
You may be reading this because your jaw clicks every time you chew, or because you keep waking up with a headache that feels like it started somewhere behind your cheekbones. Maybe your dentist said your teeth show signs of grinding. Maybe your neck is always tight, your ears feel full, and you've started to wonder whether these problems are connected.
They often are.
When patients ask, what is TMJ disorder, they're usually asking about more than one symptom. They're asking why their jaw feels off, why their face hurts, why sleep isn't refreshing, and why the problem keeps coming back after pain medicine wears off. The short answer is that TMJ disorder, also called TMD, involves dysfunction in the jaw joints, the muscles that move them, and the surrounding systems that influence how the jaw works every day.
That Clicking Jaw and Persistent Headache
A common story goes like this. A person notices a small click on one side of the jaw. It doesn't seem urgent. Then chewing tougher foods becomes annoying. A few weeks later, morning headaches start showing up, or the jaw feels tired by late afternoon, or the neck gets tight after a stressful day. Because each symptom seems minor on its own, many people wait.
That delay is understandable. TMJ symptoms rarely announce themselves in a dramatic way at first. They build through repetition. Clenching at night. Holding tension in the face. Sleeping with the mouth open. Pushing through a busy schedule while the joint and muscles absorb more strain than they can recover from.
Why this problem is so often overlooked
TMJ disorder can look like several different problems at once. Some people think they have a sinus issue. Others assume they just need a softer pillow or a different headache remedy. Some only notice the noise and ignore the pain until the jaw starts feeling unstable.
If that sounds familiar, you're not alone. In the United States alone, approximately 12% of the population, or roughly 35 million people, are affected by TMJ disorders, and it is the second most common painful musculoskeletal condition after lower back pain according to the Journal of Oral and Facial Pain and Headache review.
For many people, the first sign is clicking. If that's your main symptom, this explanation of why your jaw clicks can help you understand what that sound may mean.
Many jaw noises are not dangerous by themselves. Jaw noises paired with pain, limited motion, or headaches deserve a closer look.
The reassuring part
TMD is real, common, and treatable. A sore jaw doesn't mean you're headed straight toward surgery. It does mean your body is giving you useful information. The key is to stop treating the symptoms like separate mysteries and start looking at the jaw as part of a larger system that includes breathing, sleep, muscle balance, and posture.
Understanding Your Jaw's Complex Anatomy
The temporomandibular joint is one of the busiest joints in the body. You use it to talk, chew, swallow, yawn, and stabilize the lower face. It has to open, close, glide, and adapt to small shifts in muscle tension all day long.
A simple hinge doesn't capture how it works. The TMJ is more like a hinge plus a sliding track. The lower jawbone, called the mandible, meets the skull at the temporal bone, and between them sits a small articular disc that acts like a cushion and guide.
