
A facial injury changes the day instantly. One moment you're dealing with a fall, collision, sports injury, or assault. The next, you're trying to make sense of swelling, bleeding, jaw pain, numbness, a bite that feels wrong, and the fear that your face may never look or function the same.
That fear is understandable. Facial trauma sits at the intersection of appearance, breathing, vision, speech, eating, and pain. Patients often want one simple answer, usually, “Will I need surgery?” The honest answer is that some injuries do, some don't, and even when surgery is necessary, the operation is only one part of recovery.
Facial trauma surgery works best when it's placed inside a bigger plan. That plan starts with diagnosis, moves through fracture repair and soft tissue management, and continues into rehabilitation of the jaw joints, muscles, bite, and airway. If you're a patient, that means knowing what to expect. If you're a referring doctor, that means knowing when to escalate care and when supportive treatment becomes just as important as the procedure itself.
Your Guide After a Facial Injury
The first hours after a facial injury are rarely clear. Patients are usually focused on what they can feel right away: pain, pressure, bleeding, loose teeth, difficulty opening the mouth, blurry vision, swelling, or a bite that suddenly doesn't fit. Just as often, they're thinking about what they can't tell yet, whether something is broken, whether they'll need plates or screws, and whether the damage is permanent.
The right first move is medical evaluation, not guesswork. If the injury followed a crash or another significant event, a practical overview of seeing a doctor after an accident can help people understand why prompt documentation and assessment matter even when adrenaline masks symptoms.
Pain also needs to be described clearly. Patients often say, “It hurts a lot,” but the quality and pattern of pain matter. A simple pain scale guide can help you communicate whether the pain is dull, sharp, constant, pressure-like, or triggered by chewing or speaking.
What deserves urgent attention
Some symptoms should never be watched casually at home.
- Trouble breathing: Any concern about airway compromise requires immediate emergency care.
- Vision changes: Double vision, loss of vision, or inability to move the eye normally needs urgent specialist assessment.
- A major bite change: If the teeth no longer come together the way they did before the injury, a fracture or displacement may be present.
- Uncontrolled bleeding or deep lacerations: These need direct evaluation and, in many cases, repair.
- Jaw locking or inability to open normally: This can signal fracture, joint injury, or significant muscle spasm.
Practical rule: If the face looks different, functions differently, or feels unstable after trauma, get it examined promptly.
Most worried patients assume facial trauma surgery is a single yes-or-no decision. It isn't. Good care follows a sequence. First, clinicians protect the airway and identify urgent threats. Then they define the injury precisely. Only after that do they decide whether observation, procedural repair, surgery, or later rehabilitation is the best path.
Understanding Your Facial Injury
The easiest way to think about facial trauma is to separate it into soft tissue injury and bony injury. Soft tissue includes skin, muscle, lining inside the mouth, and the supporting tissues around the lips, cheeks, and eyes. Bone injury means fractures of the jaw, cheek, nose, orbit, or forehead region.
Facial bones act like the frame of a house. If the frame shifts, doors stop closing correctly. In the face, that “door problem” shows up as a changed bite, facial asymmetry, eye position changes, numbness, or pain with chewing.

The injuries clinicians see most often
Not every fracture behaves the same way. Some are stable and minimally displaced. Others distort the facial skeleton enough that surgery is needed to restore function and appearance.
In a study of over 1,500 hospitalized facial trauma patients, zygomatic fractures accounted for 33.1% of cases and mandibular fractures for 31.6%, showing how common cheekbone and jaw injuries are in real practice (study on facial fracture patterns).
That pattern makes clinical sense:
- Cheekbone injuries: The zygomatic area is prominent and exposed during falls, sports injuries, and assaults.
- Jaw fractures: The mandible absorbs force during direct blows and often reveals itself through pain, swelling, tooth misalignment, or limited opening.
- Orbital injuries: The bones around the eye are thin and closely tied to vision and eye movement.
- Nasal injuries: The nose projects forward and breaks easily, though not every nasal injury needs operative treatment.
