
Your child finally falls asleep. Then the noises start. Snoring. A pause. A little gasp. Maybe a sweaty forehead, a twisted blanket, a new habit of sleeping with the neck stretched back. By morning, everyone is tired, but your child may not look tired in the way adults do. Instead, they're irritable, wild, unfocused, emotional, or suddenly struggling at school.
That's the pattern many parents miss at first. They think they're dealing with separate problems. Bad sleep at night. Tough behavior during the day. Mouth breathing. Bedwetting. Trouble paying attention. But these can belong to the same story.
Child sleep apnea symptoms often show up as an airway problem that affects sleep quality, behavior, and development all at once. Pediatric obstructive sleep apnea affects an estimated 1% to 5% of children, while broader sleep-disordered breathing symptoms are reported in 4% to 11% of children, according to a pediatric review of prevalence and symptoms. That means this is not rare, and it's not something parents should feel embarrassed for asking about.
If you've been wondering whether your child is “just a bad sleeper” or whether something more is going on, that question is worth taking seriously. A good starting point is learning how pediatric sleep disorders can affect breathing, behavior, and daily function.
Is It More Than Just a Bad Night's Sleep
A lot of parents arrive at this question after months of second-guessing themselves. They've noticed the snoring. They've seen the tossing and turning. They've watched their child wake up cranky, struggle through school, or melt down over small things. Still, they hesitate because the pattern doesn't always look dramatic.
Some children with sleep-disordered breathing look busy, not sleepy. They may seem “wired,” impulsive, or hard to settle. Others breathe through their mouths, sweat during sleep, or wake up in odd positions that seem uncomfortable but somehow help them breathe a little better.
Children don't always tell us they slept badly. They show us through their mood, focus, and body language.
That's why parents often describe a feeling that something is off, even before they have the right words for it. They know their child isn't getting restful sleep, but they may not realize the airway could be part of the reason.
When the pattern starts to connect
The key is to look at the whole picture, not one symptom in isolation. A child who snores once during a cold isn't the same as a child who snores regularly, breathes through the mouth, and seems dysregulated during the day. A child who wets the bed occasionally isn't the same as one who also sleeps restlessly and wakes up unrefreshed.
These details matter because child sleep apnea symptoms often cross categories. They affect sleep, breathing, attention, emotion, and sometimes growth and learning. When parents connect those dots, the problem usually becomes less mysterious and more manageable.
What works better than waiting
What helps is observation. What doesn't help is assuming your child will outgrow every nighttime symptom. Some children do improve as circumstances change. Others keep working too hard to breathe every night, and the daytime consequences build slowly.
