
The night after surgery is often the hardest emotionally for parents. Your child looks tired, sounds congested, may not want to eat the way they normally do, and may seem upset in ways that are difficult to soothe. That doesn't mean something is going wrong. In most cases, it means recovery from cleft palate surgery has begun exactly where it usually does: with swelling, soreness, close monitoring, and a lot of hands-on support.
What helps most is knowing what matters right now, what can wait, and what healing looks like. The palate may be surgically closed in a single procedure, but a good recovery depends on protecting that repair, keeping your child comfortable, and supporting the breathing, feeding, and speech patterns that will shape long-term function.
The First 48 Hours After Cleft Palate Surgery
The first hours after surgery can feel disorienting. Your child comes back sleepy, fussy, or both. Some children cry when they wake up from anesthesia. Some seem quiet and clingy. Others act almost like themselves, then become more uncomfortable later as the medications shift.
What the team is watching closely
In the hospital, the staff's first priorities are airway, breathing, pain control, and protection of the surgical site. Those aren't abstract goals. They're the practical reasons nurses keep checking your child even when you finally think they've fallen asleep.
They're watching for things like:
- Breathing effort: noisy breathing, congestion, pauses, or signs your child is working too hard to move air
- Comfort level: whether pain medicine is helping enough for rest, drinking, and being consoled
- Bleeding or excessive drainage: small amounts of bloody saliva can happen early, but active bleeding needs quick attention
- Hydration: wet diapers, tolerated liquids, and whether swallowing is possible without too much distress
Practical rule: If your child sounds congested, don't assume that means danger. After palate surgery, swelling and secretions are common. The question is whether they are moving air comfortably.
Arm restraints, often called “no-nos,” are also common. Parents usually dislike them at first. That reaction makes sense. But they serve one purpose that matters a lot in the first days: they help stop a child from putting fingers, toys, or hard objects into the mouth and injuring the repair.
What you can do during the hospital stay
Your job isn't to replace the medical team. Your job is to help your child stay regulated.
Try these simple actions:
- Stay physically close. Voice, touch, and familiar rhythms help more than parents expect.
- Ask before each medication change. You want to understand what your child has received and when the next dose is due.
- Use the approved feeding method only. Don't improvise with nipples, spoons, or pacifiers unless your surgeon says they're allowed.
- Hold your child upright when possible. That often helps with comfort, swallowing, and airway ease.
If you're still trying to understand the surgical side of the process, this overview of how cleft palates are repaired can help make the recovery instructions feel more logical.
A useful mindset for these first two days is this: your child doesn't need perfect calm. They need steady support and protection while the immediate swelling and discomfort settle.
Navigating the First Week at Home
Home is where many parents feel the pressure rise. In the hospital, someone is always nearby. At home, you become the scheduler, comforter, feeder, and observer all at once.
That first week goes better when you stop thinking in broad terms like “just keep them comfortable” and start thinking in systems.
Build your day around pain, fluids, and protection
The children who struggle most at home are often not the ones with the most difficult surgery. They're the ones who fall behind on pain control or hydration.
Use a written log for:
- Medication times: don't rely on memory when you're sleep-deprived
- Drinks offered and tolerated: bottle, cup, syringe, or surgeon-approved feeder
- Wet diapers or bathroom trips: one of the easiest ways to spot hydration trends
- Behavior changes: sudden refusal, unusual sleepiness, or escalating irritability
When parents tell me, “We thought they were fine, then the evening was awful,” it's often because the medication schedule drifted and discomfort caught up.
Feeding takes patience, not force
Feeding after palate surgery is often slower, messier, and more emotional. That's normal. The goal is gentle intake without trauma to the repair.
Some teams recommend tools such as a specialized bottle, a soft spouted cup, an open cup, or a syringe, depending on your child's age and the exact repair. Follow your surgeon's instructions over anything you read online. What works for one cleft team may be restricted by another.
Here's the practical divide:
| Do | Don't |
|---|---|
| Offer small, frequent liquids | Push large feeds because your child “needs to catch up” |
| Keep your child upright for feeds | Let them feed flat if that increases coughing or discomfort |
| Pause often and watch effort | Rush because the volume seems too small |
| Use only approved bottles or cups | Reintroduce pacifiers or hard nipples without permission |
| Clean the mouth gently after feeds if instructed | Scrub the palate or poke at the repair |
If you care for children often, or if grandparents and sitters will help during recovery, it's worth reviewing confident action in child emergencies. Not because complications are expected, but because calm, prepared adults make home recovery safer.
Set up one recovery zone
Don't try to manage this from every room in the house. Create one simple area with:
- prescribed medicines
- a dosing log
- burp cloths or soft washcloths
- approved feeding supplies
- extra pajamas
- a dim light for night care
That kind of setup reduces mistakes. It also helps everyone caring for your child follow the same plan.
Mastering Wound Care and Oral Hygiene
Parents often worry most when they first look inside the mouth. The palate may appear swollen, patchy, or coated with a pale film. That look can be unsettling, especially if you expected a clean pink incision.
In many cases, healing tissue doesn't look neat. It looks raw, then filmy, then gradually more settled.