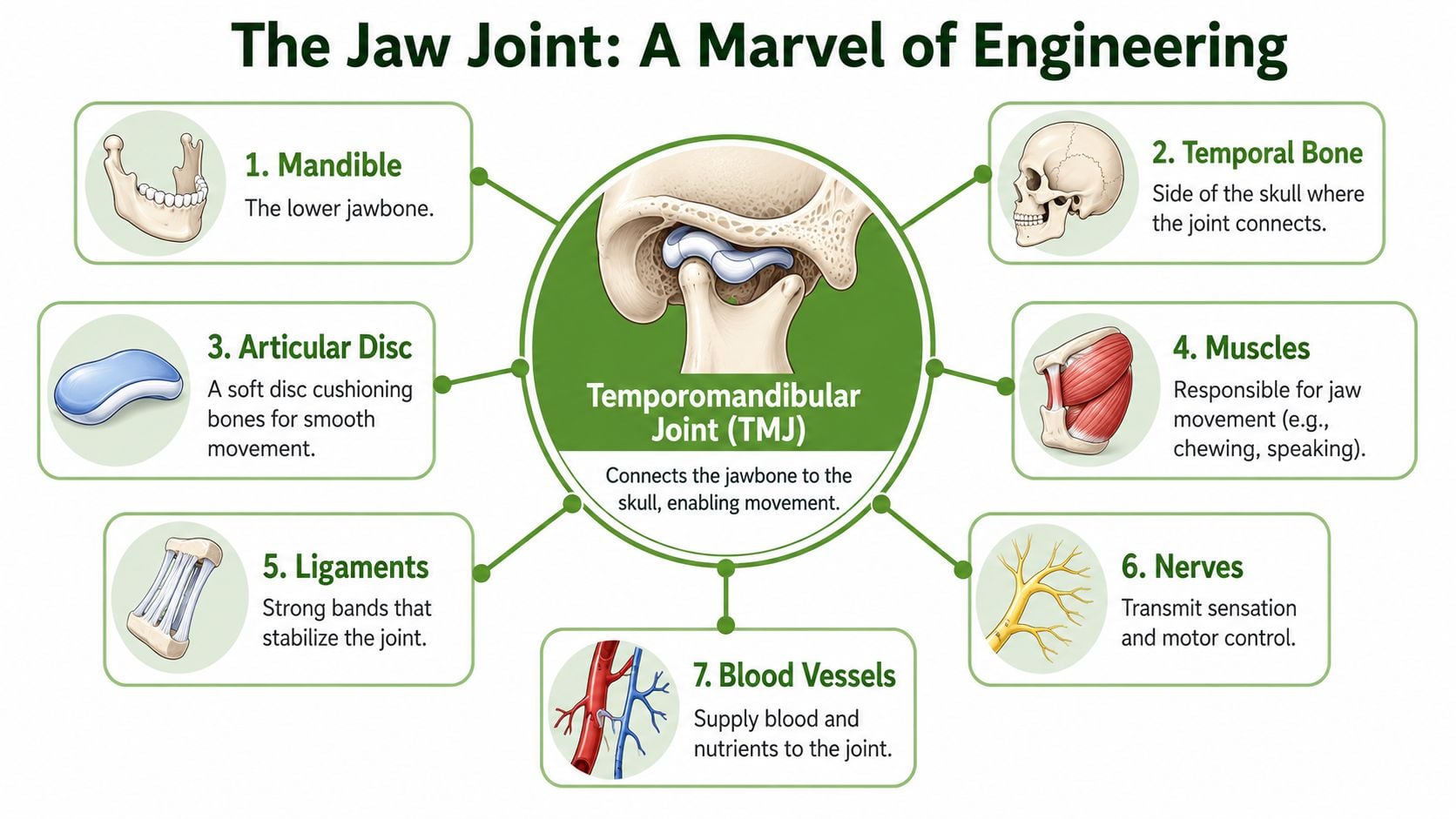
What makes the TMJ so vulnerable
This joint is small, but the forces placed on it are not. Every time you clench, grind, chew hard foods, or hold your lower jaw in a strained position, the disc, ligaments, cartilage, and muscles have to absorb that load.
A healthy TMJ depends on several parts working together:
- The disc keeps motion smooth and helps separate the bony surfaces.
- The muscles generate motion and can also create pain when overworked.
- The ligaments stabilize the joint and limit excessive movement.
- The nerves and blood supply support function and help explain why irritation in this area can feel intense.
Why anatomy matters for symptoms
When the disc tracks poorly, people may hear clicking or popping. When the muscles around the joint stay tight, the pain may feel more like a headache, temple ache, or cheek soreness than “jaw pain.” When joint motion gets restricted, yawning and chewing become difficult.
Practical rule: If a symptom gets worse with chewing, wide opening, clenching, or waking in the morning, the jaw system should be part of the evaluation.
This is why a good TMJ exam doesn't stop at the joint itself. The specialist has to look at how the jaw moves, how the bite meets, how the tongue rests, and whether breathing patterns are overloading the system.