If your child's sleep looks noisy, effortful, restless, or unusually disruptive, it's reasonable to treat that as a medical question, not a personality trait.
The Nighttime Clues Your Child Is Giving You
Nighttime symptoms are often the first clues, but parents don't always know which ones are meaningful. Some signs are obvious. Others are easy to dismiss as quirks.
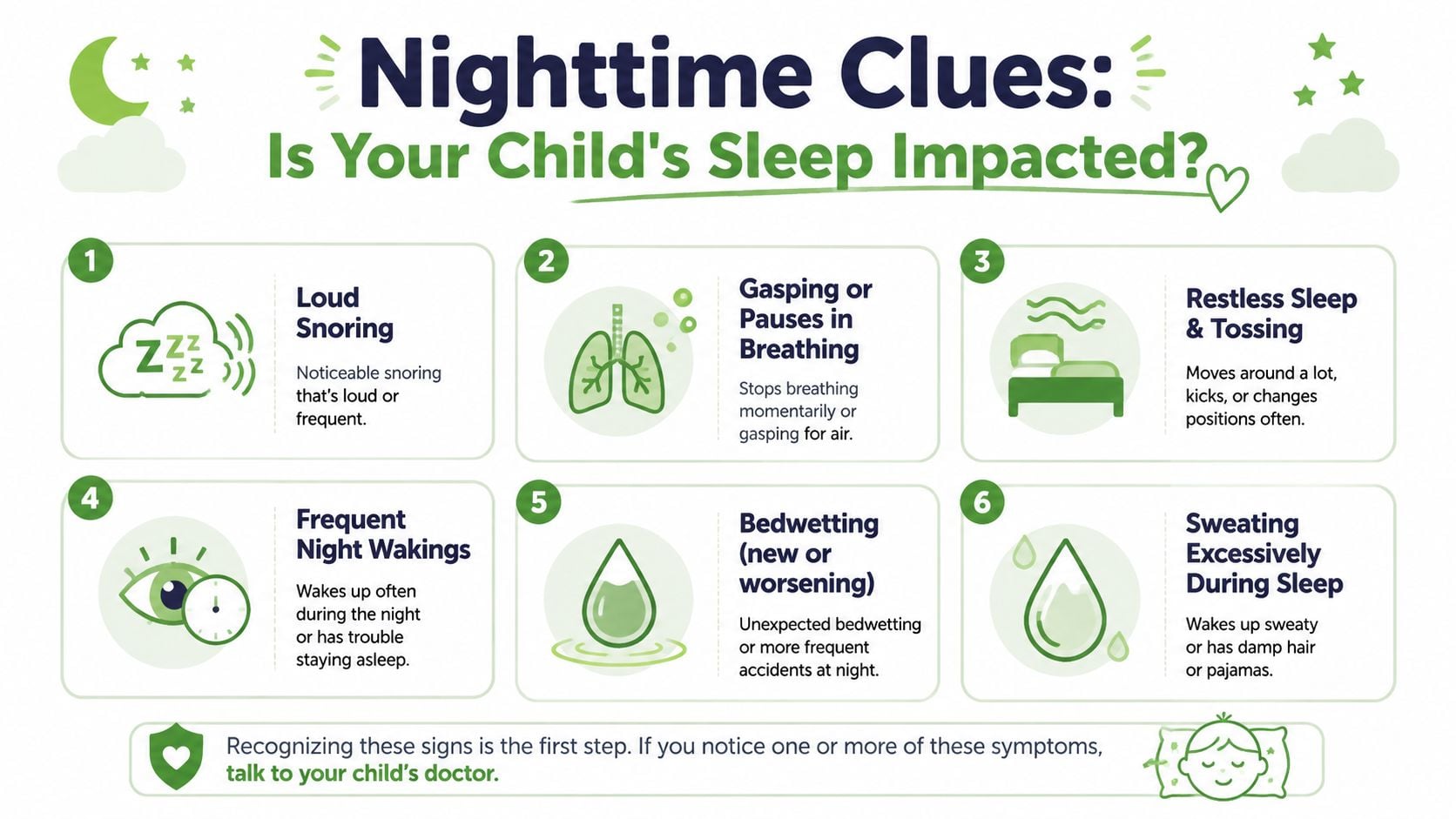
Loud clues
These are the sounds and events that make parents sit up and listen.
- Snoring that happens often: Not just an occasional stuffy-night snore, but a recurring pattern.
- Gasping, choking, or snorting: These sounds can suggest the airway is narrowing or briefly blocked.
- Witnessed pauses in breathing: A child may become quiet for a moment, then restart breathing with effort.
- Noisy breathing during sleep: Sometimes the sound isn't classic snoring. It may sound strained or labored.
Quiet clues
These signs matter because not every child with obstructive sleep apnea puts on a loud nighttime performance.
- Restless sleep: Constant tossing, turning, or tangled sheets.
- Mouth breathing: A child sleeps with lips open because nasal breathing isn't happening well.
- Night sweats: Excessive sweating during sleep can appear alongside breathing effort.
- Odd sleep positions: Neck extended, face tipped upward, bottom in the air, or other positions that seem designed to open the airway.
- Frequent wake-ups: Some children briefly arouse over and over without fully waking enough to remember it.
- Bedwetting that is new or worsening: This can sometimes be part of the pattern.
Nighttime Sleep Apnea Symptoms in Children
| Symptom Type | What to Look and Listen For |
|---|---|
| Loud clue | Regular snoring that stands out from normal quiet breathing |
| Loud clue | Gasping, choking, or snorting sounds during sleep |
| Loud clue | Breathing pauses followed by a bigger breath |
| Loud clue | Labored or noisy breathing through the night |
| Quiet clue | Mouth open during sleep and persistent mouth breathing |
| Quiet clue | Restless tossing, kicking, or constant repositioning |
| Quiet clue | Unusual sleep postures that seem to help breathing |
| Quiet clue | Heavy sweating at night without another clear reason |
| Quiet clue | Repeated wake-ups or very unsettled sleep |
| Quiet clue | Bedwetting, especially when it appears with other airway signs |
Practical rule: Don't judge your child's sleep from one minute at bedtime. The useful clues usually show up after they've been asleep for a while.
Why these clues happen
Pediatric obstructive sleep apnea is caused by partial or complete upper-airway blockage during sleep, most commonly from enlarged tonsils and adenoids in younger children. Mayo Clinic notes that a child may have snoring, mouth breathing, gasping or choking, morning headaches, and daytime hyperactivity or poor school performance, even when they don't look obviously sleepy, in its overview of pediatric sleep apnea symptoms and causes.
