
You wake up after what should've been a full night of sleep, but your body feels like it never shut down. Your mind is slow. Coffee helps for an hour, then the fog returns. Maybe you snore. Maybe your partner has noticed pauses in your breathing. Maybe no one has noticed anything, and you're still dragging yourself through the day wondering why "sleep hygiene" tips haven't fixed it.
That pattern often points to a problem higher up than typically understood. Not motivation. Not laziness. Not a lack of discipline. The airway.
Dental sleep medicine sits at the intersection of dentistry, sleep medicine, and functional airway care. It isn't just about making a mouthguard. Done properly, it helps identify when the jaw, tongue, muscles of the mouth and throat, and nighttime breathing patterns are contributing to poor sleep. For many patients, that's the missing link between chronic fatigue and a treatment plan that finally makes sense.
The Unseen Cause of Your Chronic Fatigue
Many people who feel exhausted all day assume the problem must be stress, age, hormones, or bad sleep habits. Sometimes those factors matter. But when someone sleeps for what looks like enough hours and still wakes unrefreshed, I start thinking about whether airflow is breaking down during sleep.
That breakdown doesn't always look dramatic. It can show up as snoring, dry mouth, morning headaches, trouble focusing, irritability, jaw tension, or the sense that you never quite enter restorative sleep. If breathing is unstable all night, the body keeps shifting into a protective mode instead of settling into deep recovery.
Why the airway changes everything
Sleep isn't restorative just because you're in bed. It becomes restorative when breathing stays open and steady enough for the brain and body to cycle normally through sleep stages. If the tongue falls back, the lower jaw sits too far back, or the tissues in the throat become more collapsible, the result can be fragmented sleep even when the clock says you got enough hours.
That matters for people who are trying to troubleshoot fatigue at home. Bedroom setup can help comfort and positioning, and some patients benefit from elevating the upper body, so it can be useful to compare adjustable bed models if reflux, positional breathing issues, or nighttime congestion make lying flat harder. But furniture alone doesn't diagnose whether your airway is repeatedly narrowing or collapsing.
Poor sleep isn't always a sleep hygiene problem. Sometimes it's a breathing problem happening during sleep.
When fatigue deserves a sleep apnea conversation
If your fatigue comes with snoring, witnessed pauses, frequent waking, or morning brain fog, it's worth looking at the connection between chronic fatigue and sleep apnea. Patients often feel relieved when they learn there's a structural and functional reason they feel so depleted.
Dental sleep medicine exists for exactly this reason. It focuses on sleep-related breathing disorders through the lens of the mouth, jaw, tongue, and airway. That creates an important shift. Instead of asking only, "How can I sleep longer?" we ask, "What is happening to your breathing while you sleep, and how do we stabilize it safely?"
What Is Dental Sleep Medicine
Dental sleep medicine is a recognized interdisciplinary field. UTHealth Houston describes it as a specialized area of dentistry focused on oral appliance therapy for snoring and obstructive sleep apnea, with collaboration across ENT, neurology, pulmonary medicine, internal medicine, and psychiatry. The same institutional overview notes that only 45% of responding dental schools, 12 of 28, had a dental sleep medicine clinic, and about one-third reported difficulty integrating it into existing programs, which shows that advanced training and infrastructure remain uneven even as the field grows (UTHealth Houston dental sleep medicine overview).
A simple way to think about the role of a qualified dental sleep medicine provider is this: during sleep, the dentist isn't just looking at teeth. They're evaluating the traffic pattern of the airway. Jaw position, tongue posture, bite design, nasal breathing habits, and oral structures all influence whether airflow moves smoothly or keeps getting blocked.
More than a mouthguard
Patients often arrive expecting a single device and a simple handoff. That isn't what this field is. A trained provider has to understand facial anatomy, jaw mechanics, airway behavior during sleep, side effects that can develop over time, and how treatment fits into a medical diagnosis.
That last point matters. Snoring can be socially disruptive, but obstructive sleep apnea is a medical condition. If a provider skips the medical side and jumps straight to a device, the care is incomplete.
What qualified care includes
A real dental sleep medicine workup usually includes several layers:
- Airway-focused screening: Review of symptoms, sleep history, oral anatomy, jaw position, and risk factors for sleep-disordered breathing.
- Coordination with physicians: A sleep physician confirms the diagnosis and helps define medical severity and treatment priorities.
- Appliance planning and monitoring: If oral appliance therapy is appropriate, the dentist selects, fits, and adjusts the device over time.
- Functional support: In many cases, tongue posture, mouth breathing, and muscle dysfunction also need attention.
The product is the appliance. The discipline is the management of breathing during sleep.
This is why provider training matters so much. Plenty of dentists can fabricate a guard. Far fewer are trained to evaluate whether that guard is the right intervention, how to titrate it, when to combine it with other therapies, and how to coordinate long-term follow-up with the medical team.
