
A laser frenectomy wound typically heals in 1 to 2 weeks, and multicenter data reports a mean healing time of 9.8 ± 0.4 days. But the part many families and adult patients don't hear clearly enough is that full functional recovery often continues well beyond wound closure, because the tongue, lips, swallowing pattern, and oral muscles still need retraining after the release.
If you're reading this right after being told you or your child needs a frenectomy, you're probably balancing relief with worry. Relief that there may finally be an explanation for feeding trouble, mouth breathing, speech strain, tension, or latch issues. Worry about pain, healing, and whether the procedure will solve the problem.
That mix of emotions is normal. So is the confusion around recovery. Many people hear that a laser release is quick and heals fast, and that's true as far as the wound itself goes. The mistake is assuming that tissue healing and functional success are the same thing.
They aren't.
A laser frenectomy creates the physical freedom for better movement. It doesn't automatically teach the tongue where to rest, how to lift, or how to coordinate swallowing and speech. That's why recovery should be viewed as a journey in stages: the procedure, the wound-healing phase, the stretching phase, and then the retraining phase.
Understanding Your Frenectomy Recovery Journey
A common recovery story starts the same way. The procedure is quick, the release looks good, and a parent expects feeding to improve by the next day, or an adult expects speech or tension to change as soon as the restriction is gone. Then the wound starts healing on schedule, but function still feels awkward, inconsistent, or tiring.
That does not mean the procedure failed. It usually means the mouth is in the middle of two different jobs at once. The tissue has to heal, and the tongue or lip has to learn a new pattern of movement.
Laser frenectomy recovery is usually measured in stages. Clinical guidance from the American Academy of Pediatric Dentistry policy on management of the frenulum supports the general expectation that the surgical site often heals over the first 1 to 2 weeks, while many clinicians prescribe stretches and active wound care for several weeks to limit reattachment and preserve mobility. That longer phase matters because a successful release depends on what the patient does with the new range of motion.
I explain this early because it prevents a lot of unnecessary worry. A site can look much better before feeding is organized, before tongue-to-palate suction feels natural, or before oral rest posture improves. In infants, that may mean latch gets easier in steps rather than all at once. In children and adults, it can mean better movement without immediate changes in chewing, speech clarity, nasal breathing, or muscle tension.
Clinics that discuss tongue-tie treatment in the context of feeding and oral function, including resources like Skotzko Family Dental Clinic, often prepare families better for that reality. The release creates access to normal movement. Functional recovery comes from healing plus retraining.
If you are preparing for treatment, a clear overview of a pediatric frenectomy helps set expectations about what the procedure changes physically and what still depends on aftercare, stretches, and therapy.
A frenectomy starts the process of better oral function. It does not complete it.
Wound healing versus functional healing
These are related, but they are not the same.
Wound healing is the biological process. The tissue closes, matures, and remodels.
Functional healing is the behavioral and muscular process. The patient learns to use that new mobility for better latch, tongue elevation, lip seal, swallowing, speech, and oral rest posture.
This distinction is often overlooked, and it is one of the main reasons people feel confused after an otherwise well-performed release. Orofacial Myofunctional Therapy, or OMT, addresses that gap by helping the tongue and surrounding muscles use the new freedom correctly. In practice, the best outcomes usually come from treating the frenectomy as the first procedural step in a broader plan, not as a stand-alone fix.
Families and adult patients do better when they ask two separate questions from the start:
- How long until the wound looks and feels healed?
- How long until feeding, speech, breathing, or tension patterns improve?
Those answers are often different, and knowing that early makes recovery much easier to handle.
Your Healing Timeline Day by Day and Week by Week
A common recovery pattern looks like this. The procedure goes smoothly, the site looks more dramatic on day two than it did on day one, and patients worry that something is wrong just as the mouth is doing what it should.
