
The call usually comes after a prenatal ultrasound, or in the first hours after birth. A parent hears the word cleft, then everything else becomes a blur. Feeding. Surgery. Speech. Appearance. Breathing. Future. Most families don't need more medical jargon in that moment. They need a calm roadmap.
That roadmap does exist. Cleft care follows a sequence that has been refined over many years, and each step has a reason behind it. The age for surgery is not arbitrary. Surgeons time repair around feeding safety, speech development, tissue growth, hearing, and facial development. When those pieces are coordinated well, a child gets more than a repaired lip or palate. They get a stronger foundation for eating, speaking, breathing, sleeping, and jaw function as they grow.
Parents often tell me the hardest part is not knowing what comes next. A notebook helps. A shared family calendar helps. Some families also like simple digital systems for appointments, questions, and medication notes, which is why resources on organizing family life on Everblog can be useful during the early months when everything feels fragmented.
The Journey Ahead After a Cleft Diagnosis
The first stretch after diagnosis is emotional for good reason. You're trying to absorb new information while caring for a baby who still needs to eat, sleep, gain weight, and be comforted like any other infant. Referring doctors often feel that same urgency from a different angle. They want to get the family to the right team quickly and avoid delays that can ripple through feeding, speech, and later development.
What parents usually need first
Most families ask the same early questions:
- When is the first surgery? They want a date, or at least a window, so the future feels less open-ended.
- Will my baby be able to feed and grow well enough? That concern is immediate and practical.
- How many specialists are involved? Parents want to know whether this is one operation or a longer process.
- Will this affect speech, breathing, or the jaw later on? That question often comes once the initial shock settles.
A cleft diagnosis starts a longitudinal care plan, not a single event. That can sound intimidating at first, but it's also reassuring. The child isn't expected to “get through surgery” and then manage everything else alone. Good cleft care follows the child over time, adjusting support as speech develops, teeth erupt, hearing is monitored, and facial growth changes.
The best cleft teams don't just close a gap. They protect function at every stage of growth.
Why timing matters so much
The phrase cleft palate surgery age matters because age is really shorthand for developmental readiness. Surgeons are watching for safe anesthesia, adequate tissue size, feeding stability, and the right moment to support normal speech patterns before unhelpful compensations become ingrained.
That's why the timeline has distinct stages instead of a one-size-fits-all operation. The lip is usually addressed early for feeding mechanics, facial form, and muscle continuity. The palate follows in a separate window because its role in speech, swallowing, and pressure control is different. Later interventions may support dental eruption, jaw alignment, and airway function.
Families do better when they understand the “why” behind each step. Once the sequence makes sense, the path usually feels less frightening and more manageable.
The First Step Cleft Lip Repair Timing
A common early clinic visit goes like this. Parents ask whether the lip should be repaired as soon as possible, while the surgical team is still checking weight gain, feeding stamina, and overall medical stability. The right timing is early, but it is never rushed for its own sake.
Cleft lip repair usually happens in the first several months of life, often around 3 to 6 months. Many teams still use the rule of 10s as a practical screening guide: at least 10 weeks of age, about 10 pounds in weight, and a hemoglobin of 10 g/dL. Those numbers are not a deadline. They help the team judge whether an infant is ready for surgery and safe pediatric oral surgery anesthesia planning.

That distinction matters in practice. A baby who is small but steadily gaining may be close to ready. A baby with poor feeding, reflux, a heart condition, or a recent respiratory illness may need more time. Delaying a few weeks to improve nutrition or reduce anesthesia risk often leads to a safer operation and a smoother recovery.
Lip repair changes more than appearance. The surgeon is re-creating continuity of the orbicularis oris muscle, restoring the muscular ring of the mouth so the lip can function more normally. That affects latch and seal, but it also influences how the nose, upper lip, and front of the maxilla grow under muscular pressure over time.
This is one reason timing has long-term importance. Early restoration of lip muscle balance supports more typical orofacial function during infancy, when feeding patterns, nasal airflow, and facial posture are still developing. In children with cleft conditions, those early patterns can shape later jaw mechanics and airway habits. Good cleft care starts with closure, but the larger goal is healthy growth.