The Diagnostic Journey What Patients Can Expect
Most confusion in this field starts with one basic question. Who diagnoses the problem?
The answer is straightforward. A dentist can screen for obstructive sleep apnea, but a physician must diagnose it. The American Academy of Dental Sleep Medicine states that the dentist then manages treatment as part of a collaborative team, including follow-up to make sure the oral appliance is effective and properly tracked over time (AADSM patient FAQ on dental sleep medicine).
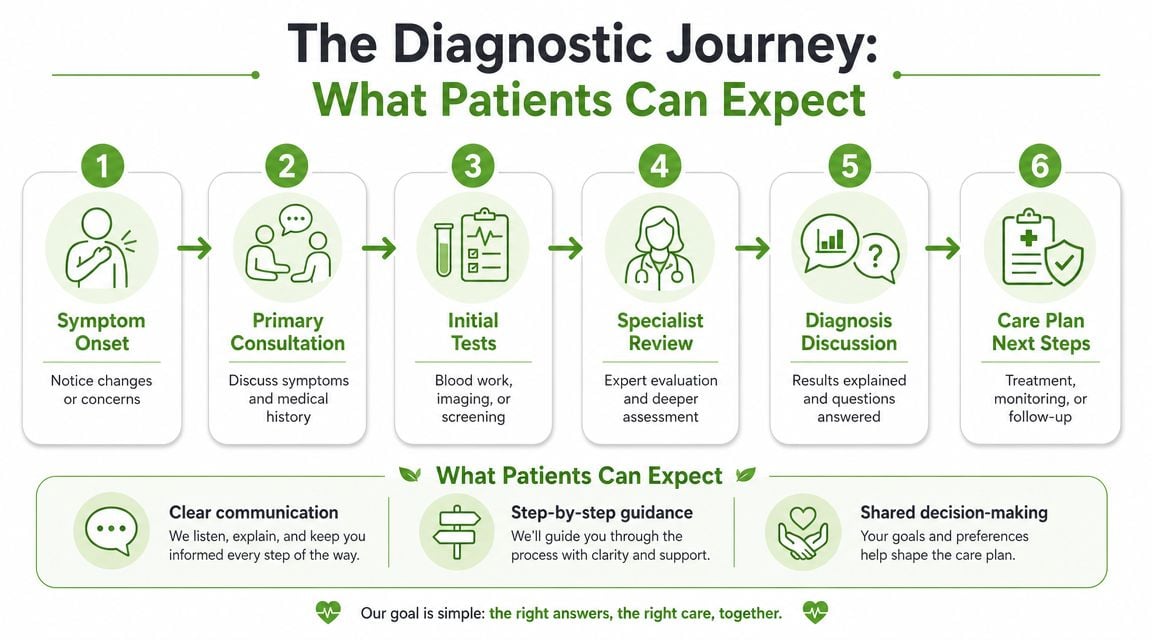
Step one starts in the dental chair
A dental office may be the first place someone hears that their airway could be part of the problem. The clues can include snoring, worn teeth, a narrow palate, scalloping of the tongue, dry mouth, or a history of waking unrefreshed. That screening is valuable, but it isn't the same as a diagnosis.
If symptoms suggest sleep-disordered breathing, the next move is medical testing. For patients trying to understand the basics, this guide on how to diagnose sleep apnea at home explains how home testing fits into the broader evaluation.
What the physician does
The sleep physician decides whether the pattern is consistent with obstructive sleep apnea or another sleep disorder. That may involve a home sleep study or an in-lab polysomnogram, depending on the clinical picture.
The physician's role is essential because not every sleepy patient has the same condition, and not every snorer has the same risk level. Some patients need broader medical workup. Others need treatment options compared against PAP therapy, positional interventions, or other medical strategies.
What happens after diagnosis
Once the diagnosis is confirmed and oral appliance therapy is selected, the dental sleep medicine provider takes over the mechanical side of treatment.
That usually means:
- Collecting detailed records so the appliance can be fabricated to fit the patient's bite and anatomy.
- Delivering a custom device and teaching the patient how to insert it, remove it, clean it, and adapt to it.
- Adjusting the position gradually so the jaw advances enough to help the airway without creating unnecessary jaw strain.
- Monitoring side effects and bite changes over time.
- Sending the patient back for follow-up testing to verify that treatment is working.
A device that feels fine but hasn't been objectively verified may still be undertreating the airway.
This is the part many introductory articles skip. The question isn't whether an appliance can be made. It's whether the treatment is being measured, coordinated, and refined with medical oversight.
Oral Appliance Therapy The Primary Treatment Tool
For many adults with obstructive sleep apnea, oral appliance therapy is the main tool dental sleep medicine uses. It is not a sports guard, not a night guard, and not a generic anti-snoring gadget. It is a medical treatment designed to improve airway stability during sleep.