Healing after a laser frenectomy is usually predictable in sequence, even when the exact pace differs by age, anatomy, and how consistently exercises and feeding or speech work are done. Laser procedures are often associated with good visibility, limited bleeding, and a relatively short early recovery period, which is one reason many clinicians prefer them for tongue-tie and lip-tie release (Pioon clinical overview of laser frenectomy).
What you may notice early on
Right after the procedure, the released area often looks open, moist, and diamond-shaped. Within the next one to two days, a white or yellow-white layer usually forms over the site. That layer is commonly fibrin, a normal part of wound healing, not pus or an automatic sign of infection. The appearance can be unsettling if nobody warned you.
Movement often feels strange before it feels better.
That matters because the mouth is adapting to a new range of motion at the same time the tissue is closing. Infants may latch differently before they latch better. Children may move the tongue more but still struggle to coordinate it. Adults often notice improved mobility before they notice smoother swallowing, speech, or oral rest posture.
Practical rule: Watch the overall direction. Mild soreness, a white healing layer, and temporary clumsiness are common. Increasing redness, swelling, bleeding, fever, or refusal to eat warrants a call to your provider.
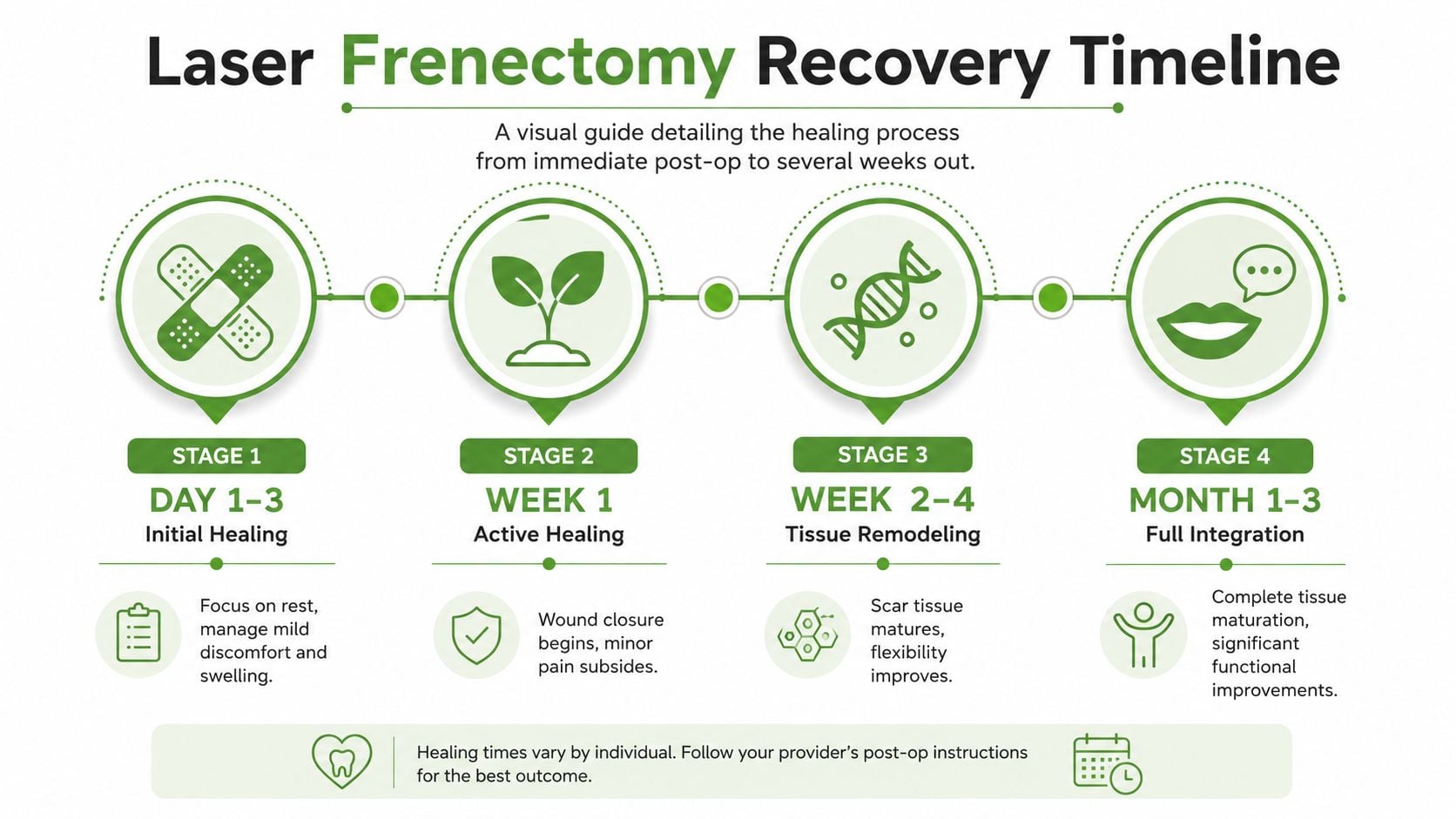
Laser Frenectomy Healing Timeline
| Timeframe | Wound Appearance | Expected Discomfort | Functional Notes (Feeding/Speech) |
|---|---|---|---|
| 0 to 48 hours | Fresh release site. A white or yellow-white healing layer often begins to appear | Usually mild to moderate soreness | Infants may feed unevenly at first. Older children and adults often feel that tongue or lip movement is unfamiliar |
| Days 3 to 7 | Surface tissue starts to organize and close. The area still looks different from surrounding tissue | Soreness often eases, though stretching and movement may remain tender | Many patients return to normal routines. Better mobility may be noticeable, but coordination is still developing |
| Weeks 2 to 4 | Ongoing remodeling. Color and texture gradually become less obvious | Daily discomfort is usually low, though exercises may still feel uncomfortable | Consistent retraining matters here. Feeding, speech, swallowing, and oral posture improve more reliably when mobility is practiced correctly |