Parents can expect several benefits from this first operation:
- Better lip seal during feeding, even if specialized bottles or feeding support are still needed
- Improved muscle alignment across the upper lip
- Better support for nasal symmetry as the face grows
- A clearer starting point for the rest of the treatment plan
I also tell families what lip repair does not do. It does not finish treatment, and it does not solve every feeding or airway concern on its own. Children still need follow-up for palate repair, hearing, speech, dental development, and facial growth. For some, that later follow-up is where we protect sleep quality, nasal breathing, and jaw function in a more meaningful way.
For referring providers, the practical message is simple. Send the child early, even if surgery is still weeks away. Feeding support, presurgical planning, and coordinated cleft team evaluation should begin well before the operating room date.
The Critical Window for Cleft Palate Surgery
Palate repair is more nuanced than lip repair. The key question isn't just “When can the surgeon close the palate?” It's “When can the surgeon close it safely, with enough tissue for a sound repair, while still protecting speech development?”
That's where the idea of a critical window comes in.
Why this timing is more variable
Cleft palate surgery is typically performed in infancy, often somewhere within 6 to 18 months, depending on the cleft pattern, the child's health, the surgeon's protocol, and the center's philosophy. The palate has to be large enough for a durable repair, but not so late that the child starts building persistent compensatory speech patterns.
For isolated cleft palate, a landmark trial supported by the National Institute of Dental and Craniofacial Research found that surgery at 6 months led to better speech-related outcomes than surgery at 12 months. By age five, the earlier-surgery group had a lower rate of velopharyngeal insufficiency, 9% versus 15%, although the earlier group also showed somewhat higher rates of dental arch constriction, according to NIDCR's summary of the isolated cleft palate trial.
That finding matters because velopharyngeal insufficiency affects how well the palate closes against the back of the throat during speech. If that seal is weak, speech can sound overly nasal and some sounds become difficult to produce clearly.
The trade-offs that families should know
Parents deserve the full picture, not a simplified slogan about “earlier is always better.” In practice, the team is balancing several real trade-offs:
- Speech protection: Earlier repair may help the child develop clearer speech patterns.
- Tissue and closure mechanics: The surgeon still needs enough growth to close the palate without excessive tension.
- Dental and facial growth considerations: Some early approaches may carry trade-offs for arch shape.
- Overall medical readiness: Nutrition, airway status, syndromic features, and anesthesia considerations all matter.
A thoughtful cleft surgeon doesn't chase one outcome while ignoring the others. The goal is not an early operation. The goal is a repair timed to give the child the best functional path forward.
Questions that improve the consultation
These questions usually lead to a stronger discussion with the surgical team:
- What palate repair age do you recommend for this specific cleft pattern?
- How does that timing support speech development in this child?
- What trade-offs are you weighing around growth and closure tension?
- What should we expect from anesthesia and recovery?
For families who want to better understand sedation and perioperative planning, it can help to review a clear overview of oral surgery anesthesia options.
A good palate plan is individualized. The same age doesn't fit every anatomy, even when the developmental goals are shared.
