
Some nights, the worry starts before your child even falls asleep. You hear the pacing, the repeated calls from the bedroom, the coughing, the restless tossing, or the long pause that makes you lean in closer just to hear breathing. Other nights, the problem shows up the next day. A child who wakes unrefreshed, melts down easily, struggles to focus, or seems wired and tired at the same time.
Parents often blame themselves first. Maybe the bedtime routine isn't right. Maybe naps went off track. Maybe this is just a phase. Sometimes it is a phase. But persistent sleep trouble deserves a closer look, especially when it keeps affecting mood, learning, behavior, growth, or family life.
When Your Child's Sleep Becomes a Worry
A pattern I see often is a parent who's been told, gently or not so gently, to wait it out. They've tried blackout curtains, earlier bedtimes, later bedtimes, white noise, fewer snacks, more snacks, and every version of “good sleep hygiene” they can find. What they need most is reassurance that pediatric sleep disorders are real medical issues, not evidence of bad parenting.
That matters because these conditions are common and often missed in everyday care. In a large U.S. primary-care sample, only 3.7% of children received a formal sleep-disorder diagnosis, even though population estimates for problems such as behavioral insomnia and primary snoring were much higher in the same paper (evidence on underdiagnosis in pediatric sleep care). Parents should take that gap seriously. If your instincts tell you something isn't right, it's reasonable to keep asking questions.
For babies and toddlers, confusion is especially common because development changes sleep so quickly. A child can be learning new skills, feeding differently, teething, and changing nap patterns all at once. Resources like this baby milestones and development guide can help parents understand what's age-expected and what may be worth discussing with a clinician.
Practical rule: A phase usually improves. A disorder tends to repeat, persist, or create daytime fallout.
The most useful shift is from self-blame to observation. Don't ask, “What am I doing wrong?” Ask, “What pattern keeps happening, and what might be driving it?” That question opens the door to real answers.
Understanding the Spectrum of Sleep Disorders
Parents usually come in with one complaint. “My child won't fall asleep.” “She snores.” “He sleepwalks.” “She's exhausted all day.” Those are starting points, not final diagnoses. Pediatric sleep disorders cover a wide range of problems, and it helps to sort them into a few broad groups.
Sleep issues are not rare. Reviews of pediatric sleep health report that bedtime problems affect 10%–30% of young children, pediatric OSA affects 1%–5%, and delayed sleep phase syndrome affects 7%–16% of adolescents (population patterns across common pediatric sleep problems). That range is one reason broad thinking matters.
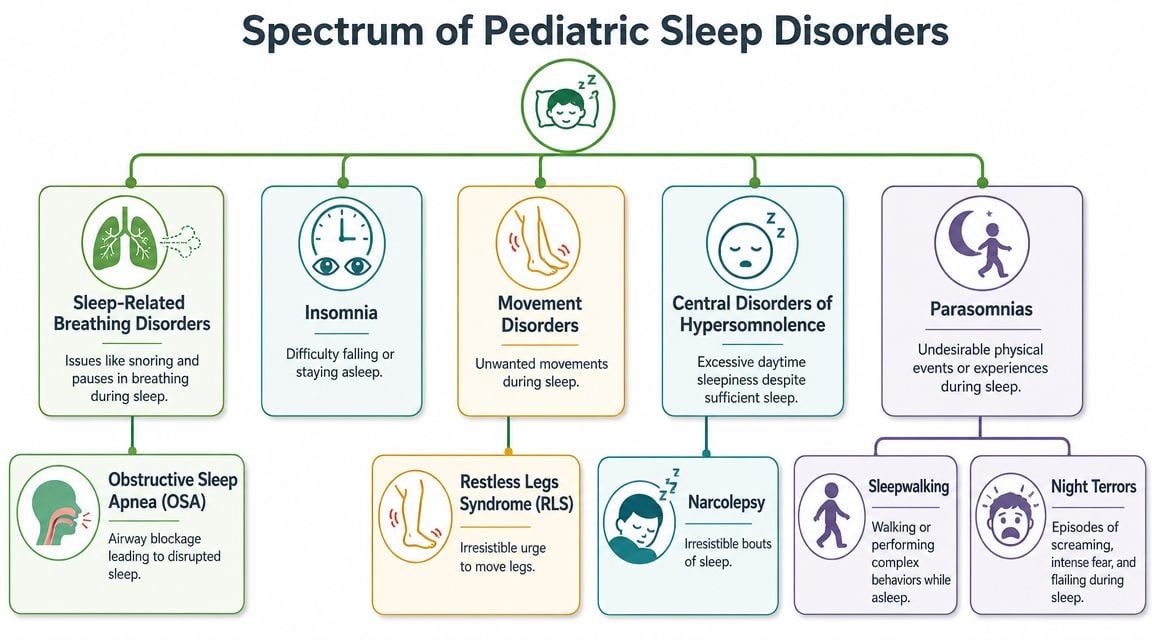
