
You wake up tired, push through coffee, answer emails, sit in MoPac traffic, and tell yourself you're just busy. By midafternoon, your concentration slips. At night, your partner complains about snoring or says you seem to stop breathing. A lot of adults in Austin live in that loop for years before they realize it may be obstructive sleep apnea, not just stress or poor sleep habits.
That matters because the right treatment can change much more than your nights. Better sleep can improve daytime alertness, reduce strain on your heart and blood pressure, and make work, driving, exercise, and family life feel manageable again. The good news is that sleep apnea treatment in Austin has expanded well beyond “just use CPAP,” and patients now have more than one realistic path.
Tired of Being Tired in Austin
A common Austin story goes like this. Someone in their 30s, 40s, or 50s starts falling asleep during movies, needs more caffeine than before, and feels oddly irritable despite getting what looks like enough time in bed. Their smartwatch may show fragmented sleep. Their partner notices loud snoring first.
Then the pattern gets harder to ignore. Morning headaches show up. Meetings feel foggy. Weekend sleep doesn't fix anything. If that sounds familiar, it's worth comparing your symptoms with common signs and symptoms of sleep apnea.
What makes this tricky is that sleep apnea rarely announces itself as one dramatic event. It often looks like normal life going slightly off track. People blame age, work stress, weight gain, allergies, or parenting. Sometimes all of those are present, but they still don't explain repeated breathing disruptions at night.
Sleep apnea can be serious and still be very treatable. Those two things are both true.
In Austin, patients usually don't need a heroic plan to get started. They need a clear one. First, confirm whether sleep apnea is present. Then match treatment to severity, airway anatomy, comfort, and what you can realistically stick with long term. That's where many online guides fall short. They list devices, but they don't help you choose.
The First Step Getting a Diagnosis in Austin
Patients often enter the system through a primary care visit, a cardiology referral, or an ENT consultation. The trigger is usually a cluster of symptoms: snoring, witnessed pauses in breathing, morning headaches, daytime sleepiness, poor focus, or unrestful sleep. If you already have high blood pressure, your doctor may be even more alert to the possibility that sleep-disordered breathing is part of the picture.
Home testing versus lab testing
In Austin-area sleep apnea care, home sleep testing is commonly used first because portable devices can measure breathing in your own bed, while in-lab polysomnography still matters when clinicians need more detailed physiologic data or when results are unclear, as described by Austin Regional Clinic's sleep apnea overview.
Home testing is often a practical starting point. It's familiar, convenient, and often faster to arrange. For many adults with straightforward symptoms of obstructive sleep apnea, it's enough to identify whether breathing events are happening often enough to require treatment.
Lab testing does more. It's typically chosen when the history is more complicated, the home test doesn't answer the key question, or your clinician needs a broader picture of what's happening during sleep. That may include cases where symptoms and home results don't line up well.
If you're wondering what at-home evaluation usually involves, this guide to how to diagnose sleep apnea at home gives a useful patient-level overview.
What the diagnosis is really for
The sleep study isn't just paperwork to “qualify” you for a machine. It helps your clinician decide which treatment category fits. The core issue in obstructive sleep apnea is recurrent upper-airway collapse during sleep, so the important question is not just whether you snore. It's how often the airway collapses, how severe the problem is, and whether the data point toward CPAP, an oral appliance, Inspire, surgery, or another approach.
A practical diagnosis visit usually includes:
- Symptom review: Snoring, sleepiness, headaches, dry mouth, and partner observations.
- Medical context: Blood pressure, weight history, nasal obstruction, jaw structure, and prior treatment attempts.
- Treatment readiness: Whether you'd realistically use a mask, prefer a dental option, travel often, or want to avoid surgery if possible.
Practical rule: A good sleep apnea workup doesn't stop at “yes or no.” It identifies the kind of patient you are, because that's what drives the treatment choice.
Why Prioritizing Treatment Matters for Your Health
Treating sleep apnea isn't only about quieting a bedroom. It's about reducing repeated stress on the body. When breathing keeps narrowing or stopping during sleep, oxygen levels and sleep quality are disrupted over and over again. Patients often feel that as fatigue first. The cardiovascular system often feels it too.

The heart and blood pressure connection
Austin Heart notes that in patients with obstructive sleep apnea, treatment can lower blood pressure by 10 or more points, and the program also states it is the only program in Central Texas integrating cardiac and sleep-disorder care on the same platform, according to Austin Heart's sleep disorders program page.
That's not a small issue. If sleep apnea is contributing to stubborn hypertension, treating the airway problem can become part of cardiovascular care, not a side topic. This is one reason cardiologists, primary care physicians, sleep physicians, and ENTs increasingly overlap in how they manage these patients.