Why the same accident can create different problems
Two people can have the same mechanism of injury and very different outcomes. One may have bruising and lacerations only. Another may have a fracture pattern that changes the bite or eye position. That's why external appearance can be misleading. A patient with modest swelling may still have a significant structural injury.
A soft tissue wound also doesn't tell you whether the deeper support is intact. A clean-looking cut over the cheek may sit on top of a displaced cheekbone fracture. A split lip can coexist with dental injury or jaw instability. The real question isn't just, “Is there a break?” It's, “Has the injury altered structure, function, or both?”
Facial trauma isn't judged by bruising alone. The key issues are alignment, function, and what happens when the patient chews, speaks, breathes, and looks in all directions.
The Diagnostic Journey What to Expect
A proper facial trauma workup starts with the bedside exam. Before anyone talks about plates, screws, or follow-up therapy, the team needs to answer basic questions. Is the airway safe? Is vision affected? Is the bite stable? Are there numb areas that suggest nerve involvement? Is the facial skeleton tender, mobile, or visibly asymmetric?
Clinicians inspect and palpate with purpose. They look at eye position, pupil response, extraocular movement, dental occlusion, jaw range of motion, facial width, contour, lacerations, and areas of step-off where bone alignment may be disrupted. They also check whether pain worsens with function, especially chewing, clenching, or opening.
Why CT matters so much
Plain X-rays still have limited roles in some settings, but they don't define complex trauma well enough when surgical decisions are on the table. High-resolution CT scanning with 3D reformatting is the gold standard for evaluating facial trauma, because it lets surgeons visualize fracture lines and plan treatment in detail before entering the operating room (3D CT imaging in facial trauma planning).
That level of imaging helps answer practical questions such as:
- Where exactly is the fracture line?
- Has the bone rotated or collapsed inward?
- Is the orbital wall involved?
- Will the patient need open reduction and internal fixation?
- Is bone grafting or skeletal resuspension likely to be part of the repair?
What patients should expect during assessment
The diagnostic process often feels slow to patients because several teams may be involved. Emergency medicine may stabilize the patient first. Oral and maxillofacial surgery, ENT, plastic surgery, or ophthalmology may then join depending on the injury pattern.
That pace is usually a good sign, not a delay caused by uncertainty. Good facial trauma surgery depends on planning. Surgeons want a map before they rebuild.
A typical evaluation includes:
