
You wake up with a tight jaw, a temple headache, and a sore spot at the base of your skull. By afternoon, your shoulder feels hard as stone. You try stretching. You rub the painful area. Maybe you even get a massage that helps for a day, then everything returns.
That pattern is common in people with trigger points. The pain feels local, but the underlying driver may be somewhere else. That's one reason jaw pain, TMJ symptoms, headaches, and neck tension can linger for months without a clear explanation.
When patients finally understand trigger point therapy, many feel relief before treatment even starts. Not because the problem is gone, but because the pattern starts to make sense. The jaw can trigger the temple. The neck can trigger the face. Sleep posture can keep the whole cycle going. Once you identify the right tissue, treatment becomes much more precise.
Why Your Muscle Pain Might Not Be What It Seems
A lot of muscle pain gets treated at the place it hurts. That sounds reasonable, but it often misses the source.
If you feel pain in the temple, many people focus only on the head. If your jaw clicks, attention goes straight to the joint. If your neck burns by late afternoon, treatment may stay centered on the neck itself. Sometimes that's appropriate. Often, it isn't.
A trigger point can act like a faulty light switch in a wiring system. The switch is in one room, but the problem shows up somewhere else. In muscle pain, that means a tight, irritable spot in one muscle can send pain into a different region entirely.
Why this gets missed
A widely cited discussion of myofascial care notes that active myofascial trigger points are estimated at 46.1% in the general population, yet clinicians often treat the pain site rather than the actual trigger point causing it (myofascial trigger point prevalence and diagnostic gap). That helps explain why so many people feel stuck between temporary relief and recurring symptoms.
Clinical reality: If treatment keeps chasing the place you feel pain, but never checks the muscles that refer pain into that area, progress is often short-lived.
This matters even more in the head, face, and jaw. Orofacial pain is crowded. Teeth, joints, nerves, airway issues, posture, clenching, and neck muscles can all overlap. A trigger point in a chewing muscle can feel like tooth pain. A neck trigger point can mimic a headache disorder. A strained jaw muscle can make TMJ symptoms look worse than the joint itself.
What usually works better
A better exam asks different questions:
- Where does pressure reproduce your familiar pain rather than only where are you tender