What normal healing often looks like
A healing palate may show:
- swelling
- a whitish or yellowish film
- visible stitches
- mild odor from pooled saliva or milk residue
Those findings can be normal. What matters is the whole picture. Is your child drinking at least some fluids, settling with comfort measures, and acting reasonably consistent with recovery? Or are things worsening sharply?
Dissolving stitches can also look irregular before they disappear. Don't tug on anything you see. Don't test the site with a spoon, finger, or toothbrush.
How to keep the mouth clean safely
The safest oral care is usually the gentlest. Your surgeon may advise rinsing, offering sips of water after feeds, or careful cleaning at the front of the mouth while avoiding the repair itself.
Use this approach:
- Follow the exact discharge instructions first. Every repair is a little different.
- Use soft tools only if approved. A baby toothbrush or gauze may be allowed for teeth or lips, but not for the palate itself.
- Clean after feeds if instructed. The goal is reducing residue, not “scrubbing” the mouth.
- Take photos when you're unsure. A well-lit picture can help your surgeon decide whether what you see is expected.
A white healing layer is not automatically pus. Parents often fear infection when they're actually seeing normal tissue repair.
Call your surgical team sooner rather than later if you notice worsening foul odor with increasing pain, active bleeding, drainage that concerns you, or a child who suddenly refuses all intake. Those changes matter more than whether the palate looks cosmetically tidy.
Ensuring Safe Sleep and Restful Recovery
Sleep after palate surgery is rarely smooth at first. Children may wake more often, sound stuffy, or resist lying flat. Parents then face two competing worries: “My child needs rest,” and “My child sounds uncomfortable when asleep.”
Both concerns are valid. The answer is not to chase perfect sleep. It's to create the safest, calmest setup for healing.
Position, airway, and comfort work together
A child recovering from palate surgery often does better when resting in a position that supports easier breathing and drainage. Many families find that slightly more upright holding before sleep and careful crib placement after transfer help reduce the sense of “gurgly” congestion.
Use only the sleep positioning your surgeon recommends. Don't add pillows, wedges, or soft items to a crib unless your medical team specifically instructs you to do so.
These habits usually help:
- Keep the nose clear as allowed by the care team. Dried secretions can make nights harder.
- Avoid overhandling once asleep. Overtired children often sleep worse, not better.
- Watch for mouth-breathing strain. Some noisy breathing is expected, but labored breathing is not.
What “activity restriction” really means
For toddlers, “no rough play” is too vague to be useful. It should mean no activities that increase the chance of falling, mouth injury, heavy crying spells from overexcitement, or objects being shoved into the mouth.
Reasonable quiet options include:
- board books
- sticker books for older toddlers
- soft stuffed animals
- supervised drawing
- short stroller walks if approved
Nationwide Children's notes that the repaired palate should be protected from injury for about 3 weeks after surgery, which is why this period calls for more restraint than many parents expect.
Rest supports more than sleep
Good rest isn't only about mood. A calmer child tends to feed better, swallow with less struggle, and spend less time crying hard enough to dry out the mouth and irritate the repair.
This is also where airway awareness matters. Children heal best when breathing is as easy and quiet as possible. If your child already had noisy sleep, persistent congestion, or a habit of open-mouth posture before surgery, keep paying attention after the incision heals. Structural repair helps, but long-term breathing patterns may still need support.
Your Child's Healing Timeline and Milestones
The question I hear most often after the first few days is simple: Is this normal, or are we falling behind? Parents need a timeline that is realistic, not overly optimistic.
Major pediatric centers are fairly consistent on the big picture. Most children return to their usual behavior about one week after surgery, but the internal incision usually takes about 3 to 4 weeks to heal according to Cleveland Clinic's cleft lip and palate surgery guidance. That gap matters. A child can seem “back to normal” well before the palate is ready for normal activity or feeding challenges.

A practical recovery map
| Time Period | What to Expect |
|---|---|
| Day 1-7 | Soreness, swelling, feeding adjustment, closer observation, more interrupted sleep |
| Week 2-4 | Better energy, less visible swelling, ongoing protection of the palate while internal healing continues |
| Months 2-6 | Scar maturation, follow-up visits, closer attention to speech, swallowing, and oral habits |
| Beyond 6 months | Continued developmental monitoring, therapy if needed, reassessment of function rather than incision alone |
What counts as “on track”
During the first month, I look less at whether a child is cheerful every day and more at whether the trend is moving in the right direction.
Good signs include:
- taking fluids more reliably
- needing less comfort to settle
- sleeping in longer stretches
- less swelling and less guarded behavior around the mouth
Alberta Health also reports that most children are back to their usual behavior about a week after surgery, while the incision typically takes 3 to 4 weeks to heal, swelling can last 1 to 2 weeks, and pain medicine is often needed for the first few days in its cleft palate repair aftercare guidance. That pattern supports a common parent experience: your child looks better before the palate is fully healed.
If you need coordinated long-term follow-up, a dedicated cleft palate clinic can help keep surgery, speech, dental care, feeding, and airway issues from becoming separate disconnected problems.