| Month 1 to 3 | Tissue continues to mature and soften | Pain is usually no longer the main issue | Muscle patterns, rest posture, speech clarity, and swallowing mechanics may continue improving, especially with OMT or other guided therapy |
Pediatric and adult timelines differ
Children often close the wound quickly. Infants and younger children may also look improved before they have fully integrated the new movement into feeding, sleep, and oral habits. Parents sometimes interpret that mismatch as failed treatment, when it more often reflects a coordination lag.
Adults usually heal well too, but recovery tends to feel less uniform. The tissue may settle early while long-standing compensation patterns remain. Jaw tension, shallow tongue posture, mouth breathing habits, and guarded swallowing often take longer to change than the wound takes to close. Adult healing guidance from the American Association of Oral and Maxillofacial Surgeons on frenectomy reflects that broader point. The procedure is brief. Functional adaptation can take longer.
The part many people underestimate
A closed wound is only one milestone.
The larger question is whether the tongue or lip starts working better in real tasks. Can the infant transfer milk more efficiently. Can the child maintain better lip seal and tongue posture. Can the adult swallow without neck tension, rest with the tongue up, or speak without compensating?
Those changes usually do not happen on tissue healing alone. They improve when the release is followed by purposeful retraining. That is why I tell families and adult patients to track two timelines from the start. One is for the wound. The other is for function. The second one is often longer, and it has more to do with exercises, feeding support, and Orofacial Myofunctional Therapy than with the procedure itself.
Managing Discomfort and Supporting Oral Function
The first evening after a laser frenectomy is often the point when families and adult patients start second-guessing the decision. The area looks raw, movement feels unfamiliar, and eating or feeding may seem less coordinated before it gets better. That early phase is usually part of normal recovery.
Pain is often manageable, but the mouth can feel sore, tight, or mildly stinging for several days. Many adults describe it as similar to a fresh burn from hot food. A white or yellow film can also appear over the release site within the first day or two. The American Academy of Pediatric Dentistry notes that this fibrin layer is part of normal healing after oral procedures, not a sign of infection by itself (AAPD policy and guidance on management of the frenulum).