- Which muscles feel ropey or restricted during movement and palpation
- What habits keep the tissue irritated such as clenching, mouth breathing, poor desk setup, or sleep position
That root-cause approach doesn't make trigger point therapy a magic fix. It makes treatment more honest and more targeted.
What Exactly Is a Trigger Point
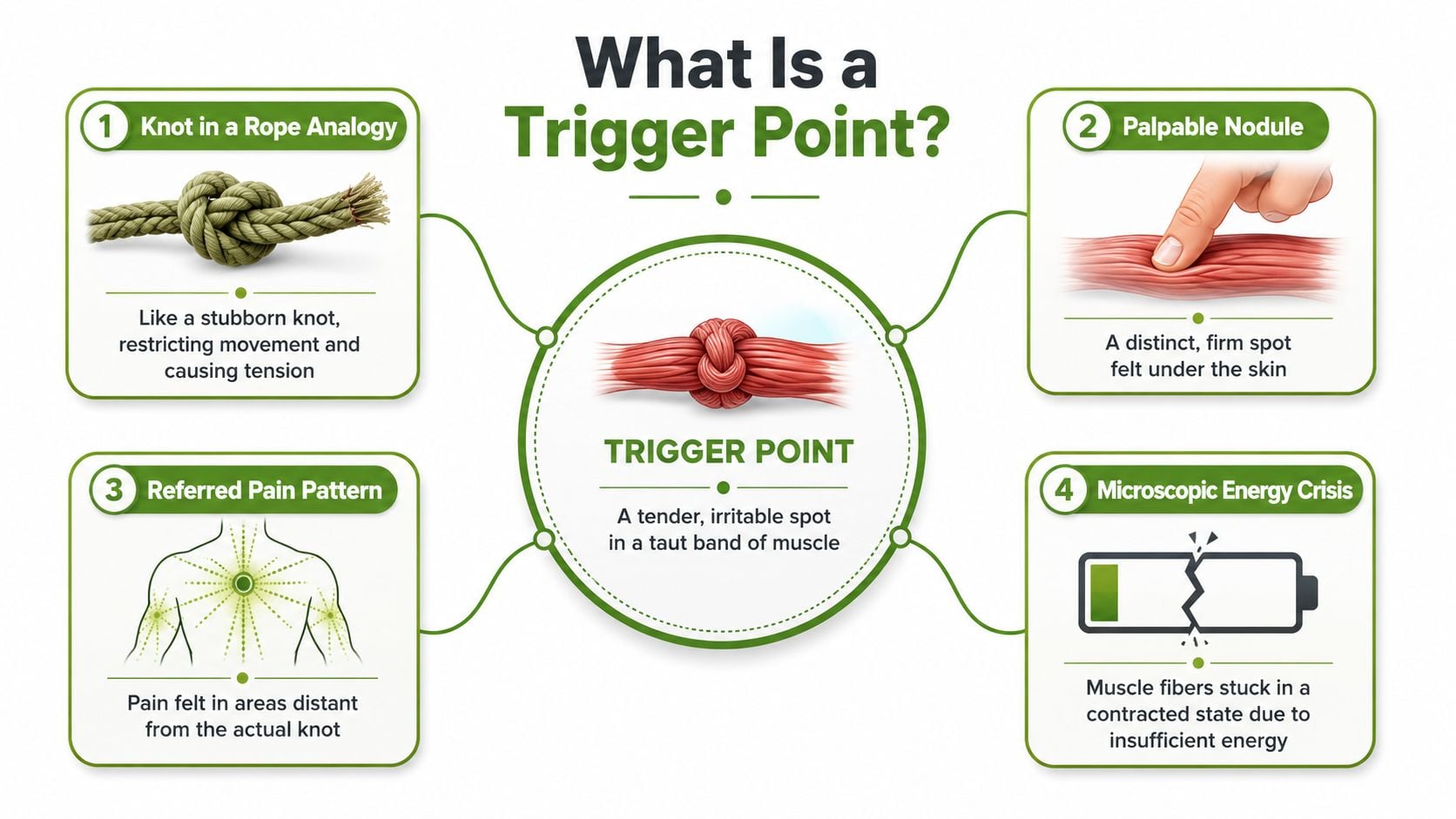
A trigger point is a tender, irritable spot inside a tight band of muscle. Clinicians often feel it as a small nodule or thickened section within a taut muscle strand.
A simple way to picture it is a knot in a rope. One short segment bunches up, and now the whole rope doesn't glide well. The tissue around it has to compensate. Movement becomes less efficient, pressure hurts, and pain may spread beyond the knot itself.
Active and latent trigger points
Not all trigger points behave the same way.
An active trigger point hurts in a recognizable way, sometimes even when nobody is pressing on it. This is the kind that can feed ongoing jaw pain, a temple headache, or a pulling ache under the shoulder blade.
A latent trigger point is quieter. You may not notice it during normal activity, but it becomes painful when pressed. These often matter because they still restrict movement and can become active when stress, overuse, poor sleep, or clenching increase the load on the system.
Pain patterns are more predictable than most people think
Trigger points aren't random sore spots. A statistical analysis of pain patterns in Myofascial Pain and Dysfunction: The Trigger Point Manual found highly consistent anatomical distributions, with Muscle Belly Pain in 85.4%, Origin-Insertion Pain in 80.9%, and Referred Pain in 59.5% (predictable trigger point pain patterns).
That finding matters in practice. It means a trained clinician isn't just poking around hoping to get lucky. They are using known muscle referral behavior, symptom reproduction, range-of-motion findings, and tissue feel to identify likely pain generators.
Pressing the right spot should feel familiar, not just tender. Patients often say, "That's it. That's my headache," or "That shoots into my jaw."
What patients usually notice
People with trigger points often report a mix of symptoms rather than one clean complaint:
- Local tenderness that feels sharp, achy, or bruised
- Pain with movement such as chewing, turning the head, or opening the mouth
- Referral into the temple, ear, teeth, face, or back of the head
- Tightness without obvious injury that keeps returning after self-massage or stretching
This is why trigger point therapy can be so useful. It gives a practical explanation for pain that doesn't behave the way people expect.