The True Root Causes of TMJ Pain
The biggest mistake people make is assuming TMJ disorder has one cause. It usually doesn't. TMJ disorder is a multifactorial disease driven by the mechanical overload of the joint, which disrupts the balance of cartilage cell activity. This process is influenced by muscle dysfunction, trauma, and even psychosocial stressors like anxiety, which can worsen inflammation and pain as described in the Journal of Oral Medicine and Pain review.
That phrase, mechanical overload, matters. It means the joint is being asked to tolerate more force, tension, or instability than it can handle well.
Structural and injury-related factors
Some TMJ cases start after a clear event. A fall. A car accident. A difficult dental procedure with prolonged opening. A direct blow to the jaw. In other cases, the problem grows from anatomy and function over time, especially when the joint has to compensate for an unstable movement pattern.
Common structural contributors include:
- Disc derangement: The cushioning disc may not move as cleanly as it should.
- Joint inflammation or degeneration: Cartilage and bone can become irritated under repeated load.
- Old trauma: Even if the injury seemed minor at the time, the joint may have adapted poorly.
Muscle overuse is often the daily driver
For many adults, the strongest day-to-day trigger is muscle tension. Clenching and grinding are obvious examples, but they're not the only ones. People also overload the jaw by bracing the teeth together during concentration, keeping the tongue low in the mouth, or breathing through the mouth during sleep.
These patterns matter because they change where the jaw rests and how hard the surrounding muscles have to work. If the tongue doesn't support the palate and the lips don't stay comfortably sealed, the jaw often drifts into a less stable position. The neck and shoulder muscles then join the compensation.
The hidden links with breathing, sleep, and posture
Many patients finally find answers. A jaw that hurts every morning may not just be a jaw problem. It may be reacting to poor-quality sleep, nighttime clenching, airway strain, or a forward-head posture that changes how the jaw hangs at rest.
Consider the chain:
- Mouth breathing can dry tissues, alter oral posture, and encourage a lower jaw position that strains the joint.
- Sleep-disordered breathing can trigger protective muscle activity at night, including clenching.
- Forward-head posture can change muscle tone from the neck to the jaw.
A jaw joint rarely suffers in isolation. The airway, the tongue, the neck, and sleep quality often leave fingerprints on the problem.
Stress also plays a role, but not in the oversimplified way people often hear. Stress doesn't mean the pain is “just emotional.” It means the nervous system can amplify guarding, clenching, and pain sensitivity, which can keep a mechanical problem active longer.
Recognizing the Wide-Ranging Symptoms of TMD
Some TMJ symptoms are easy to connect to the jaw. Others are not. That's why many people bounce between providers before someone finally sees the full pattern.
The most direct symptoms include jaw pain, facial soreness, clicking, popping, grinding sensations in the joint, and difficulty chewing. Some people feel stiffness on waking. Others notice the jaw deviates to one side when opening. A few experience episodes of locking, where the mouth won't open or close normally for a period of time.