Why symptoms can fool you
Many adults assume they'd know if something serious were happening at night. They usually don't. Sleep apnea often builds gradually. Some patients never notice dramatic choking awakenings. They just become a lighter, less restorative sleeper and a more exhausted daytime version of themselves.
That's why I often tell patients to think about untreated sleep apnea as a mechanical problem with body-wide consequences. The airway keeps failing when it should stay open. The result isn't just noise. It's repeated physiologic strain.
A short explainer can help make that connection clearer:
The real goal of treatment
Patients often arrive focused on one symptom. Their partner wants the snoring to stop. They want more energy. Their doctor wants better blood pressure control. All of those are valid reasons to treat.
The important shift is this: sleep apnea treatment in Austin should be viewed as protective care, not just comfort care. When treatment works and the patient uses it consistently, the payoff reaches well beyond bedtime.
A Guide to Sleep Apnea Treatment Options
Once a sleep study confirms apnea, treatment becomes a matching problem. The best option depends on what is collapsing, how severe the obstruction is, what you are likely to use consistently, and what your insurance will cover in Austin. A treatment that looks strong on paper can still fail if it does not fit your anatomy or your routine.
CPAP and related PAP therapy
CPAP is still the starting point for many adults with obstructive sleep apnea, especially in moderate to severe cases. It uses pressurized air to hold the airway open during sleep. For many patients, it works well because it treats the airway directly and can be adjusted with different masks, pressure settings, humidification, and follow-up support.
Best fit:
- Moderate to severe OSA in many cases
- Patients who want a non-surgical first-line option
- People willing to work through mask fitting and adjustment
Pros:
- Strong first-line role in established care
- Non-surgical
- Adjustable for comfort and effectiveness
Cons:
- Mask fit, dry air, pressure discomfort, or claustrophobia can limit use
- A technically effective device does not help much if it stays on the nightstand
Oral appliance therapy
Oral appliances move the lower jaw forward to reduce airway collapse during sleep. In the right patient, this is a legitimate treatment option, not a backup plan. It is often a reasonable choice for mild to moderate OSA, and it can also help selected patients with more severe disease who cannot use CPAP.
If you are weighing the two most common non-surgical options, this comparison of sleep apnea oral appliance vs CPAP is useful because comfort, fit, and long-term use often matter as much as the device category.
Best fit:
- Patients who cannot tolerate CPAP
- Mild to moderate OSA in many cases
- People who want a smaller, travel-friendly device
Pros:
- Compact and portable
- Often easier for travel and shared sleeping spaces
- Better tolerated by some patients who struggle with masks
Cons:
- Not effective for every airway pattern or severity level
- Requires a proper dental sleep medicine fitting and follow-up adjustments
- Can cause jaw discomfort, bite changes, or dental side effects in some patients
Inspire hypoglossal nerve stimulation
Inspire is an implantable treatment for selected adults with obstructive sleep apnea who cannot use CPAP. It stimulates the nerve that helps keep the airway open during sleep. This is not a shortcut around the usual workup. It requires careful screening, including severity review, body weight criteria, and an airway exam to see whether the collapse pattern is a good fit.
Austin ENT describes Inspire as an outpatient surgical option for adults with moderate to severe OSA who meet candidacy requirements and cannot tolerate CPAP, with patient-reported benefits that include less snoring and high satisfaction on longer-term follow-up, according to Austin ENT's sleep apnea treatment page.
Best fit:
- Selected adults with moderate to severe OSA
- Patients who cannot use CPAP
- People who meet anatomy and candidacy requirements
Pros:
- No nightly mask
- Appeals to patients who want a device-free bedtime routine
- Outpatient procedure in many cases
Cons:
- Requires surgery
- Not every patient qualifies
- Approval often depends on both medical criteria and insurance review
Surgery and anatomy-focused care
Surgery can help when a specific structural problem is driving the obstruction. That might involve the nose, soft palate, tonsils, tongue base, or a more complex airway pattern. One operation does not fit every patient.
I encourage patients to slow down and ask a focused question: what exactly is the procedure trying to fix? A nasal procedure may improve breathing and make CPAP easier to use, but it usually does not cure moderate or severe OSA by itself. Palate or tongue-base surgery may help selected patients, but results depend heavily on the pattern of collapse seen on exam.
Best fit:
- Patients with a clear anatomic contributor to obstruction
- People who have failed or declined non-surgical treatment
- Patients who need surgery as part of a combination plan
Pros:
- Can address a structural problem directly
- May improve tolerance of CPAP or oral appliance therapy
- Sometimes part of a successful multi-step treatment plan
Cons:
- Recovery time varies
- Outcome depends on choosing the right procedure for the right anatomy
- Surgery can improve apnea without eliminating it completely
Lifestyle and medical therapy
Lifestyle measures matter, but they need to be matched to the case in front of you. Weight reduction, positional therapy, reducing alcohol near bedtime, and treating nasal obstruction can all improve airway stability. For some patients with mild disease, those steps may meaningfully reduce symptoms. For many others, they work best alongside CPAP, an oral appliance, or another primary treatment.