That airway blockage doesn't need to be complete to matter. Even repeated narrowing can fragment sleep and make breathing harder all night long. Parents often focus on the loudest symptom, but the quieter signs are sometimes what complete the picture.
What tends to mislead families
A common mistake is thinking, “If it were serious, I'd hear loud snoring every night.” That isn't always true. Some children have more subtle sleep disruption. Others sound worse in certain positions or only part of the night.
The better question is this: Does my child look like they are sleeping peacefully, or like they are working to sleep? If it looks like work, that's worth discussing with a qualified clinician.
How Sleep Apnea Shows Up During the Day
Many parents expect poor sleep to create a sleepy child. In pediatrics, it often does the opposite.

A child who isn't breathing well at night may wake up looking active, oppositional, scattered, or emotionally brittle rather than drowsy. That's one reason child sleep apnea symptoms get mistaken for temperament issues, school problems, or a stage the child will “grow out of.”
St. Louis Children's Hospital notes that, unlike adults, children with sleep apnea often show behavioral issues rather than overt sleepiness, including irritability, impulsivity, and attention problems, in its guide to pediatric sleep apnea signs. That's a major reason daytime clues deserve real weight.
The behavior signs parents notice first
Parents often describe changes like these:
- Short fuse: More irritability, emotional swings, or easy frustration.
- Busy but unfocused behavior: A child seems constantly in motion but struggles to sustain attention.
- School difficulties: Trouble listening, remembering directions, sitting still, or learning efficiently.
- Morning complaints: Headaches, crankiness, dry mouth, or a rough start to the day.
- Restless regulation: They're tired in a dysregulated way, not a calm, sleepy way.
Some children do get sleepy during the day. But many don't. That's the trap.
Why the daytime pattern gets mislabeled
When the brain gets fragmented sleep night after night, the effects show up where children are asked to perform. In the classroom. At homework time. During transitions. Around siblings. During sports or activities that require attention and self-control.
A child may look defiant when they're exhausted. They may look inattentive when they're running on poor-quality sleep. They may look “high energy” when their nervous system is compensating.
If your child's behavior changed around the same time as snoring, mouth breathing, bedwetting, or restless sleep, don't treat those as separate stories.
This short video gives a helpful overview of what parents may observe when sleep-disordered breathing affects a child's days as well as nights.
The symptom many families miss
Another important point is that some children with sleep apnea may not snore at all. A broader pediatric review explains that daytime symptoms can be subtle and easy to miss, and that infants and young children may not snore even when obstructive sleep apnea is present, as discussed in this review on pediatric OSA recognition.
That matters because parents often search for “snoring” and stop there. If your child has hyperactivity, poor attention, learning difficulty, morning headaches, bedwetting, or restless sleep, the airway still belongs on the list of possibilities.
A development-focused way to think about it
Sleep is when the body restores itself. If breathing keeps interrupting that process, the effects won't stay confined to the bedroom. They can spill into mood, learning, resilience, and daily function.
The practical takeaway is simple. If daytime struggles don't fully make sense on their own, look backward at the night.