Comfort matters because it affects function. A patient who is too sore to latch, swallow, speak, or do gentle wound care is more likely to guard the area. Guarding creates tension, and tension can interfere with the very movement the release was meant to improve.
What usually helps
Simple measures work well when patients use them consistently.
- Use approved pain relief: Adults often do well with acetaminophen or ibuprofen if their physician says those medicines are safe for them.
- Choose bland, soft foods: Yogurt, smoothies, eggs, mashed vegetables, soups that are warm rather than hot, and other easy foods are often more comfortable early on.
- Drink fluids often: A dry mouth makes soreness more noticeable and can make tongue movement feel rougher.
- Use cold strategically: Cool liquids, chilled foods, or an ice pack on the face can reduce soreness in the first day or two.
- Keep movement gentle and regular: Light, appropriate movement usually supports recovery better than protecting the area all day.
Some practices also pair recovery with adjunctive light-based care. For clinicians evaluating options, effective laser therapy for clinics may be part of a broader post-procedure support plan, but it does not replace skilled aftercare, feeding support, or myofunctional retraining.
Feeding and speech often feel different before they feel better
Infants may have more tongue mobility right away and still feed inconsistently for a period of time. The tongue has to coordinate a new range of motion with sucking, swallowing, and breathing. Parents should expect practice, not instant efficiency.
Older children and adults often notice temporary changes in speech, saliva control, chewing, or swallowing. Tongue-tip sounds may feel awkward. Resting posture may feel strange. Some patients even report that the floor of the mouth feels tired because the muscles are finally being asked to move in a different way.
That does not mean the procedure failed. It usually means the nervous system is adjusting to a movement pattern it has not used well before.
What tends to slow progress
A few habits make recovery harder than it needs to be:
- Eating sharp, spicy, acidic, or very hot foods too soon
- Letting fear stop all tongue or lip movement
- Skipping stretches or oral exercises that were prescribed
- Assuming wound closure alone means function has returned
This last point matters. A frenectomy creates access to better movement. It does not teach the tongue, lips, and jaw how to use that movement well. If soreness is managed and the wound is healing, the next job is purposeful retraining through feeding work, speech support when needed, and Orofacial Myofunctional Therapy. That is where many of the lasting gains in latch, tongue posture, swallowing, and oral rest posture develop.
Key Factors That Influence Recovery Speed
No two patients have the same laser frenectomy recovery time. The procedure may be similar, but the biology and the habits behind the restriction are not.
Age is one of the biggest variables. Infants often heal rapidly because their tissues regenerate quickly and they haven't had years to build compensatory patterns. Adults and adolescents usually have denser tissue, more muscle tension, and more established movement habits.
Why adults often need more patience
A 2025 clinical study found that 42% of adult patients reported persistent discomfort beyond day 7, which pushes back against the overly simple idea that adult recovery is always quick and straightforward (Dr. Jesse Witkoff on frenectomy recovery time). That doesn't mean the procedure is failing. It means adult recovery often needs more realistic expectations and better support.
Adults also tend to notice secondary issues more clearly. They may feel tongue fatigue, floor-of-mouth tightness, altered speech mechanics, or jaw guarding as the system adapts. Patients with facial pain, clenching, or airway-related tension often need especially careful follow-up.
Other variables that matter
Recovery is shaped by more than age alone.
- Baseline muscle tension: A tightly braced jaw or tongue often slows comfortable adaptation.
- General health and immune response: Healthier tissue tends to recover more smoothly.
- Type and severity of restriction: Some releases create a more dramatic functional change than others.
- Consistency with aftercare: This is often the difference between steady improvement and preventable setbacks.
In some practices, adjunctive approaches are also discussed as part of broader tissue support and pain care. For clinicians exploring supportive modalities, information on effective laser therapy for clinics can be useful background, especially when treating patients with pain-sensitive oral and facial tissues.
The factor patients control most
Technique matters. Biology matters. But the variable patients control most is adherence.