The four big buckets parents should know
Behavioral insomnia is the “won't sleep” category. A child may resist bedtime, need very specific conditions to fall asleep, or wake repeatedly and need help returning to sleep. Sometimes the issue is routine and sleep associations. Sometimes routine is only part of the picture, and discomfort, breathing issues, anxiety, or sensory dysregulation keep the pattern going.
Parasomnias are the “strange things during sleep” category. This includes sleepwalking, confusional arousals, and night terrors. These events can be dramatic and frightening to watch, but they don't always mean a dangerous disorder. What matters is timing, frequency, safety risk, and whether poor sleep quality is making them more likely.
Sleep-related breathing disorders are the “can't breathe well during sleep” group. Parents often picture only loud snoring, but breathing problems can also show up as mouth breathing, restless sleep, sweating, unusual sleep positions, teeth grinding, repeated awakenings, or daytime irritability. Obstructive sleep apnea works a lot like a kink in an air hose. Air is trying to move, but the passage narrows or collapses enough to disturb sleep and strain the body.
Central disorders of hypersomnolence are the “too sleepy despite enough time in bed” problems. These are less common in everyday parenting discussions, but they matter. If a child or teen seems persistently sleepy, struggles to stay awake in passive settings, or never seems restored by sleep, it deserves evaluation rather than being dismissed as laziness.
Why labels matter less than patterns at first
Parents don't need to diagnose the exact category at home. They do need to notice which pattern sounds familiar.
- Bedtime battle pattern: The child resists sleep, delays sleep, or depends on a parent to return to sleep.
- Breathing pattern: Snoring, open-mouth sleep, gasping, unusual sleeping positions, or restless nights.
- Event pattern: Sleepwalking, screaming episodes, or behaviors that occur while not fully awake.
- Daytime sleepiness pattern: Morning difficulty, dozing, poor attention, or an “always tired” teen.
If you're sorting through whether your child's wake-ups are a regression, a developmental phase, or part of something broader, this guide on tackling sleep challenges can be a helpful companion for framing the question.
Not every child with a sleep disorder looks sleepy. Some look hyperactive, impulsive, emotional, or impossible to settle.
That's one reason pediatric sleep disorders get mislabeled. The nighttime clue and the daytime clue don't always look like they belong to the same problem.
Age-Specific Symptoms and Red Flags to Watch For
The same sleep disorder can look very different at different ages. Infants may show feeding and settling trouble. School-aged children may show behavior changes. Teenagers may look unmotivated when they are sleep deprived or sleeping at the wrong biological time.