- Initial stabilization: Airway, bleeding control, neurologic status, and overall trauma assessment.
- Focused facial exam: Bite, jaw motion, numbness, lacerations, eye movement, contour, and tenderness.
- Imaging review: CT findings are matched to the physical exam.
- Specialist input: Eye, dental, sinus, or soft tissue concerns may change the surgical plan.
- Decision-making: Observation, urgent surgery, delayed surgery, or staged repair.
The best operation is usually the one that was planned from the clearest imaging, not the fastest one scheduled under uncertainty.
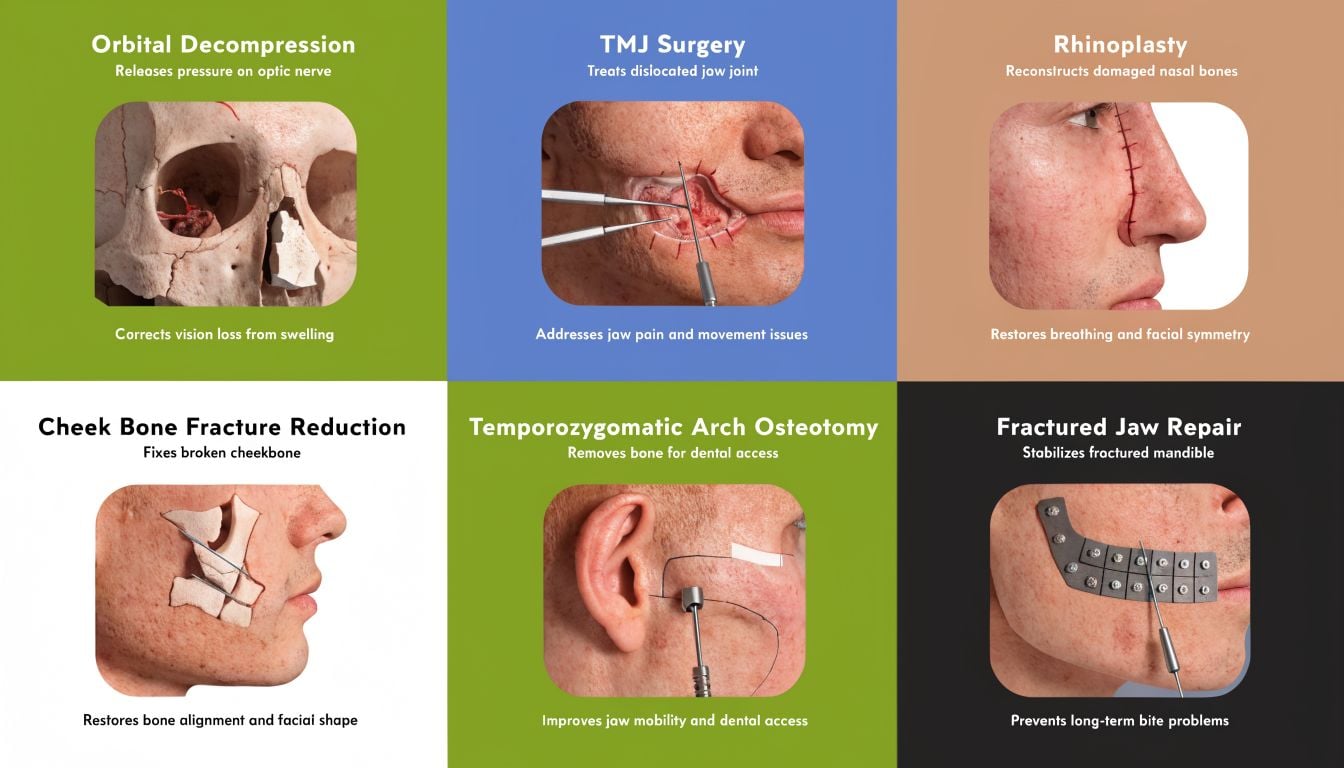
Common Facial Trauma Surgical Procedures
Most facial trauma surgery aims to do three things. Restore alignment, restore function, and protect appearance as much as possible. The exact procedure depends on the fracture pattern, the amount of displacement, and what the patient can no longer do normally.
Some fractures can be monitored. Others need operative repair because the bones won't heal in a functional position on their own. When patients hear that surgery is recommended, they often imagine a dramatic reconstruction. In reality, many procedures are precise structural repairs.
Open reduction and internal fixation
The most common concept patients should understand is open reduction and internal fixation, often shortened to ORIF. “Open reduction” means the surgeon exposes the fracture and returns the bone to the correct position. “Internal fixation” means small plates and screws hold it there while healing occurs.
A simple analogy helps. If a wooden frame cracks and shifts, taping the outside won't restore the original geometry. A skilled craftsperson has to line up the pieces and secure them from the inside so the structure heals straight. That's what ORIF does for many jaw, cheek, and orbital fractures.
Common goals of ORIF include:
- Jaw repair: Re-establish the bite and stabilize chewing forces.
- Cheekbone repair: Restore width and projection of the midface.
- Orbital repair: Support the eye and restore orbital volume when the socket has been disrupted.
- Frontal or upper facial repair: Protect contour and, in select injuries, adjacent sinus or cranial structures.
Soft tissue repair and orbital work
Laceration repair matters more than many patients realize. Good soft tissue closure isn't just “stitches.” It involves layered repair, careful edge handling, tension control, and alignment of natural borders such as the lip margin or eyelid. The cosmetic and functional result often depends on that detail.
Orbital fracture surgery has its own priorities. The surgeon may need to free trapped soft tissue, support the orbital floor or wall, and correct changes that could affect eye movement or position. The goal isn't cosmetic alone. It's visual function, comfort, and symmetry together.