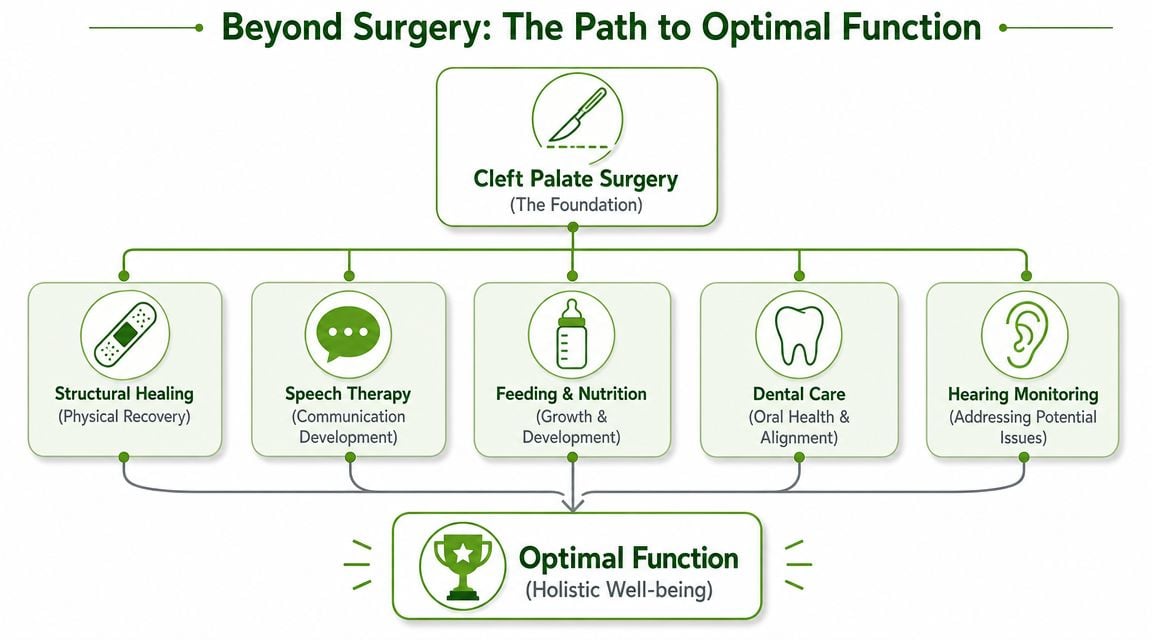
The Bridge to Optimal Function After Surgery
A closed palate is a major success. It is not the finish line.
This is the point many families are not prepared for. The incision may heal, the feeding restrictions may ease, and yet speech still sounds off, breathing may still be noisy, and swallowing patterns may still look compensatory. That doesn't mean the surgery failed. It often means your child now needs help learning how to use the repaired structures well.
Healing tissue is not the same as healed function
Speech is the clearest example. Research on secondary palate surgery for velopharyngeal insufficiency shows that functional recovery can continue for many months. In one report, improvement in hypernasality continued up to 12 months post-surgery, and the authors emphasize that neuromuscular adaptation takes time rather than happening as soon as the wound closes, as described in this ASHA Perspectives article on postoperative speech outcomes.
That changes how follow-up should work. Early speech concerns deserve attention, but premature judgment can be misleading. Children often need time, repetition, and therapy before the new anatomy performs consistently.
Structural closure gives your child the opportunity for better speech and breathing. Therapy helps turn that opportunity into function.
The pillars that shape long-term outcome
| Component | Role |
|---|---|
| Structural healing | Protects the repair and allows tissues to recover without disruption |
| Speech therapy | Builds sound production, resonance control, and more efficient use of the repaired palate |
| Feeding and nutrition | Supports growth while helping the child transition away from protective or compensatory patterns |
| Dental care | Tracks bite, eruption, arch development, and oral health over time |
| Hearing monitoring | Helps identify issues that can affect speech development and learning |
| Airway and breathing support | Encourages nasal breathing, better oral posture, and less strain during rest and function |
Why airway and myofunctional therapy belong in this conversation
Children don't use the mouth in isolated ways. Tongue posture affects swallowing. Swallowing affects pressure patterns and oral muscle habits. Oral posture affects whether a child defaults to open-mouth breathing. Breathing influences sleep quality, facial development, and even how stable speech patterns become.
That's why airway-focused care and therapy such as orofacial myofunctional therapy should not be treated as optional add-ons when a child shows persistent mouth breathing, poor tongue posture, inefficient swallow patterns, or ongoing oral muscle compensation.
What works is an integrated plan. Surgery creates structure. Speech therapy teaches sound use. Feeding support protects growth. Airway and functional therapy help the lips, tongue, palate, and breathing pattern work together instead of fighting each other.
What doesn't work is assuming that a healed incision automatically means a fully healed child.
If your child needs support beyond the surgical phase, Pain and Sleep Therapy Center offers airway-focused, root-cause care that looks at breathing, oral posture, swallowing, and functional recovery as connected pieces. For families trying to understand why speech, sleep, or mouth breathing still seem off after structural healing, that kind of multidisciplinary perspective can be a valuable next step.