A beautifully performed release can still heal in a less functional way if the patient doesn't follow the postoperative plan. On the other hand, a patient with slower tissue healing can still achieve a strong outcome when aftercare, exercises, and follow-up are handled consistently.
That's why recovery should never be described as passive. The body heals. The patient participates.
Your Step-by-Step Guide to Aftercare and Stretches
The hardest point for many families is not the procedure day. It is the first evening at home, when the wound looks different than expected, the baby cries during stretches, or an adult wonders whether normal soreness means they should stop moving the area. In most cases, that is the moment that determines how well the release heals functionally.
Aftercare has two jobs. It protects the surgical site, and it helps the tissue heal with the mobility gained during the release. If the wound closes without guided movement, the mouth can slip back toward the same restricted pattern that caused symptoms in the first place.
A practical home plan usually includes wound care, pain control, feeding or diet adjustments, and a set of stretches your clinician has demonstrated. The stretch phase often continues for several weeks during active healing, and pediatric tongue-tie aftercare guidance from University of Mississippi Medical Center describes repeated post-release exercises as part of preventing the tissue from healing back together.

The daily priorities
Most plans are personalized, but the same four priorities come up again and again.
Keep the area clean enough to heal well
Gentle oral hygiene limits debris and lowers the chance of extra irritation. Follow the cleaning instructions you were given rather than inventing a stronger routine.Do the assigned stretches on schedule
This is what keeps the wound from sealing in a less mobile position. Skipped sessions are one of the most common reasons a release heals with less improvement than expected.Control discomfort well enough to allow normal movement
If a patient is too sore to move the tongue or lip, they often guard, clench, or avoid feeding and speaking normally. That can reinforce the old compensation pattern.Choose foods and feeding methods that do not keep re-traumatizing the site
Soft, easy-to-manage foods usually make the first few days simpler for older children and adults. Infants may need temporary feeding support while latch and tongue motion are adjusting.
How to approach stretches
Stretches should be deliberate and specific. They should open the wound enough to keep the released surfaces from sticking back together, without rough handling.
Use these principles at home:
- Wash your hands first: Clean technique matters.
- Follow the exact demonstration: Shallow stretches often look correct but do very little.
- Stay consistent through the day: Missing several sessions and doing extra later is usually less effective.
- Expect some protest in infants: Brief crying does not automatically mean injury.
- Ask for another teaching visit if needed: Parents should not have to guess.
For patients who need more visual guidance, a dedicated set of frenectomy exercises can help reinforce proper technique between visits.
The larger goal is function, not just wound appearance. A nicely healing site is only part of success. The tongue, lip, jaw, and swallowing pattern also need repeated, correct use so the new range of motion becomes part of daily function.
The stretches are part of treatment. They support the result your procedure created.
A visual walkthrough can also help families feel more confident with the home routine:
What helps families stay consistent
The families who stay on track usually build the routine into the day instead of relying on memory.
- Pair stretches with existing habits: after feeds, diaper changes, meals, or brushing teeth.
- Use a checklist: This is especially helpful when multiple caregivers are sharing the schedule.
- Keep the approach calm and brief: Children read caregiver tension quickly.
- Show up for follow-up visits: Early reattachment can be subtle before symptoms are obvious.
- Address other oral habits during recovery: If you also need to help your child stop thumb sucking, reducing that extra oral tension can make healing and retraining easier.
Good healing and good function are related, but they are not identical. The procedure creates access to better movement. Aftercare and repeated oral use help preserve it.
Why Full Recovery Includes Orofacial Myofunctional Therapy
A successful release gives tissue more freedom. It does not automatically change years of compensation.
That's the missing piece in many conversations about laser frenectomy recovery time. Patients are often told when the wound will close, but not what it takes to convert that new mobility into better breathing, swallowing, chewing, speech, and oral rest posture.
Emerging data suggests that 60 to 70% of post-frenectomy patients fail to achieve optimal oral function without structured therapeutic follow-up, especially adults and older children who have built long-standing compensatory motor habits (Enclave Dental on questions to ask before frenectomy treatment).