According to guideline-based recommendations, oral appliance therapy is supported for adult obstructive sleep apnea when delivered by a trained dentist. In mild OSA, defined in the guideline as an apnea-hypopnea index of 5 to 15, it is considered an appropriate alternative to PAP. For moderate-to-severe disease, it is generally used as a second-line option when PAP is not tolerated or preferred. Its mechanism is specific: a custom titratable mandibular advancement device moves the mandible forward, enlarges the retroglossal airway, and can reduce airway collapsibility during sleep (AADSM special article on oral appliance therapy).

How the appliance actually works
A mandibular advancement device holds the lower jaw in a more forward position while you sleep. That forward positioning changes the relationship between the tongue, lower jaw, and throat space. In the right patient, it helps keep the airway from narrowing as muscles relax overnight.
The key word is titratable. The device needs adjustability because there is a balance to strike. Too little advancement may leave the airway unstable. Too much may aggravate the jaw joints, muscles, or teeth.
What works and what doesn't
The biggest mistake patients make is assuming all oral appliances are equivalent. They aren't.
| Option | What it does well | Main limitation |
|---|---|---|
| Custom titratable appliance | Fits the bite precisely and can be adjusted over time | Requires professional fitting and follow-up |
| Over-the-counter boil-and-bite device | Easy to buy | Often bulky, imprecise, and not designed for proper medical titration |
| Night guard not intended for OSA | May protect teeth from grinding | Doesn't reliably address airway collapse |
A few practical points matter here:
- Custom fit matters: A poorly fitting device can loosen, feel intolerable, or shift forces onto the wrong teeth.
- Adjustment matters: The first setting usually isn't the final one.
- Follow-up matters: Success depends on symptom response, side-effect management, and objective sleep testing, not just whether snoring gets quieter.
For patients weighing different treatments, this comparison of sleep apnea oral appliance vs CPAP is useful because it frames the decision around tolerance, anatomy, and treatment goals rather than brand loyalty.
Side effects are manageable, but they are real
Most side effects are mechanical, not mysterious. Some patients notice temporary tooth tenderness, jaw soreness, salivation changes, or a bite that feels different in the morning. Long-term occlusal changes can occur, which is why ongoing review is part of proper care.
Practical rule: If a provider offers an appliance without a plan for calibration and long-term follow-up, that's incomplete treatment.
Done properly, oral appliance therapy can be elegant. Done casually, it can become a frustrating gadget that never reaches therapeutic benefit.
Beyond the Appliance Integrated Root Cause Therapies
A common scenario looks like this. A patient starts using an oral appliance, the snoring drops, and the sleep study looks better. Yet they still wake tired, keep their lips apart during the day, or fall back into mouth breathing at night. That is a gap we often see patients run into, and it usually points to function, not just anatomy.
Dental sleep medicine works best as the hub of a coordinated plan. The appliance creates airway support during sleep, but lasting improvement often depends on what the tongue, lips, nasal airway, head posture, and breathing pattern are doing the other 23 hours of the day.

Practical Neurology describes the same shift many of us see clinically. Care is becoming more individualized and often combines oral appliance therapy with other strategies, including positional therapy, with follow-up sleep testing used to confirm benefit (Practical Neurology on dental sleep medicine).
Why function matters
Airway collapse rarely has a single cause. Low tongue posture, poor lip seal, oral resting posture, nasal obstruction, swallowing mechanics, and upper chest breathing can all make a vulnerable airway less stable during sleep.
Patients and referring doctors sometimes miss the bigger picture. A well-made appliance can hold the jaw in a better position and still leave the patient with persistent mouth breathing, poor nasal use, or weak oral muscle patterns.
Orofacial myofunctional therapy addresses those patterns directly. It trains tongue posture, lip competence, swallowing coordination, and nasal breathing habits. In the right patient, that work supports the appliance instead of competing with it.
Breathing retraining, including Buteyko-based approaches for selected patients, can also help. Someone who chronically breathes through the mouth, over-breathes, or uses the neck and chest excessively to breathe may need coaching, not just hardware.
How integrated care looks in practice
The treatment plan should fit the person in front of you.
- If body position worsens events: Side-sleeping strategies or head-of-bed elevation may reduce airway narrowing for some patients. For people reviewing comfort options at home, Woodstock Furniture & Mattress Outlet adjustable bases can be one practical resource to consider alongside medical guidance.
- If oral muscle function is part of the problem: Myofunctional therapy may help reinforce lip seal, tongue-to-palate posture, and more efficient swallowing.
- If breathing habits are driving symptoms: Breathing retraining can support nasal breathing and reduce habitual mouth breathing.