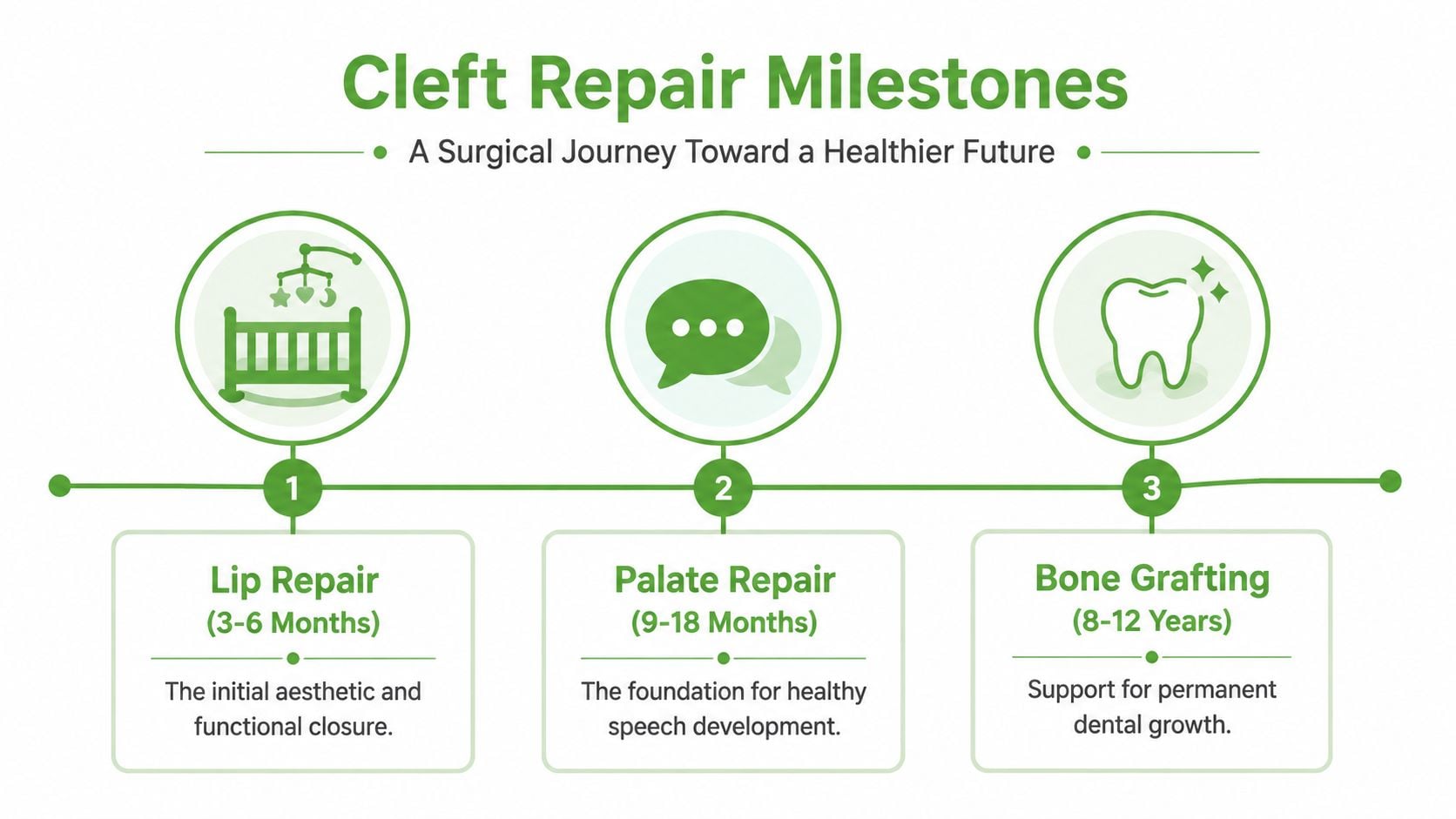
A Visual Timeline of Cleft Repair Milestones
At a first team visit, many parents want one answer: When will the surgeries happen? The more useful answer is a roadmap. A cleft timeline shows how each decision supports the next stage of development, from feeding and hearing in infancy to speech, dental eruption, jaw growth, and later breathing during sleep.
Why the sequence is built this way
The timeline follows function, not just calendar age. Early visits focus on safe feeding, weight gain, and identifying airway or syndromic concerns that can change surgical planning. Lip and palate procedures come next, but those repairs are only part of the job. Ongoing follow-up protects hearing, guides speech development, and watches how the upper jaw, dental arch, and nasal airway are growing together.
Reviews of cleft timing and outcomes support palate repair in late infancy because that window can balance speech goals with closure mechanics and growth considerations, as discussed in this PubMed Central review on cleft palate timing and outcomes. In practice, that means the sequence is designed to reduce avoidable problems later, including compensatory speech patterns, persistent fistula concerns, bite problems, and airway issues that may not become obvious until childhood or adolescence.