How These Painful Knots Form and Persist
Some trigger points begin after overuse, clenching, poor posture, awkward sleep, stress, or an injury that never fully settled down. Others build slowly when a muscle stays overloaded for too long.
The deeper problem isn't just "tightness." It's a local breakdown in muscle function.

The energy crisis inside the muscle
A trigger point is best understood as a localized energy crisis. According to an osteopathic review, trigger points involve ischemia and a perpetual contraction knot, with neurotransmitters and cytokines sensitizing pain receptors and sustaining a vicious cycle (trigger point pathophysiology and energy crisis).
In plain language, a small portion of muscle gets stuck in a contracted state. That contracted tissue compresses its own local circulation. Less blood flow means less oxygen delivery and poorer waste removal. The tissue becomes chemically irritated. Nearby nerves become more sensitive. The muscle tightens more. The cycle feeds itself.
Why stretching alone often doesn't hold
A tight muscle with no trigger point may respond well to routine stretching. A trigger point is different. If the tissue is locked in this low-oxygen, irritated state, stretching can feel good briefly but fail to change the underlying loop.
That's why people often say things like:
- "I stretch every day, but the same spot comes back."
- "Massage helps for a few hours."
- "My jaw loosens, then tightens again by evening."
Those aren't signs that you're doing something wrong. They usually mean the trigger point hasn't been adequately deactivated, or the perpetuating factor is still there.
A short visual overview can help make that mechanism easier to grasp:
Why some trigger points become stubborn
Chronic trigger points rarely persist for one reason alone. More often, several inputs keep re-irritating the tissue:
- Jaw clenching or grinding during stress or sleep
- Head-forward posture at a laptop or phone
- Shallow breathing patterns that overwork neck muscles
- Poor sleep position that loads the jaw, neck, or shoulder for hours at a time
Important distinction: A trigger point can be the pain generator, but it can also be the messenger. If you deactivate it without changing the reason it formed, symptoms often return.
This is why effective trigger point therapy isn't just hands-on treatment. It also includes identifying what keeps the muscle from calming down.
How Professionals Deactivate Trigger Points
Professional care ranges from hands-on pressure work to needling and injection-based treatments. The right choice depends on the tissue involved, the patient's tolerance, the duration of symptoms, and whether the problem is mostly muscular or tied to a joint, ligament, or airway-related habit.
Manual treatment first
The least invasive option is usually manual trigger point therapy. That can include ischemic compression, sustained pressure, cross-fiber work, and myofascial release.
When done well, manual work isn't a contest to see how much pain you can tolerate. Good treatment uses enough pressure to engage the tissue, but not so much that the muscle guards harder. In the jaw, temple, neck, and upper trapezius, precision matters more than brute force.
Manual care tends to work best when:
- the trigger point is superficial and easy to access
- the patient is very sensitive to needles
- symptoms are newer or more reactive than entrenched
Dry needling and why it helps some patients more
Dry needling places a thin needle directly into the trigger point. The goal is not to inject medication. The goal is to mechanically and neurologically disrupt the dysfunctional spot.
Systematic reviews covering 19 studies found that trigger point dry needling was more effective than stretching and at least as effective as manual therapy for myofascial pain, with meaningful short-term pain reduction and functional improvement, even though it mainly deactivates trigger points rather than permanently eliminating them (systematic review summary on dry needling for myofascial pain).
A local twitch response often tells the clinician they've hit the right area. Patients describe it as a brief jump or snap in the muscle. After that response, the tissue may soften, pressure pain may drop, and movement may become easier.
Dry needling can be very effective, but it isn't automatically the best first step for every patient. A guarded jaw, a highly sensitized nervous system, or fear of needles may call for a gentler starting point.
When injections or regenerative approaches enter the picture
Some cases don't stay in the simple "muscle knot" category. Chronic pain around the jaw and head often overlaps with tendon irritation, ligament laxity, joint overload, or tissue that hasn't healed well after months or years of strain.