Red flags by developmental stage
| Age Group | Common Red Flags |
|---|---|
| Infants | Frequent difficulty settling, very noisy breathing during sleep, persistent mouth breathing, arching or seeming uncomfortable when laid down, very fragmented sleep that doesn't improve, feeding struggles tied to poor oral coordination, and a parent sense that sleep never looks peaceful |
| Toddlers | Strong bedtime resistance, repeated night waking, snoring, sweating during sleep, unusual sleeping positions, night terrors, frequent movement, needing a parent present every time they wake, and daytime irritability that seems out of proportion |
| School-aged children | Snoring, open-mouth posture, restless sleep, bedwetting that seems tied to poor sleep quality, morning headaches, hard-to-wake mornings, falling asleep in the car, attention problems, hyperactivity, emotional volatility, and teachers reporting focus issues |
| Teenagers | Very late sleep onset, major trouble waking for school, sleeping in excessively when allowed, daytime sleepiness, napping that shifts the schedule further, academic drop-off, irritability, depressed mood, and “insomnia” that is actually a delayed body clock |
What deserves earlier evaluation
Some signs should move parents from watchful waiting to active follow-up.
- Breathing concerns: Loud snoring, pauses, gasping, persistent mouth breathing, or labored breathing during sleep.
- Daytime impairment: School problems, behavior shifts, persistent fatigue, headaches, or frequent morning battles that feel disproportionate.
- Nighttime events: Sleepwalking or night terrors that happen often, cause injury risk, or worsen over time.
- Growth and feeding concerns: Especially in infants and younger children when oral function and breathing mechanics may overlap.
A useful rule is to think in clusters rather than single symptoms. A child who snores once during a cold is different from a child who snores, sleeps restlessly, mouth breathes, and struggles in the morning.
The symptom parents often miss
Hyperactivity can be a sleep symptom. So can clumsiness, poor frustration tolerance, and “second wind” energy late at night. Many children don't respond to fatigue by slowing down. They speed up.
If your child seems overtired but won't settle, don't assume that means they aren't tired. In pediatrics, exhaustion often shows up as dysregulation.
Parents know their child's baseline. If sleep has started changing behavior, mood, learning, or family functioning, that observation is clinically useful. Write it down. It helps more than trying to remember details in a rushed appointment.
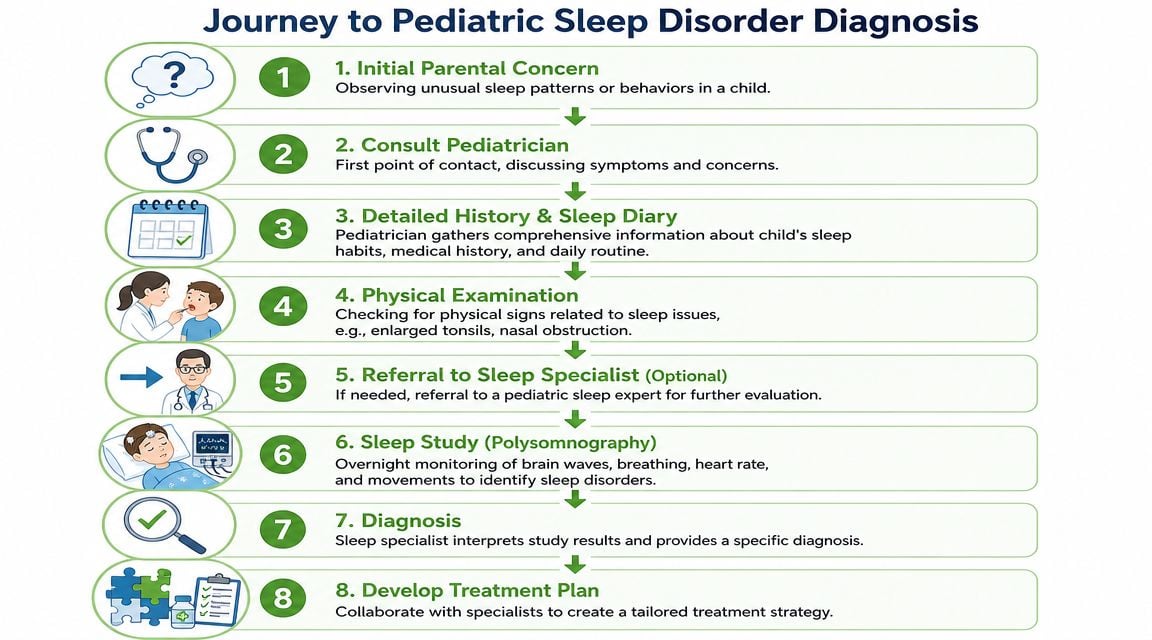
The Path to a Clear Diagnosis
A good diagnosis rarely starts with a test. It starts with a history. The fastest way to get useful answers is to show a clinician what's happening over time, not just what happened on the worst night.