Medical therapy is also getting more attention than it used to. SleepDoc notes that treatment discussions now may include obesity-directed medication for adults with moderate to severe OSA and obesity, including tirzepatide after FDA approval in this setting, according to SleepDoc's sleep apnea services page. That does not replace a sleep study or device-based therapy when one is needed, but it can change the treatment plan for the right patient.
Pain and Sleep Therapy Center also offers evaluation and treatment related to sleep-disordered breathing and apnea as part of a broader airway-focused practice.
Sleep Apnea Treatment Options at a Glance
| Treatment | How It Works | Best For | Key Pro | Key Con |
|---|---|---|---|---|
| CPAP | Uses pressurized air to keep the airway open | Many patients, especially moderate to severe cases | Strong first-line role | Some patients cannot tolerate it |
| Oral appliance | Holds the jaw forward to reduce airway collapse | Mild to moderate OSA, or CPAP-intolerant patients | Smaller and easier to travel with | Not ideal for every severity or anatomy |
| Inspire | Stimulates airway muscles through an implantable system | Selected adults with moderate to severe OSA who cannot use CPAP | No mask at night | Requires surgery and candidacy screening |
| Surgery | Targets anatomic obstruction | Patients with specific airway findings | Can address structural contributors | Outcome depends heavily on the exact anatomy |
| Lifestyle and medical therapy | Addresses contributing factors such as obesity or position | Selected patients, often as part of combination care | Can complement device-based care | Often not enough as a stand-alone treatment |
How to Choose the Right Treatment Path for You
The best treatment is rarely the one with the most advertising. It's the one that fits your diagnosis and your life well enough that you'll keep using it.
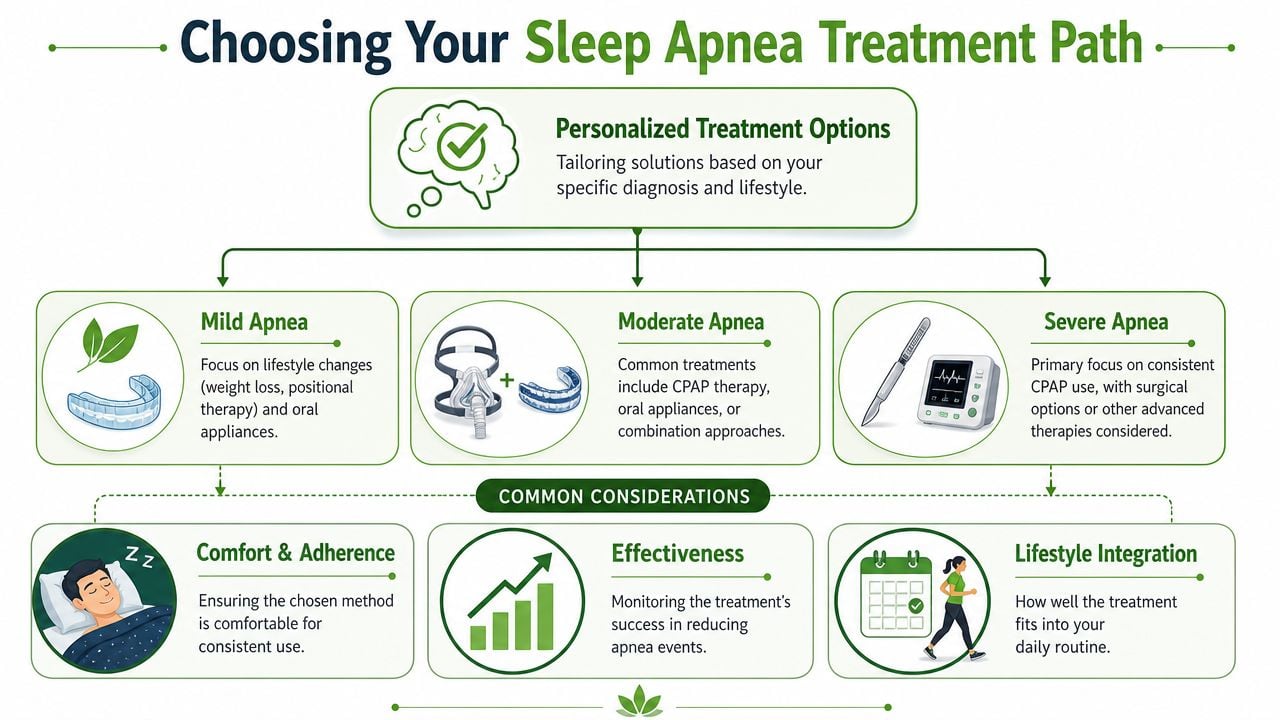
Start with severity, then narrow further
Clinical guidance in Austin consistently points to one central principle: treatment should match severity and anatomy, not just convenience. Capital ENT notes that oral appliances are typically used for people who can't tolerate CPAP or prefer an alternative, while hypoglossal nerve stimulation is generally reserved for a select group with moderate-to-severe OSA who cannot use CPAP, and that consistent adherence drives outcomes.