That long view matters.
A child with a well-healed repair may still need help with resonance, orthodontic guidance, or evaluation for sleep-disordered breathing. Families who understand that early tend to feel less blindsided later, especially if snoring, restless sleep, or mouth breathing raise concern for pediatric sleep apnea treatment.
Typical cleft care timeline
| Age Range | Key Milestone or Intervention | Primary Goal |
|---|---|---|
| Birth to early infancy | Initial craniofacial evaluation, feeding support, care planning | Support feeding, growth, airway review, and referrals |
| 3 to 6 months | Lip repair | Rebuild lip muscle continuity and improve early oral function |
| 9 to 18 months | Palate repair | Separate the oral and nasal cavities and support clearer speech development |
| Early childhood | Speech, hearing, dental, and growth follow-up | Identify functional problems while they are still easier to address |
| 8 to 12 years | Bone grafting if needed | Support eruption of permanent teeth and improve arch continuity |
| Adolescence | Orthodontic and possible jaw evaluation | Address bite, facial balance, nasal airflow, and jaw function |
What parents and referring doctors should expect over time
It helps to think in phases.
The first phase is about stability. Feeding, growth, airway safety, and readiness for anesthesia come first.
The next phase is developmental. Speech, middle ear health, tongue posture, swallowing patterns, and dental eruption start to matter more because they influence how the face and airway function over time.
The later phase is growth-related. During this stage, the team looks carefully at the bite, arch form, jaw position, nasal breathing, and whether the child is showing signs of sleep disturbance or strain in the jaw joints.
A successful infancy repair is an important start. It is not the end of cleft care. The strongest long-term outcomes usually come from coordinated follow-up that connects each milestone to the child's future speech, facial growth, airway health, and comfort.
Beyond Repair Connecting Surgery to Lifelong Airway Health
Closing the cleft is the beginning. It isn't the end of the functional story.

A child's palate is part of a larger breathing and jaw system. The way the palate functions influences oral pressure, tongue posture, swallowing patterns, resonance, and nasal airflow. The way the face grows after repair can also shape the airway for years to come. That's why the cleft palate surgery age discussion shouldn't stop at speech and appearance.
Why airway and jaw function belong in the conversation
One often overlooked issue is the relationship between repair timing, midface growth, and later airway health. A review aimed at this broader discussion notes that while palate repair at 9 to 15 months is standard, 20 to 30% of cleft patients still develop obstructive sleep apnea that can persist into adulthood, often in the setting of midface hypoplasia, as discussed in this review on ideal age and long-term cleft considerations.
That doesn't mean surgery causes sleep apnea in a simple one-to-one way. It means craniofacial growth, scar behavior, jaw position, nasal breathing, and oral muscle patterns all interact over time. Some children grow into a stable airway. Others need long-term monitoring because their anatomy and function start pushing in the wrong direction.
What root-cause follow-up looks like
When follow-up is done well, the team watches for signs that the child is compensating rather than functioning efficiently:
- Mouth breathing: This can become a habit if nasal airflow is poor.
- Low tongue posture: This affects palatal shape and swallowing mechanics.
- Jaw strain: Abnormal bite relationships can load the TM joints unevenly.
- Fragmented sleep: Parents may notice snoring, restless sleep, or daytime fatigue.
That is where non-surgical care can matter. Speech therapy may be part of the picture. So can orthodontic guidance, airway evaluation, and in selected cases orofacial myofunctional therapy to improve nasal breathing, lip seal, and tongue function.
For families worried about nighttime breathing as a child grows, it may help to review signs and treatment pathways for pediatric sleep apnea treatment.
A short overview of airway-centered thinking can also help frame the bigger picture:
The surgery may happen in infancy. The functional consequences of that anatomy can keep evolving through childhood and adolescence.
Assembling Your Child's Multidisciplinary Care Team
A child with a cleft doesn't need one excellent clinician. That child needs a coordinated team that communicates well.