- If the case is medically layered: Pain and Sleep Therapy Center may combine dental sleep medicine, myofunctional therapy, breathing work, and physician collaboration within one coordinated plan.
That team-based model matters. Sleep physicians diagnose and help define severity. Dentists provide appliance design, fit, titration, and dental monitoring. Myofunctional therapists and breathing specialists address the habits and muscle patterns that can limit long-term success if they are ignored.
What this approach does better
The appliance creates space. Functional therapy helps the patient hold and use that space more effectively.
I often explain the trade-off this way. If treatment focuses only on jaw advancement, the airway may improve while poor oral posture and mouth breathing continue. If treatment focuses only on exercises in a patient with a clearly collapsible airway, progress can be slow and incomplete.
The strongest plans match the mechanical treatment to the functional problem. That is how dental sleep medicine becomes more than a mouthguard. It becomes the center of a care team built to improve breathing, sleep quality, and long-term stability.
Choosing Your Qualified Dental Sleep Medicine Provider
Finding the right provider matters as much as choosing the right treatment. A general dentist may be excellent at restorative care and still have limited training in airway management, sleep-disordered breathing, and long-term appliance titration.
When you're evaluating a provider, focus less on whether they "offer sleep appliances" and more on how they practice dental sleep medicine.
What to look for
A strong provider usually has several features in place:
- Advanced training: Look for formal education in dental sleep medicine, not just a weekend course.
- Board certification or recognized credentials: Credentials signal that the provider has gone beyond entry-level exposure.
- Physician collaboration: Ask whether the office routinely works with sleep physicians, ENTs, neurologists, and primary care doctors.
- A follow-up protocol: The office should have a clear plan for titration, side-effect review, and objective verification after delivery.
- Comfort with combination care: The provider should understand when an appliance needs to be paired with positional care, myofunctional therapy, or other support.
Questions worth asking
Ask direct questions. The answers tell you a lot.
- Who diagnoses obstructive sleep apnea in your process?
- Do you use custom titratable appliances, and how do you adjust them over time?
- How do you confirm that treatment is working after the appliance is delivered?
- What do you do if the patient develops jaw pain, bite changes, or poor tolerance?
- Do you coordinate with the referring physician and send follow-up reports?
A practical point for both patients and referring offices is insurance workflow. Dental sleep medicine often sits at the boundary of dental and medical systems, which can create billing confusion. Teams trying to understand that side of practice operations may find it useful to review how AI-powered dental billing solutions are being applied to specialty dental claims and coordination processes.
A simple standard
If the conversation starts and ends with "We can make you a device," keep looking.
If the conversation includes diagnosis, medical partnership, custom treatment design, side-effect management, and objective follow-up, you're much closer to the standard this field requires.
Frequently Asked Questions About Treatment and Outcomes
Is oral appliance therapy covered by insurance
It may be, but coverage often depends on diagnosis, documentation, and whether the claim is handled through medical insurance rather than a routine dental benefit. This is one reason coordinated offices are helpful. They understand that sleep apnea treatment doesn't fit neatly into a standard dental box.
How long does it take to get used to an appliance
Adaptation varies. Some patients adjust quickly. Others need time, small titration changes, morning bite exercises, or additional support if jaw muscles are sensitive. A slower start doesn't mean failure. It usually means the device needs to be managed thoughtfully.
What side effects should I expect
Common issues include temporary soreness, tooth pressure, excess saliva or dryness, and a bite that feels "off" in the morning. Those effects are part of why follow-up matters. A properly managed appliance is not a set-it-and-forget-it treatment.
Can dental sleep medicine cure sleep apnea
Sometimes symptoms improve dramatically, but the safer question is whether treatment is controlling the condition. In many adults, dental sleep medicine is a highly useful management strategy rather than a one-time cure. That is especially true when the airway problem involves anatomy, weight, nasal issues, sleep position, and functional habits all at once.
Why is this field getting so much attention now
Because it is becoming a more central access point for care. The U.S. dental sleep medicine market was estimated at USD 1.10 billion in 2024 and is projected to reach USD 2.20 billion by 2035, implying roughly 6.5% annual growth over the 2025 to 2035 period. That same market analysis identifies oral appliances as the largest segment and points to the growing integration of sleep medicine into dental practices (U.S. dental sleep medicine market analysis).
The increase in visibility is useful, but patients should still be selective. Growth in the field doesn't replace the need for proper diagnosis, multidisciplinary care, and follow-up that proves the treatment is working.
If you're dealing with snoring, daytime fatigue, jaw tension, or diagnosed sleep apnea and want a more complete plan than "just wear this device," Pain and Sleep Therapy Center offers evaluation and treatment for sleep-related breathing problems with a focus on dental sleep medicine, physician collaboration, myofunctional therapy, and breathing-based care.