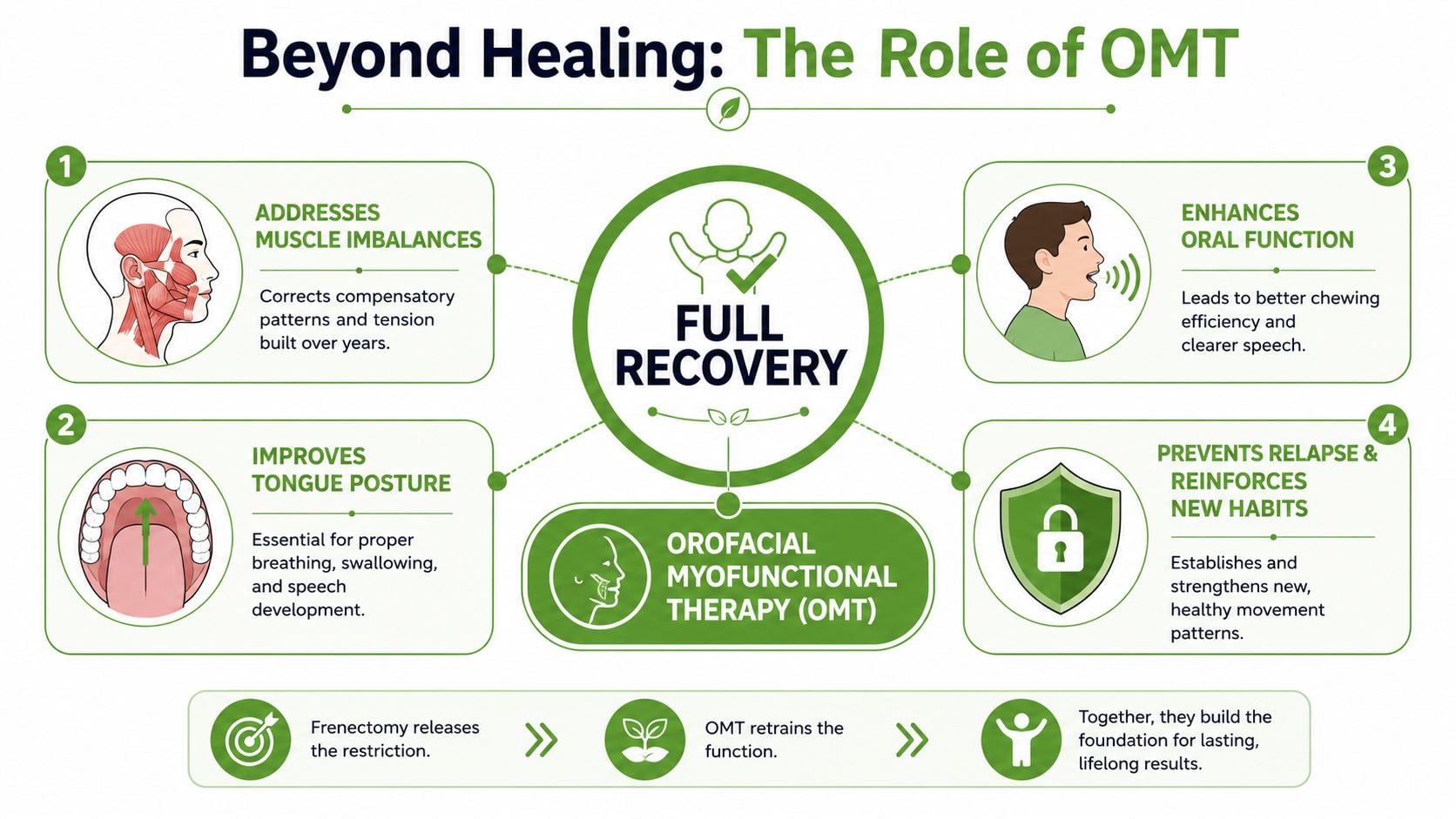
What Orofacial Myofunctional Therapy actually does
Orofacial Myofunctional Therapy, or OMT, retrains the muscles of the tongue, lips, cheeks, and face to work in a healthier pattern. That includes:
- Tongue posture: Teaching the tongue to rest where it should, not where it learned to compensate.