How surgeons judge complexity
Not all fracture cases place the same demands on the operating team. The Facial Injury Severity Scale, or FISS, helps predict complexity. Scores above 6 are associated with longer surgeries, often exceeding 2 hours, and hospital stays longer than 1 week, which helps teams anticipate resources and staging needs (Facial Injury Severity Scale and surgical prediction).
For patients and referrers, the practical meaning is simple. A recommendation for surgery says nothing by itself about how “bad” the case is. One isolated fracture may be repaired efficiently. A panfacial pattern with multiple disrupted areas is a very different undertaking.
If you want a visual reference for how reconstructive specialists approach complex facial restoration, this overview of expert facial reconstruction procedures is a useful complement to the surgical concepts described here.
Clinical perspective: The operation succeeds when the patient can bite, breathe, speak, and heal in stable alignment. Hardware alone doesn't define success.
Your Recovery Timeline and Rehabilitation
Patients often prepare for the operation but not for the weeks after it. That's where expectations matter. Recovery depends on the fracture pattern, the tissues involved, pre-injury health, and whether the jaw, orbit, or multiple facial regions were affected. A retrospective study found that each additional facial fracture increased hospital stay by 5.82%, showing how strongly complexity shapes early recovery (hospitalization patterns in facial trauma).
The first days
The first forty-eight hours are usually dominated by swelling, bruising, fatigue, congestion, and soreness with movement. Numbness can also appear, especially when nerves were stretched or compressed by trauma or surgery. The face may look worse before it looks better because swelling peaks before it recedes.
Patients need a practical home setup. A preparation guide such as recovering from surgery at home can help with basics like positioning, cold therapy supplies, and eating modifications.
Key priorities in the first days include:
- Protect the repair: Follow instructions on mouth opening, chewing, nose blowing, and physical activity.
- Control swelling: Cold packs, elevation, and rest usually matter more than patients expect.
- Stay nourished: Soft or liquid foods are often necessary after jaw or midface surgery.
- Watch for red flags: Worsening pain, fever, drainage, visual change, or a bite that suddenly shifts should be reported.
The first two weeks
This phase is about consistency. Swelling gradually improves, but chewing may still be limited and speech may feel awkward if the lips, jaw, or occlusion were affected. Follow-up visits matter because the surgeon is checking stability, incision healing, sensory changes, and whether the bite remains where it should be.
Patients often underestimate how tiring recovery is. Pain may improve before normal stamina returns.
A focused jaw surgery recovery guide can also help patients understand what eating, hygiene, and functional progress may look like after procedures involving the mandible.
The first few months
By this stage, the question changes from “Did the repair heal?” to “Did function return well?” Bone healing and functional recovery aren't always the same. A patient may have a healed fracture and still report jaw deviation, muscle guarding, headaches, or joint pain with chewing.
Rehabilitation is decisive at this stage. The goal is a gradual return to normal eating, work, exercise, and speech without forcing the system too early. Good recovery isn't passive. It requires monitoring, guided progression, and attention to the bite, TMJ, soft tissue mobility, and muscle patterning.
Beyond Surgery Regenerative and Supportive Care
This is the part many standard facial trauma surgery guides skip. A technically successful repair can still leave the patient with post-traumatic TMJ dysfunction, protective muscle tension, scar restriction, headache patterns, or persistent pain during chewing. The bone may be stable while the system around it remains dysfunctional.
That gap matters most in jaw injuries, condylar injuries, bite changes, and cases where patients clench in response to pain. It also matters after immobilization, when muscles lose coordination and the joint no longer tracks smoothly.
Why non-surgical care belongs in the plan
Standard resources on facial trauma surgery often overlook non-surgical and regenerative options, even though they can help patients who want to avoid unnecessary invasive care or improve recovery after surgery. Clinic-based therapies such as PRF and cold laser therapy can help address that gap, especially for post-traumatic TMJ pain (discussion of the non-surgical gap in facial trauma resources).
That doesn't mean regenerative care replaces surgery when a fracture is displaced or unstable. It means the best long-term outcome often comes from combining structural repair with biologic and functional rehabilitation.
Examples of supportive care include:
- PRF treatment: Used in clinical regenerative settings to support healing responses in injured tissues.