What to bring to the first visit
Before the appointment, it helps to gather a short record.
- Sleep timing: Bedtime, sleep onset, wake times, naps, and how long night wakings last.
- Breathing observations: Snoring, mouth breathing, pauses, sweating, or odd sleep positions.
- Daytime effects: Mood, focus, headaches, morning behavior, and school concerns.
- Short videos if safe to capture: A brief clip of breathing or movement during sleep can be very useful.
Sometimes clinicians begin with screening questions and an exam. Sometimes they recommend a home-based step first. If you're trying to understand what that process can look like, this overview of how to diagnose sleep apnea at home gives a practical sense of where home testing may fit.
What a sleep study actually tells you
Later in the workup, some children need polysomnography, which is an overnight sleep study. It records multiple body signals during sleep so the team can evaluate breathing, arousals, movement, and overall sleep architecture. This can sound intimidating to families, but the purpose is straightforward. It replaces guessing with measurement.
For pediatric polysomnography, sleep efficiency of 85% or higher is considered normal, and sleep latency of 10 to 30 minutes is typical (plain-language pediatric polysomnogram reference values). Those numbers don't diagnose a child in isolation, but they help clinicians interpret whether the night looked efficient or disrupted.
A short video can make the process feel more concrete for parents considering next steps.
Why one specialist is not always enough
Many children need more than a single-lens evaluation. A pediatrician may identify the concern. A sleep specialist may guide testing. An ENT may assess tonsils, adenoids, and nasal obstruction. A dentist or orthodontic provider may look at jaw development and oral space. A myofunctional therapist may evaluate tongue posture, lip seal, swallowing patterns, and breathing habits.
That doesn't mean every child needs a large team. It means the right diagnosis often comes from asking whether the problem is behavioral, structural, functional, neurologic, or a mix of several.
Why Looking Beyond Tonsils Is Crucial
For years, many families heard a simplified message. Child snores, check tonsils. If tonsils are large, remove them. If they're not, move on. That approach helps some children, but it misses many others.

Airway problems are rarely one-dimensional
Large tonsils and adenoids can absolutely contribute to sleep-disordered breathing. But they're not the whole story. A Cleveland Clinic expert discussion notes that a broader view is needed, including obesity, craniofacial anatomy, and comorbid conditions. The same source states that up to 80% of children with Down syndrome have sleep apnea, and it also notes rising pediatric burden alongside obesity trends (broader contributors to pediatric obstructive sleep apnea).
That broader view changes the questions clinicians ask. Is the child a chronic mouth breather? Is the palate narrow? Does the jaw sit back? Is lip seal weak? Does the tongue rest low in the mouth? Are there swallowing patterns, oral restrictions, or breathing habits that affect facial growth over time?
Structure and function shape each other
A child's airway is not just a static tube. It's part of a living system that includes nasal breathing, tongue posture, jaw development, muscle tone, and sleep position. If nasal breathing is difficult for a long time, children often compensate with open-mouth posture. That can affect oral function. Over time, oral function can also influence growth patterns.
This is why a narrow “snoring equals big tonsils” model falls short. Even when surgery is appropriate, it may not fully address how the child breathes, rests the tongue, swallows, or stabilizes the airway during sleep.
A treatment can remove one obstruction and still leave the child with poor breathing mechanics.
That's the gap many parents sense when symptoms improve only partly, or return later.