Understanding the Causes of Child Sleep Apnea
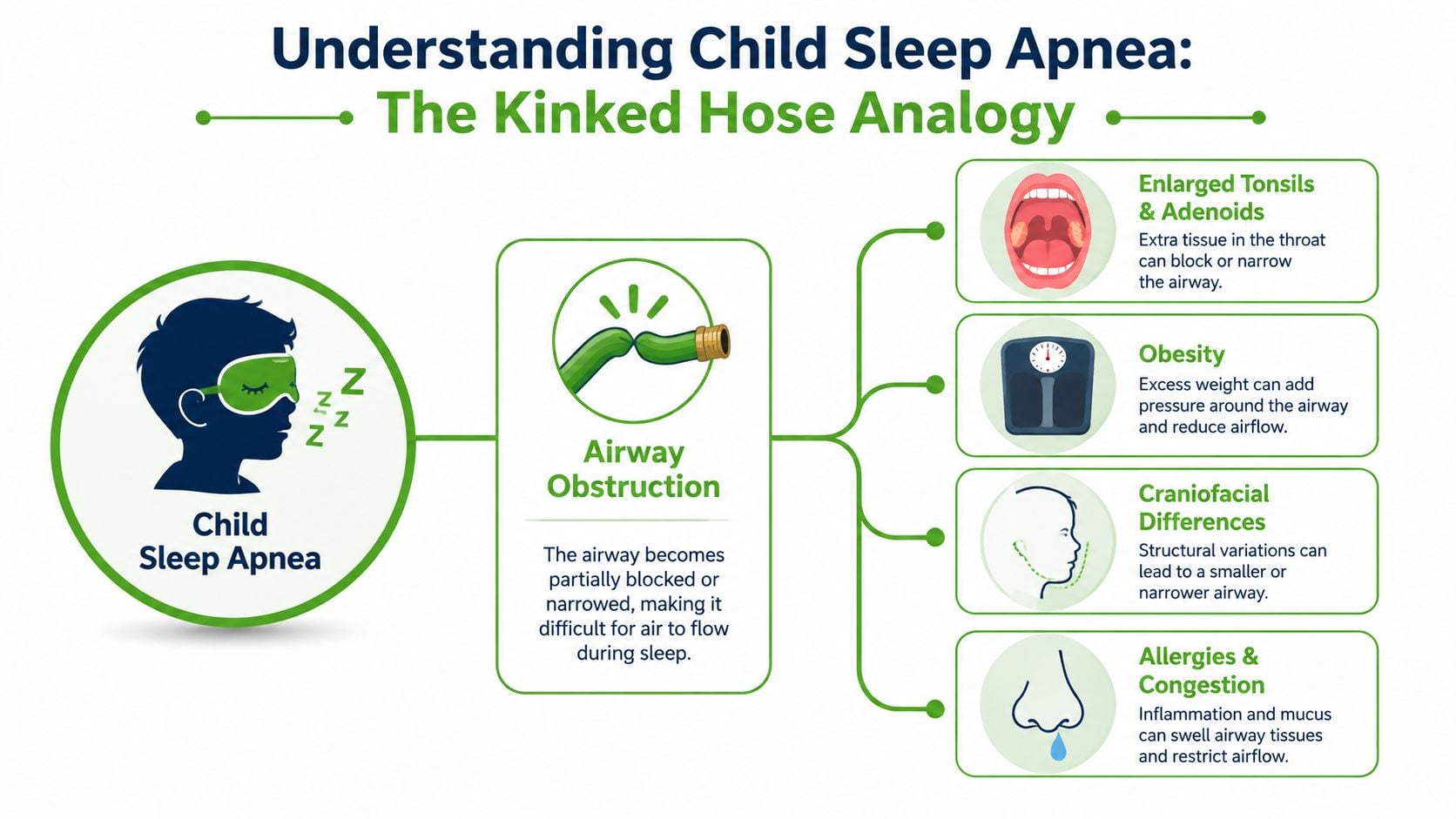
The easiest way to understand pediatric obstructive sleep apnea is to think about a garden hose with a kink in it. Water still tries to move through, but the passage is narrowed. Pressure changes. Flow becomes noisy and irregular. Sleep breathing works in a similar way when the airway is crowded or collapses during sleep.
The most common cause
In younger children, the most common physical blocker is enlarged tonsils and adenoids. They take up space in the back of the throat and behind the nose. When the muscles relax during sleep, that crowded space can narrow even more.
This is why some children breathe loudly, gasp, or seem to work hard to move air at night. It's not just “deep sleeping.” It's a mechanical problem with airflow.
Other factors that can narrow the airway
Not every child has the same reason for airway obstruction. Several contributors can overlap:
- Body size and tissue volume: Obesity becomes a more important contributor in teenagers.
- Nasal congestion: Allergies, chronic stuffiness, and poor nasal breathing can push a child toward mouth breathing.
- Jaw and facial structure: A narrow palate, a recessed lower jaw, or limited room for the tongue can crowd the airway.
- Oral posture patterns: If the tongue rests low and the lips stay open, that can reinforce less efficient breathing patterns over time.
The airway is not just a throat issue. The nose, palate, tongue posture, and jaw all influence how easily a child can breathe during sleep.
Why root-cause thinking matters
Treatment decisions warrant increased consideration. If enlarged tonsils and adenoids are the major issue, that deserves attention. But if a child also has poor nasal breathing, a narrow upper jaw, low tongue posture, or dysfunctional oral habits, removing one obstruction may not solve the entire breathing pattern.
That's why a root-cause approach matters. Families do best when clinicians ask not only, “What is blocking the airway?” but also, “Why is the airway struggling in the first place, and what can support healthy growth from here?”