That is where trigger point injections, Prolotherapy, or Platelet-Rich Fibrin (PRF) may become part of a broader plan. If you want a patient-friendly primer before discussing that option with a clinician, this guide to understanding trigger point injections is a useful overview.
Regenerative medicine approaches aim to do more than quiet a painful spot. In the right setting, they may support healing in tissues that keep re-triggering muscular pain. That's especially relevant when a trigger point is downstream from a stressed attachment point or an unstable local structure.
Some practices also combine soft tissue work with modalities such as cold laser therapy for pain relief, which may fit patients who want a noninvasive option alongside hands-on care.
Comparing treatment options
| Therapy | Mechanism | Best For |
|---|---|---|
| Manual therapy | Sustained pressure and soft tissue release to reduce irritability and improve tissue glide | Superficial trigger points, sensitive patients, first-line care |
| Dry needling | Needle stimulation of the trigger point to provoke a twitch response and reset the muscle | Stubborn myofascial pain, deeper trigger points, limited response to stretching |
| Trigger point injections | Precise injection into painful tissue to reduce local pain and improve function | Focal pain that hasn't responded to conservative care |
| Prolotherapy or PRF | Regenerative injection approach aimed at supporting tissue healing and reducing recurrent irritation | Cases with chronic overload, attachment pain, or structural contribution |
The trade-off is straightforward. Less invasive options are easier to start but may need repetition. More advanced options can be helpful in the right hands, but they require sharper diagnosis and should be used for the right tissue target.
The Link Between Trigger Points, TMJ, Headaches, and Sleep
Jaw pain rarely lives in the jaw alone. Patients with TMJ symptoms often also deal with temple pressure, facial aching, ear symptoms, neck tightness, and morning headaches. Trigger points are one reason these complaints cluster together.
A jaw muscle doesn't need to be visibly swollen to create major symptoms. It only needs to be overloaded, irritable, and connected to the pain pattern you're feeling.
The jaw and head referral map
Several muscles matter more than most patients realize.
The masseter can refer pain into the jaw, cheek, and teeth. The temporalis can create temple pain and head pressure that feels very much like a tension headache. The sternocleidomastoid and upper trapezius can send discomfort into the side of the head, behind the eye, or toward the base of the skull.