This matters everywhere, but it becomes especially visible when systems are strained. In many low- to middle-income countries, children experience major delays, with an average initial cleft surgery age of 3.25 years, and 83% of cases rely on charitable organizations outside national systems, according to the American Society of Plastic Surgeons report on barriers to cleft lip and palate surgery. The lesson applies broadly. Access and coordination change outcomes.
Who should be at the table
A strong cleft team usually includes several core roles:
- Plastic or craniofacial surgeon: Plans and performs staged repair, then monitors healing and growth impact.
- Pediatrician: Tracks weight gain, general health, readiness for surgery, and routine development.
- Speech-language pathologist: Evaluates resonance, articulation, and whether speech is using normal pressure patterns.
- Audiologist and ENT: Monitor hearing and middle ear function, which often need close attention in cleft care.
- Orthodontist or pediatric dentist: Follows dental eruption, arch form, and later bite development.
- Orofacial myofunctional therapist: Helps evaluate breathing pattern, oral posture, and swallow function when those become relevant.
Where collaboration changes the outcome
The best referrals happen before a problem becomes entrenched. A baby who can't feed well should not wait for surgery before getting practical help. A child with unclear speech should not be assumed to “grow out of it” without a structured assessment. A child with chronic mouth breathing or a narrow arch deserves an airway-informed evaluation, not a fragmented set of opinions.
Tongue mobility can also influence oral posture and feeding in some children, which is why some providers look at resources related to pediatric tongue-tie specialists when sorting through the broader oral function picture.
The most effective cleft care is collaborative. No single specialist can see the whole child alone.
Frequently Asked Questions for Parents and Providers
Parents often save their hardest questions for the end of a visit. Referring doctors often have the same questions but ask them in clinical language. Both are usually asking about the same things: safety, timing, long-term function, and whether they're missing something important.
Will my child need more than one surgery
Often, yes. Lip and palate repair are separate milestones, and some children later need support for dental eruption, bone grafting, speech-related revision, or jaw alignment. The exact path depends on the cleft type, growth pattern, and how function develops over time.
What are the main risks of surgery
The care team will review the specific surgical and anesthesia risks for your child. In practice, the main concern for families is usually not just the operation itself, but whether the child is medically ready and whether recovery will protect feeding, hydration, and healing. That's why preoperative assessment is so important.
How do I prepare my baby for surgery
Focus on what you can control:
- Protect growth: Keep feeding support front and center so weight gain stays on track.
- Keep records: Bring feeding notes, medication lists, and all specialist recommendations to appointments.
- Ask for specifics: Request clear instructions about feeding after surgery, pain control, and incision care.
- Prepare your home rhythm: Arrange help for the first stretch after surgery so one adult isn't carrying everything alone.
Will this affect my child's speech forever
Not necessarily, but speech deserves close follow-up. Early repair supports better function, yet some children still need speech therapy or further evaluation for resonance and pressure-related speech issues. The important thing is not to assume that speech is “fine” without listening carefully as language develops.
Can cleft repair influence future jaw pain or sleep
Yes, it can influence the structures that shape later jaw and airway function. That doesn't mean a child is destined to develop TMJ problems or sleep-disordered breathing. It means those areas should be watched as part of whole-child follow-up, especially if there are signs such as mouth breathing, snoring, bite asymmetry, facial tension, or chewing fatigue.
When should a provider refer to a cleft team
As early as possible. Prenatal referral is ideal when the diagnosis is known before birth. After delivery, referral should happen immediately so feeding support and care planning begin before delays create avoidable problems.
Parents do best when they leave the visit knowing the next step, the reason for it, and who to call if something changes.
If your child has a history of cleft repair and now struggles with mouth breathing, snoring, restless sleep, jaw tension, or oral function concerns, Pain and Sleep Therapy Center offers airway-focused, root-cause evaluation for pediatric sleep, jaw function, and orofacial development. The team works from a whole-child perspective to help families understand how breathing, oral posture, swallowing, and facial growth fit together over time.