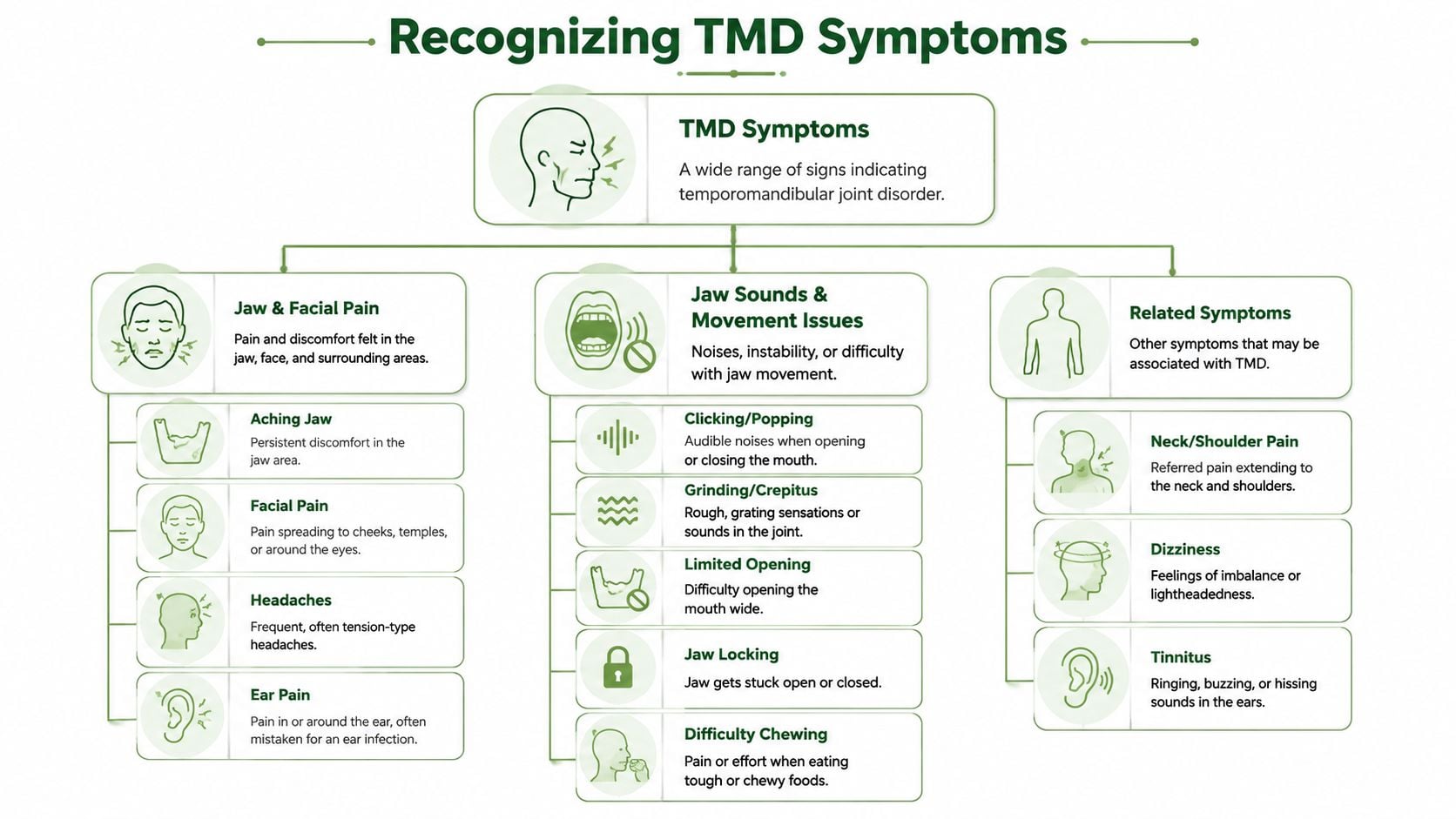
Symptoms that don't seem like jaw symptoms
The confusion starts when pain travels. The jaw muscles and joints share close relationships with the temples, ears, cheeks, and neck. That means irritation in one area can be felt somewhere else. This is called referred pain.
Patients commonly describe:
- Temple headaches: Often mistaken for tension headaches or migraines.
- Ear discomfort: Fullness, aching, or pressure without an obvious infection.
- Neck and shoulder tension: Especially when jaw strain and posture issues coexist.
- Tinnitus or dizziness: Less intuitive, but sometimes part of the pattern.