That overlap is one reason many people spend months trying to sort out whether they have a dental problem, a sinus issue, a neck problem, migraines, or TMJ. Sometimes the answer includes more than one of those. Sometimes the muscle is the main driver.
If you want a broader overview of jaw-related symptoms and mechanics, this page on TMJ disorder lays out the condition clearly.
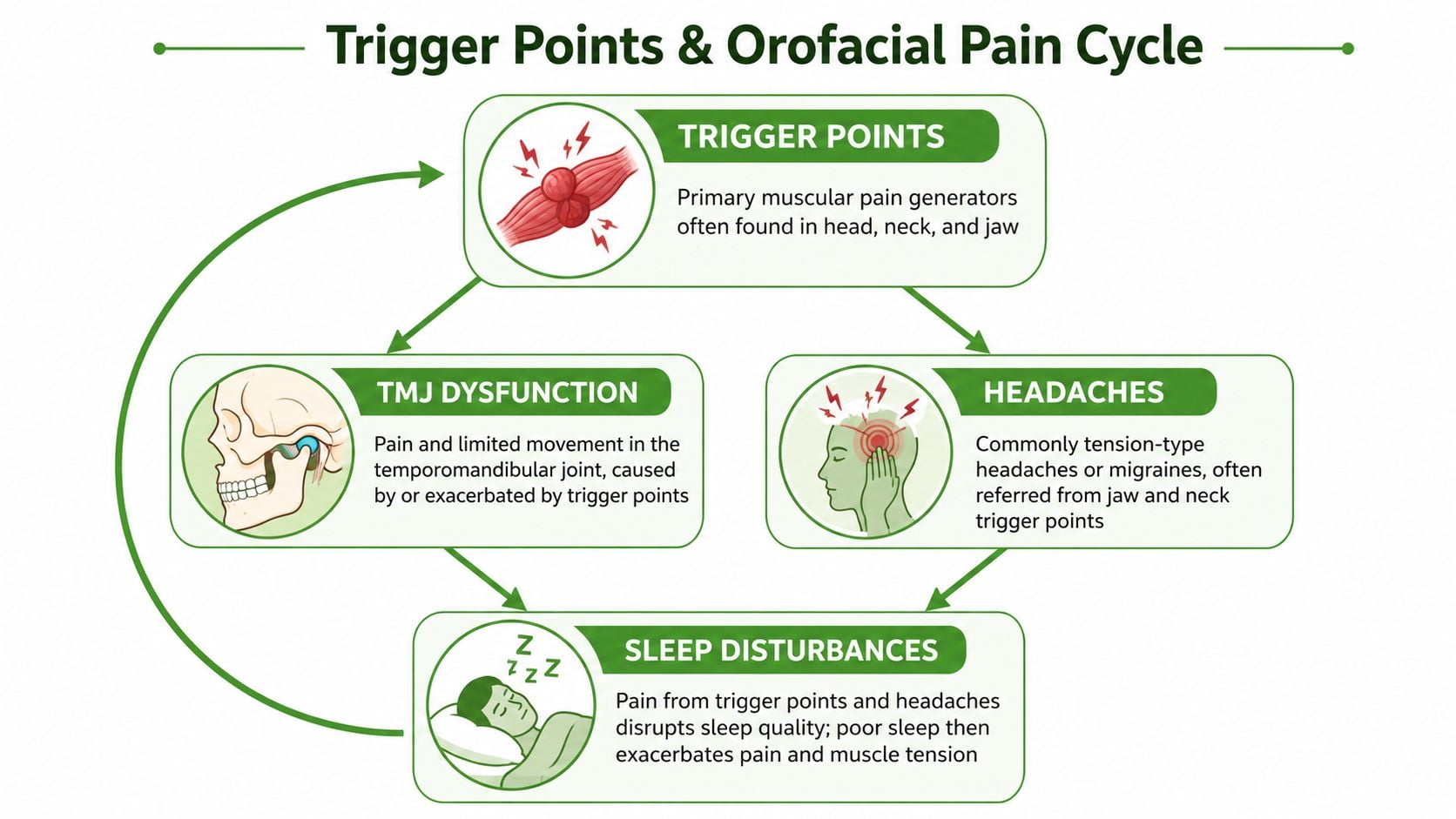
Why sleep can make it worse
Nighttime is often when the system gets reloaded.
If you clench, grind, sleep with your head twisted, or breathe poorly during sleep, the same muscles may stay active for hours. That can leave you waking with locked jaw muscles, neck stiffness, or a headache that seems to arrive before your day even starts.
Poor sleep also lowers your tolerance for pain. So even when the trigger point itself hasn't changed much, your nervous system may react more strongly after a rough night.
The airway connection clinicians shouldn't ignore
This is the part many general articles miss. Muscle tension around the jaw, tongue, face, and neck can interact with sleep-related airway problems.
When oral posture is poor, nasal breathing is limited, or the jaw and neck muscles are chronically braced, patients may snore more, wake unrefreshed, or maintain positions that keep overloading the same tissues. The result is a loop. Poor sleep aggravates muscular pain. Muscular pain disturbs sleep. Airway strain can intensify both.
For patients trying to reduce sleep-related strain on the neck and back, practical bedroom setup advice can help. This article on Lucas Furniture advice for back pain offers useful guidance on sleep positioning and support surfaces.
If your headaches are worst in the morning, your jaw feels fatigued on waking, and your sleep isn't restorative, don't treat those as separate problems until someone has evaluated how they connect.
A focus on root causes is important. In the right patient, treating the trigger points helps. So does reducing the reason those muscles are overworking in the first place.
Self-Care Techniques for Managing Trigger Points at Home
Home care can calm trigger points, especially when you use the right amount of pressure and stop trying to crush the spot into submission. The goal is to reduce irritability, improve blood flow, and help the muscle let go without provoking a flare.