- Cold laser therapy: Often used to calm irritated tissue and support recovery in painful regions.
- Manual and exercise-based TMJ rehab: Helpful when the jaw opens unevenly, clicks, deviates, or fatigues quickly.
- Scar and soft tissue management: Important when facial movement is limited by tissue stiffness.
- Breathing and oral posture retraining: Relevant when trauma alters oral rest posture or mouth breathing becomes habitual.
Function has to be retrained
After trauma, patients often unconsciously adapt in unhelpful ways. They chew on one side, guard the jaw, thrust the head forward, or breathe through the mouth because opening feels unsafe. Those compensations can maintain pain even after the fracture has healed.
That's why I don't view rehabilitation as an optional add-on. If the injury involved the jaw, bite, joint, tongue posture, or airway pattern, function has to be retrained deliberately. In selected cases, a broader look at regenerative medicine for joint pain also helps patients understand where biologic support may fit into recovery planning.
Surgery restores structure. Rehabilitation restores use. Patients usually need both to feel fully recovered.
Frequently Asked Questions About Facial Trauma
Patients usually ask the most important questions after the first shock wears off. They want to know what will look normal again, what function should return, and when lingering symptoms become a problem rather than a normal part of healing.
Quick answers to common concerns
| Question | Answer |
|---|---|
| Will I always have visible scars? | Not necessarily. Scar visibility depends on the location of the injury, how the wound was repaired, skin quality, tension across the closure, and how healing progresses. Many incisions used in facial trauma surgery are placed in natural creases, inside the mouth, or in less visible locations when possible. |
| How do I know whether my jaw pain after trauma is “normal”? | Early soreness is expected. Ongoing pain with chewing, jaw locking, deviation on opening, headaches, or a bite that still feels off deserves further evaluation. Persistent symptoms often point to joint, muscle, or occlusal dysfunction rather than just routine healing. |
| Can a fracture heal and still leave me with TMJ problems? | Yes. Bone union and joint function aren't the same thing. A patient may heal structurally but still develop muscle guarding, altered bite mechanics, or TMJ irritation that needs targeted treatment. |
| When should a facial pain specialist get involved? | Usually when pain, jaw dysfunction, limited opening, chewing difficulty, headaches, or sleep-related symptoms continue after the acute surgical phase, or when those symptoms become the main obstacle to recovery. |
| Will I need surgery for every facial fracture? | No. The decision depends on displacement, instability, bite change, eye involvement, airway concerns, and whether normal form and function can be preserved without an operation. |
| What should a referring doctor watch for after surgery? | Persistent malocclusion, progressive limitation in opening, worsening asymmetry, sensory complaints that don't improve, chronic facial pain, and signs that the patient has shifted into protective chewing or breathing patterns. |
What patients can do to improve outcomes
A better recovery usually comes from small disciplined steps rather than one dramatic intervention.
- Keep follow-up appointments: The surgeon and rehabilitation team need to catch subtle problems early.
- Report function, not just pain: Tell your clinician if chewing, speaking, swallowing, or breathing feels different.
- Don't force the jaw: Pushing range too aggressively can prolong irritation.
- Protect nutrition: Healing is harder when patients avoid eating because chewing feels awkward.
- Ask about rehabilitation early: If the bite, TMJ, or facial muscles still feel abnormal, waiting too long rarely helps.
A patient who says, “The fracture healed, but my jaw still doesn't feel right,” is giving useful diagnostic information, not complaining too much.
For referring clinicians, the key is timing. Early surgical referral is necessary when structure is unstable. Later specialty referral is necessary when function doesn't normalize. Those are different moments in care, and both matter.
If you're dealing with lingering jaw pain, TMJ dysfunction, facial muscle tension, headaches, or sleep-related issues after facial trauma, Pain and Sleep Therapy Center offers specialized evaluation focused on root-cause recovery. Their team treats the problems that often remain after the fracture itself has healed, including post-traumatic TMJ symptoms, dysfunctional breathing patterns, and persistent facial pain, with personalized rehabilitation and regenerative care options.