What symptoms tend to show up together
Rather than looking for one perfect symptom, it helps to notice clusters. TMD often looks like combinations such as:
| Symptom cluster | What patients often notice |
|---|---|
| Morning pattern | Jaw soreness, headache, teeth feel tender, fatigue on waking |
| Chewing pattern | Pain with gum, steak, crunchy foods, tiredness after meals |
| Posture pattern | Jaw tension plus neck tightness at desk work or driving |
| Ear pattern | Fullness, ringing, or pressure that doesn't behave like an infection |
If chewing hurts, it's also worth considering whether the teeth themselves are part of the story. Mouthology explains tooth pain causes in a way that helps people distinguish dental sensitivity from pressure-related pain that can overlap with jaw dysfunction.
Why accurate diagnosis matters
Not every face or jaw pain problem is TMD. Tooth fractures, sinus conditions, nerve pain, and certain headache disorders can mimic parts of it. That's why a proper evaluation matters. The goal isn't to label every symptom as “TMJ.” The goal is to identify whether the jaw is the source, a contributor, or an innocent bystander.
When symptoms spread across the jaw, ears, temples, and neck, guessing usually prolongs the problem.
How Specialists Diagnose TMJ Disorders
A good TMJ evaluation should feel methodical, not rushed. The process usually starts with listening. When did the symptoms begin? Is the pain worse in the morning or later in the day? Does chewing trigger it? Do headaches, snoring, poor sleep, or neck tension show up alongside the jaw pain?
Those details matter because they reveal patterns. An overworked muscle problem behaves differently from an inflamed joint. A breathing-related clenching pattern often sounds different from pain after an injury.
What happens during the exam
The physical exam usually includes several parts:
- Jaw movement testing: The clinician looks at how wide you open, whether the jaw deviates, and whether opening is smooth or guarded.
- Muscle palpation: Gentle pressure helps identify overactive or tender muscles in the jaw, temples, neck, and face.
- Joint loading checks: Certain movements help reveal whether the pain is more muscular, intra-articular, or both.
A specialist may also assess habits and function. That includes daytime clenching, tongue posture, lip seal, swallowing pattern, and whether your breathing looks nasal or mouth-dominant at rest.
Why modern diagnosis looks beyond the jaw
A narrow exam can miss the reason the problem keeps returning. If a person has poor nasal breathing, fragmented sleep, or posture that constantly drags the head forward, the jaw is forced to compensate over and over again.
That whole-system perspective is why many patients benefit from seeing an orofacial pain specialist rather than relying on a quick screening alone.
When imaging becomes useful
Imaging isn't necessary in every case, but it can be very helpful when the history suggests joint damage, asymmetry, trauma, degenerative change, or an internal derangement that needs a closer look. Cone Beam Computed Tomography, often called CBCT, can help evaluate bony structures in more detail than a simple visual exam.
The best diagnosis combines three things: symptoms, hands-on findings, and imaging when indicated. That's how treatment gets individualized instead of guessed.
Healing Your Jaw Without Surgery
Most patients feel relieved when they learn this: approximately 80% of patients with TMJ disorders achieve symptom resolution through non-surgical interventions, with treatment focused on reducing joint overload and controlling habits like clenching, while surgery is reserved for severe refractory cases according to UT Health San Antonio's TMJ guidance.
That matters because too many people assume they have only two options. Live on pain medication or eventually have surgery. In practice, there's a much broader middle ground.

Start with load reduction and stability
The first job is to calm the system down. That usually means reducing the forces that keep irritating the joint and surrounding muscles.
Common first-line strategies include:
- Custom oral appliances: These can help reduce strain from clenching and create a more stable jaw position in selected cases.
- Temporary diet changes: Softer foods for a period can decrease aggravation while tissues settle.
- Heat and movement care: Moist heat and guided exercises can reduce guarding and improve motion.
- Behavior changes: Keeping teeth apart during the day and avoiding gum chewing often helps more than people expect.
What doesn't work well is chasing short-term symptom suppression while ignoring the drivers. Repeatedly taking pain relievers without changing load, breathing, posture, or oral habits often leaves patients stuck in a flare cycle.