What a root-cause evaluation looks like
A more modern workup asks whether the child has:
- Anatomical contributors: Tonsils, adenoids, nasal blockage, palate shape, jaw position, or facial growth concerns
- Functional contributors: Mouth breathing, low tongue posture, poor lip seal, inefficient swallowing, or dysfunctional breathing patterns
- Medical contributors: Allergies, weight-related factors, neurologic or genetic conditions
- Behavioral contributors: Irregular schedules, learned sleep associations, or anxiety around sleep
Parents exploring this side of care often find it useful to learn how myofunctional therapy for sleep apnea fits into a broader airway plan. The value isn't in chasing a trendy therapy. It's in understanding that airway stability depends on both form and function.
Evidence-Based Treatments for Restful Nights
Treatment works best when it matches the driver of the problem. A child with bedtime resistance needs a different plan from a child with airway obstruction. A child with night terrors needs a different approach from a teen whose body clock has shifted late. The mistake is trying one generic fix for every sleep complaint.
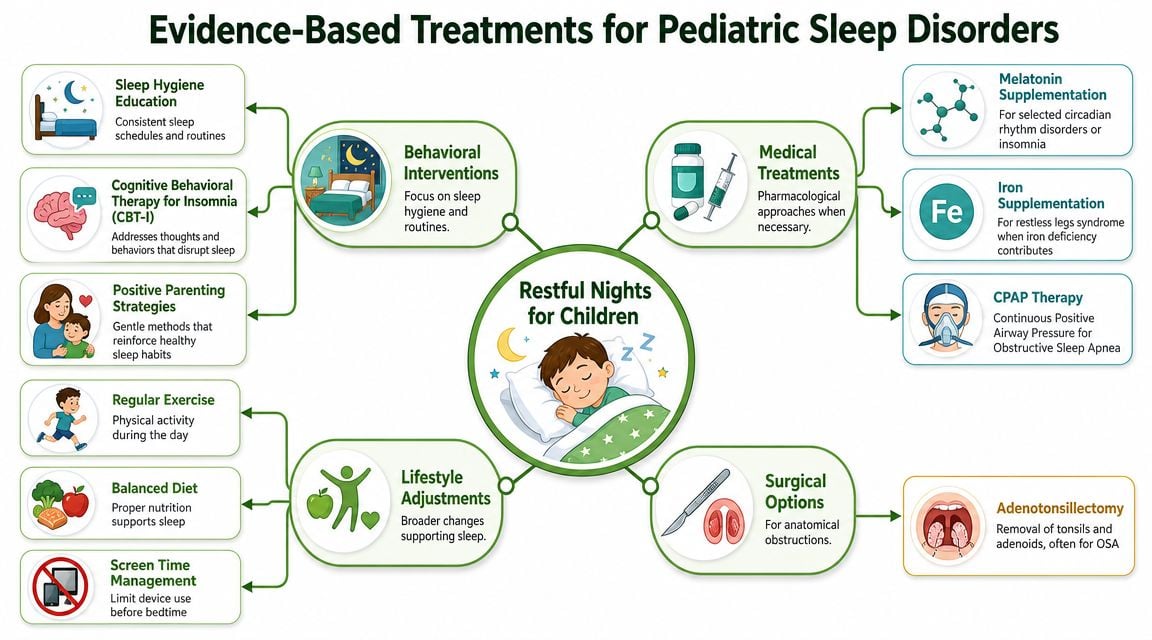
What often works first
For many families, the foundation is behavioral and environmental.
- Consistent timing: A regular wake time is often more powerful than endlessly adjusting bedtime.
- A predictable wind-down: Children settle better when the sequence is stable and boring in the best possible way.
- Screen management: Bright, stimulating media close to bedtime commonly makes sleep onset harder.
- A sleep-friendly room: Dark, quiet, and cool is the goal, but families should adapt this realistically, not perfectly.
These measures matter, but they are not cure-alls. Good routines won't fix untreated sleep apnea, restless movement, or chronic mouth breathing.
Medical and device-based options
Some children need medical treatment targeted to the diagnosis. That may include support for allergies or congestion, treatment for underlying contributors identified by the child's clinician, or positive airway pressure for significant obstructive sleep apnea. In selected cases, surgery such as adenotonsillectomy is appropriate when anatomy is a major part of the problem.