Use pressure, but keep it measured
A lacrosse ball, tennis ball, foam roller, or Thera Cane can all work. The best tool depends on the body region.
For the upper trapezius or the muscles along the shoulder blade, a lacrosse ball against the wall gives good control. For the jaw and temple, fingers usually work better because the area is smaller and more sensitive.
Try this sequence:
- Find the familiar spot. Look for a tender band or knot that reproduces your usual pain pattern.
- Apply steady pressure. Hold gentle to moderate pressure. Sharp pain means back off.
- Breathe slowly. Exhale and let the area soften rather than bracing against the sensation.
- Release and retest. Check whether head turn, jaw opening, or shoulder motion feels easier.
Two rounds are often enough. More isn't always better.
Good habits matter more than heroic effort
A trigger point often reflects what your body repeats all day and all night. That's why small habits often outperform occasional intense self-treatment.
- Desk posture matters. Bring the screen up, support the forearms, and stop craning toward the laptop.
- Driving posture matters too. If your seat pushes your head forward, your neck muscles never really rest.
- Hydration and regular movement help irritable muscles recover better than hours of stillness.
- Jaw rest position is useful. Lips together, teeth apart, tongue resting comfortably up, unless a clinician has told you otherwise.
If jaw muscles are a major part of your symptoms, these practical steps for how to massage your jaw can help you work more safely at home.
Fix the overnight aggravators
If you do great self-care all day and then sleep in a position that reloads the same tissue for hours, progress slows down. Pillow height, neck rotation, and stomach sleeping can all matter.
For a broader look at nighttime mechanics, these insights on sleeping posture and spinal health are worth reviewing.
At-home rule: Aim for a "good pain" that feels productive and eases after pressure. If the area throbs, bruises, or feels angrier for the rest of the day, the dose was too much.
What not to do
Some self-care approaches backfire:
- Don't jab aggressively into the jaw, temple, or front of the neck
- Don't stretch hard immediately after heavy pressure on an irritated spot
- Don't keep treating the same point repeatedly if it never changes
- Don't ignore clenching, posture, or sleep position while expecting lasting relief
Home care works best as support, not as a substitute for a proper diagnosis when symptoms are persistent or complicated.
When Self-Care Is Not Enough and You Need an Expert
Self-treatment is reasonable for mild, straightforward muscle pain. It isn't enough when the pattern is persistent, spreading, or mixed with other symptoms.
Seek urgent medical attention if pain is sudden and severe, follows major trauma, comes with numbness or weakness, includes loss of muscle control, or is accompanied by symptoms that suggest something more serious than a muscular problem. Trigger points can cause impressive pain, but they shouldn't be used to explain away every symptom.
Signs it's time for a specialist evaluation
A professional assessment makes sense when any of these apply:
- Pain keeps returning despite stretching, massage, or home release work
- Jaw symptoms are escalating, such as locking, catching, or limited opening
- Headaches are frequent or persistent, especially if they seem tied to chewing, neck movement, or waking
- Sleep is affected, including snoring, poor rest, morning jaw fatigue, or waking with facial tension
- Function is dropping, whether that's eating, talking, exercising, concentrating, or working comfortably
What a good evaluation should include
A useful exam usually looks beyond the sore spot itself. It should consider muscle referral patterns, jaw mechanics, cervical involvement, parafunctional habits like clenching, breathing pattern, and what happens during sleep.
That kind of assessment changes treatment. Sometimes the answer is direct trigger point therapy. Sometimes it's a mixed plan that includes manual work, dry needling, exercise, jaw rehabilitation, airway-focused treatment, or regenerative options for irritated supporting tissue.
The main point is simple. If symptoms are chronic, complex, or keep circling back, guessing costs time. A careful diagnosis gives you a real chance at lasting relief.
If you're dealing with TMJ pain, headaches, facial tension, or sleep-related symptoms that don't seem to fit into one simple category, Pain and Sleep Therapy Center offers root-cause evaluation focused on the connection between jaw function, muscle pain, and airway health. Their team provides personalized care for patients who want more than temporary symptom control.