Modern care can go beyond symptom masking
When inflammation lingers or tissues need more support, many clinicians now use non-surgical therapies designed to encourage healing rather than mute pain.
Cold laser therapy is one option. It's used to calm irritated tissues and support recovery in a low-force way. Patients generally appreciate that it's noninvasive and easy to combine with other treatment.
A newer category involves regenerative treatment. Therapies such as prolotherapy and Platelet-Rich Fibrin, or PRF, aim to stimulate the body's own repair response in areas that have become chronically irritated or unstable. In the right patient, that's a very different goal from numbing the problem.
If you want a focused overview of that approach, this page on orthobiologic therapy explains how regenerative options are used in jaw and facial pain care.
The best non-surgical plan doesn't just ask, “How do we lower pain today?” It asks, “Why is this joint being overloaded in the first place?”
Lasting relief usually requires functional correction
Even a well-made appliance won't solve everything if the tongue posture is poor, the patient mouth-breathes at night, or the neck and jaw stay in a guarded pattern all day. Long-term stability often comes from retraining function.
That may involve:
- Orofacial myofunctional therapy to improve tongue posture, swallowing, and lip seal
- Breathing retraining to support nasal breathing and reduce compensatory tension
- Targeted physical therapy for jaw, neck, and upper shoulder coordination
A brief visual explanation can help make that treatment path easier to picture.
What surgery is actually for
Surgery has a place, but it's not the usual starting point. It's usually considered when conservative care has been done well and the patient still has significant structural dysfunction, persistent locking, or refractory pain that matches the imaging and clinical findings.
For many patients, the better path is less dramatic and more effective. Calm the overload. Improve stability. Support tissue healing. Restore healthier breathing and muscle function. That's how jaw problems stop acting like they're “mysteriously” coming back.
Your Questions About TMJ Treatment Answered
When should I see a specialist instead of waiting?
If symptoms are mild and short-lived, simple self-care may help. If the pain keeps returning, chewing becomes difficult, headaches are frequent, or your jaw locks, it's time for a proper evaluation. You should also seek help sooner if the problem is tied to trauma, sleep disruption, or significant ear and neck symptoms.
What should I expect at the first visit?
Expect a conversation that is more detailed than a routine dental check. A thorough clinician will want to understand your pain pattern, sleep quality, oral habits, jaw function, headache history, and breathing pattern. You should also expect a hands-on exam of the jaw joints, muscles, bite, and related structures.
Will I automatically need an appliance or injections?
No. Good care is individualized. Some patients need habit correction and targeted exercises first. Others benefit from an appliance, physical therapy, laser treatment, or regenerative support. The plan should match the actual driver of your symptoms, not a one-size-fits-all protocol.
Is medication enough for TMJ pain?
Medication may help during a flare, but it usually doesn't correct the reason the flare keeps happening. If the jaw is being overloaded by clenching, poor tongue posture, sleep-related breathing issues, muscle imbalance, or joint instability, pain medicine alone won't fix that pattern.
What makes treatment more successful?
Patients do best when the provider looks at the jaw as part of a connected system. Relief tends to be more durable when treatment addresses joint mechanics, muscle behavior, breathing, sleep, and posture together rather than treating each symptom separately.
What if I've already tried a night guard and it didn't help?
That doesn't mean the problem is untreatable. It often means the diagnosis or treatment plan was incomplete. Not every guard is appropriate for every jaw problem, and no appliance can single-handedly correct airway strain, daytime clenching, or dysfunctional oral posture.
If you're tired of chasing jaw pain, headaches, and poor sleep as if they're unrelated problems, Pain and Sleep Therapy Center offers a root-cause approach focused on non-surgical relief. Their team evaluates how your jaw, breathing, sleep, and muscle function interact, then builds a personalized plan that may include conservative care, regenerative treatment, and functional therapy to help you heal more completely.