Families considering a broader range of options can review pediatric sleep apnea treatment to understand how treatment plans may combine medical, behavioral, and airway-focused care.
Clinical reality: The “best” treatment is not the most aggressive one. It's the one that matches the child's actual mechanism of sleep disruption.
Where functional therapies fit
A lot of mainstream articles stop too early. They mention surgery, maybe CPAP, maybe sleep hygiene, and leave out the functional piece.
Orofacial myofunctional therapy focuses on how the tongue, lips, cheeks, and jaw work together. In children with open-mouth posture, low tongue posture, poor lip seal, or inefficient swallowing, retraining oral function may support healthier breathing patterns and better airway stability. It does not replace medical evaluation. It complements it when function is part of the problem.
Breathing retraining helps children who habitually overbreathe, mouth breathe, or use poor mechanics during rest and sleep transitions. The aim is not perfection. The aim is easier nasal breathing, calmer physiology, and more efficient patterns.
Frenectomy, when indicated after careful evaluation, may be part of treatment in children whose tongue mobility is restricted in a way that affects feeding, oral function, posture, or airway-related patterns. It is not a stand-alone answer. Without preparation and follow-up therapy, the child may keep the same dysfunctional habits.
Trade-offs parents should understand
Different treatments solve different parts of the problem.
| Approach | Best for | What it may not fix by itself |
|---|---|---|
| Behavioral sleep work | Bedtime resistance, sleep associations, schedule drift | Structural airway obstruction |
| ENT or surgical care | Enlarged tonsils/adenoids, some anatomical blockages | Low tongue posture, mouth-breathing habits, sleep anxiety |
| CPAP or other airway support | Ongoing obstructive sleep apnea when indicated | Daytime habits, oral dysfunction, adherence challenges |
| Myofunctional and breathing therapy | Oral posture, breathing mechanics, functional contributors | Conditions that need medical or surgical treatment first |
The strongest treatment plans are often layered. A child may need better routines, allergy management, airway evaluation, and functional retraining. That's not overcomplicating care. That's matching care to reality.
Your Action Plan for Helping Your Child Sleep Better
Parents do best when they have a simple next step. For pediatric sleep disorders, I'd narrow that to three.
Observe with purpose
Keep a brief log for one to two weeks. Note bedtime, how long sleep seems to take, wake-ups, breathing signs, sleep position, and next-day behavior. Short phone videos of snoring, mouth breathing, or restless movement can help if they're captured safely.
Discuss the full picture
Bring both nighttime and daytime symptoms to your child's clinician. Don't lead only with “won't sleep.” Mention snoring, mouth breathing, headaches, hyperactivity, hard mornings, feeding issues, school concerns, or repeated parasomnias. Patterns across systems often point to the cause.
Seek care that matches the cause
If the issue looks like breathing, anatomy, oral function, or a mix, ask whether your child needs a broader airway-focused evaluation rather than a single-discipline opinion. Keep in mind that sleep health is also shaped by context. An NIH review emphasizes that neighborhood conditions such as noise, air quality, and safety can affect pediatric sleep, so effective treatment sometimes means addressing environmental barriers along with medical ones (NIH review on social and environmental drivers of pediatric sleep health).
For home habits, families often benefit from practical, non-alarmist resources with valuable insights for better sleep. Use those ideas as support, not as a reason to delay care when red flags are present.
You are not overreacting by paying attention to your child's sleep. You're noticing a health signal. That's exactly what good parents do.
If your child snores, mouth breathes, sleeps restlessly, or struggles with sleep in ways that don't fit a simple routine problem, Pain and Sleep Therapy Center offers root-cause, interdisciplinary evaluation for pediatric airway and sleep-related concerns. Their team looks beyond surface symptoms to assess breathing, oral function, jaw development, and sleep-disordered breathing patterns so families can pursue a treatment plan that fits the child, not just the diagnosis.



