imaging guidance: For spine-related injections, accuracy matters. Blind placement should raise concern.
- What is the goal in my case: Pain reduction, functional improvement, activity tolerance, or delaying surgery are all different goals.
- What happens if I don't improve: Good providers discuss alternatives, not just repeat the same offer.
- What is the rehab plan after the procedure: If there is no plan for activity progression, the care may be incomplete.
If you want to review clinician background before booking, a provider page such as meet our providers can help you understand training and scope before the first visit.
Red flags patients should take seriously
Some warning signs appear again and again:
- Cure language: No ethical clinician can promise a cure for chronic back pain.
- One-size-fits-all recommendations: Different pain generators need different strategies.
- Pressure to decide immediately: Good medical decisions can survive a second opinion.
- No discussion of limits: Every legitimate treatment has trade-offs.
- No functional outcome discussion: If the only goal is "less pain," the plan may be too shallow.
The right decision often comes down to this. You want a clinician who can tell you when regenerative treatment makes sense, when it probably won't, and what they would recommend if you were their family member. That level of clarity is far more valuable than a glossy brochure.
If you're weighing regenerative medicine for back pain and want a careful, non-surgical evaluation, Pain and Sleep Therapy Center offers assessment-based care that looks at root causes and may include regenerative options when they're appropriate to the diagnosis.