What doesn't work well
What usually doesn't help is reducing the problem to one symptom or one body part. A child who snores may also need evaluation of nasal breathing. A child who had surgery may still need help with tongue posture or mouth breathing habits. A child with “behavior issues” may need an airway workup.
The more precisely the cause is defined, the more targeted the treatment can be.
The Path to a Clear Diagnosis
Parents often worry that diagnosis will be complicated or intimidating. In reality, the process is usually straightforward. The hard part is often deciding to look into it.

What a good evaluation looks for
A thorough evaluation starts with pattern recognition. The clinician listens for nighttime symptoms, daytime behavior changes, and signs of airway effort. Then the exam looks at structures that influence breathing, such as the nose, tonsils, oral posture, palate shape, and jaw relationship.
This kind of visit is not just about checking a box for snoring. It's about understanding whether the child's sleep and daytime function point to a breathing problem.
When a sleep study comes in
An overnight sleep study, also called a polysomnogram, is the standard way to measure what happens during sleep. Parents are often relieved to learn that it's observational. The goal is to record breathing and sleep, not to put the child through a painful test.
If you're trying to understand the practical side of testing, this overview of how to diagnose sleep apnea at home can help frame the conversation about what screening can and can't tell you before a formal study.
Questions worth bringing to the appointment
Bring specifics. They help more than general impressions.
- Describe the night: Snoring, gasping, mouth breathing, sweating, bedwetting, unusual sleep positions.
- Describe the day: Irritability, hyperactivity, morning headaches, focus problems, learning changes.
- Describe the timeline: When did it start, and has it been getting worse?
- Describe prior treatment: Allergies, ENT visits, orthodontic concerns, surgery, or prior sleep testing.
A short phone video of your child sleeping can be useful. It gives the clinician a glimpse of what you're seeing at home.
If symptoms continue after surgery
This is an important issue that families don't hear enough about. Surgery can help many children, especially when enlarged tonsils and adenoids are a major contributor. But surgery does not guarantee that every child's sleep apnea is fully resolved.
The American Thoracic Society notes that some children, especially those with severe OSA or other risk factors, may still have persistent symptoms after adenotonsillectomy and should have a follow-up sleep study 2 to 3 months later, as explained in its patient guide to obstructive sleep apnea in children.
That follow-up matters. If a child still mouth breathes, snores, sleeps restlessly, or struggles during the day after surgery, don't assume the job is done.
Modern Treatment Options for Healthy Growth
Treatment should match the child, not just the diagnosis label. Some children need surgical care because enlarged tonsils and adenoids are the main obstruction. That can be the right step. But many children also benefit from a broader airway plan that looks beyond a single procedure.
What root-cause care tries to change
A root-cause approach focuses on the physical patterns that shape breathing over time:
- Nasal breathing: Restoring it whenever possible, because nasal breathing supports healthier airflow and oral posture.
- Tongue and facial muscle function: Orofacial myofunctional therapy can help retrain resting posture, swallowing patterns, and lip seal.
- Breathing mechanics: Buteyko-based breathing work may help children who habitually overbreathe through the mouth or struggle with nasal breathing habits.
- Jaw and airway support: In selected cases, custom oral appliances can support airway space and guide more favorable function during growth.
What tends to work better long term
The most durable plans are usually coordinated. They don't ask one tool to do everything. They combine the right referrals, the right timing, and the right follow-through. If a child has persistent mouth breathing after surgery, therapy focused on nasal breathing and oral posture may matter. If the jaw is narrow and the tongue has poor resting space, that structural issue shouldn't be ignored.
What usually works less well is waiting for a child to “mature out of” dysfunctional breathing patterns while symptoms continue. Habits get reinforced. Sleep stays fragmented. The child adapts, but not in a healthy way.
One practical treatment path
Parents looking for non-surgical options can explore pediatric sleep apnea treatment that includes airway-focused evaluation, myofunctional therapy, breathing retraining, and oral appliance options when appropriate. Pain and Sleep Therapy Center is one clinic that offers that type of care as part of a broader sleep and airway approach.
The hopeful part is this. Most families feel better once the problem has a name and a plan. A child who sleeps with less effort often functions like a different child during the day. Not because their personality changed, but because their body finally stopped fighting so hard every night.
If your child snores, mouth breathes, sleeps restlessly, wets the bed, or seems unusually irritable or unfocused during the day, it may be time to look at the airway more closely. Pain and Sleep Therapy Center provides evaluation and treatment for pediatric sleep-disordered breathing with an emphasis on root-cause care, including airway assessment, myofunctional therapy, breathing retraining, and other non-surgical options when appropriate.