- Swallowing mechanics: Reducing patterns like tongue thrust or excessive lip and chin recruitment.
- Breathing habits: Supporting nasal breathing over chronic open-mouth posture.
- Muscle balance: Lowering unnecessary tension that can continue even after the restriction is released.
If you're unfamiliar with the process, a plain-language explanation of orofacial myofunctional therapy is a useful place to start.
Why the release alone may not solve the problem
A tongue-tie can restrict movement for years. During that time, the body adapts. The patient learns workarounds. Muscles recruit in unusual ways. The jaw may brace. The lips may overwork. Breathing and swallowing can shift into less efficient patterns.
Once the tie is released, those old habits don't disappear on command.
That's especially true in older children and adults. They often need structured repetition to build a new default. Without that retraining, it's common to see patients with improved mobility but incomplete functional change.
Better motion is an opportunity. OMT is how many patients learn to use that opportunity well.
Who benefits most from therapy
OMT is especially valuable when the patient has signs of long-standing compensation, such as mouth breathing, unusual swallowing patterns, speech strain, facial muscle tension, or persistent oral habits. Parents who are already working on broader oral habits may also find related guidance helpful, including ways to help your child stop thumb sucking, since habit patterns and oral muscle function often overlap.
In practical terms, the best outcomes usually come from treating the release and the retraining as one coordinated process. That's the difference between a healed site and a changed system.
Recognizing Complications and Planning Your Follow-Up
A common recovery scenario looks like this. The site develops a white or yellow healing layer, stretches feel uncomfortable for a few seconds, and function seems uneven before it improves. Those changes are often part of normal healing.
What deserves attention is a recovery pattern that is drifting in the wrong direction. I tell patients and parents to watch the trend, not a single moment. Day by day, the site should look calmer, pain should become easier to manage, and oral function should gradually open up with practice.
Signs to contact your provider
- Bleeding that does not settle: More than light spotting, or bleeding that restarts and does not slow with pressure.
- Signs of infection: Pus, fever, worsening redness, or swelling that is increasing instead of easing.
- Poor intake: An infant who cannot feed, or an older child or adult who is drinking so little that hydration becomes a concern.
- Loss of mobility after early gains: If the tongue or lip moved better at first and then starts feeling restricted again, the site may need to be checked for reattachment.
- Pain that is escalating: Soreness is expected. Pain that keeps intensifying is not.
Follow-up visits matter because wound healing and function do not always progress at the same pace. Tissue can look acceptable while the patient is still struggling with latch, tongue elevation, speech coordination, or oral rest posture. The visit gives the clinician a chance to assess both.
Many practices schedule the first post-procedure check within about a week, often around 7 to 10 days, which aligns with common postoperative instructions in oral surgery care pathways from the University of Mississippi Medical Center. That timing is useful because early healing changes are visible, stretch technique can be corrected if needed, and functional setbacks can be addressed before they become habits again.
This is also where the bigger picture becomes clear. Some patients need reassurance that healing is on track. Others need better pain control, feeding guidance, or a more precise home routine. Many need continued Orofacial Myofunctional Therapy so the new mobility turns into better swallowing, tongue posture, breathing patterns, and speech use.
Good outcomes come from treating follow-up as part of the procedure, not a separate extra step.
If you're looking for a team that evaluates frenectomy recovery in the larger context of oral function, airway, muscle tension, and sleep-related symptoms, Pain and Sleep Therapy Center offers multidisciplinary care for infants, children, and adults. Their approach goes beyond wound healing alone, with support for myofunctional therapy, breathing patterns, TMJ-related tension, and the functional habits that often determine whether a release delivers its full benefit.