Severity gives the first layer of direction. A patient with mild disease and favorable anatomy may have several reasonable options. A patient with severe OSA usually needs a more reliable airway-stabilizing strategy from the start. But severity alone still doesn't settle the decision.
The questions that matter in real life
These are the questions I'd want answered before calling any treatment “right”:
- How severe is the obstruction? Your sleep study determines the starting point.
- What does your airway anatomy look like? Jaw position, tongue base, nasal resistance, and soft tissue crowding all matter.
- What have you already tried? A patient who failed CPAP needs a different plan than one who never had proper fitting or support.
- What can you use consistently? A treatment only works when it's used.
- Does your BMI affect candidacy? It can matter, especially for advanced options like Inspire.
- What does your day-to-day life require? Frequent travel, shift work, claustrophobia, or dental limitations can all shape the decision.
The “best” therapy on paper can become the wrong therapy if the patient won't wear it.
A practical decision framework
If you're sitting with new test results and trying to sort out sleep apnea treatment in Austin, use this sequence:
- Confirm the diagnosis clearly. Don't move forward on symptoms alone.
- Ask what your clinician considers first-line for your severity. That establishes the medical baseline.
- Identify barriers early. Mask intolerance, jaw issues, nasal blockage, and travel needs should come up immediately.
- Discuss alternatives only after the basics are honest. Some patients were told they “failed CPAP” when they had poor coaching, bad mask fit, or no follow-up.
- Measure success by adherence and results together. Comfort without effectiveness isn't enough. Effectiveness without consistent use isn't enough either.
What doesn't work well
Patients lose time when they choose based on convenience alone, or when they chase a single treatment category before understanding their own phenotype. A small device isn't automatically better than CPAP. Surgery isn't automatically stronger than a device. Inspire isn't a universal replacement for masks.
The right frame is narrower and more useful. Which option is most likely to control your apnea, fit your anatomy, and remain realistic for the next several years?
Navigating Insurance and Costs in Central Texas
A common Austin scenario goes like this. A patient is ready to treat sleep apnea, then the first estimate arrives and the process suddenly feels harder than the diagnosis. That reaction makes sense. Sleep apnea care often involves several moving parts, and the cost depends as much on the treatment path as the treatment itself.

One patient may only need a home sleep test, a CPAP setup, and routine follow-up. Another may need imaging, ENT evaluation, oral appliance fitting, or review for Inspire or surgery. Each step can involve a different bill from a clinic, sleep lab, DME supplier, dentist, surgery center, or insurer.
The practical question is not only, “What does this cost?” It is, “What will my insurance cover for my diagnosis, and what documentation does that option require?”
What to verify before you agree to anything
The biggest financial mistakes usually happen early. A device gets ordered through an out-of-network supplier. A study is done before prior authorization is confirmed. A patient agrees to an oral appliance or implant consultation without understanding what the plan requires first.
Ask these questions before anything is scheduled or shipped:
- Who is in network? Confirm the sleep clinic, interpreting physician, ENT, dentist, surgeon, hospital or surgery center, and DME supplier.
- What needs prior authorization? This may apply to the sleep study, CPAP, oral appliance therapy, surgery, or Inspire evaluation and implantation.
- How is the equipment billed? Some plans rent CPAP first and convert to purchase later. Others apply different rules.
- What follow-up is covered? Mask refits, compliance visits, pressure changes, appliance adjustments, and post-op visits are not always handled the same way.
- What is my real out-of-pocket cost? Ask about deductible, copay, coinsurance, and whether a separate specialist bill is likely.
How costs differ by treatment path
This is where choice matters in a very practical way. CPAP is often the most straightforward option for insurance approval, especially for moderate to severe obstructive sleep apnea. It can still become expensive if the wrong supplier is used, compliance rules are missed, or replacement supplies are not covered the way the patient expected.
Oral appliance therapy can be a strong option for selected patients, but coverage varies more. Some medical plans cover it under durable medical equipment or medical benefits. Some plans push more of the cost to the patient. Dental and medical billing do not always line up neatly, which is why patients should ask who submits the claim and what records are needed.
Inspire and other surgical approaches usually require more documentation. In my experience, patients do better when they expect a review process rather than a quick approval. Insurers often want proof of diagnosis details, severity, body habitus criteria, and prior CPAP use or intolerance before they approve an implantable therapy.
Medical therapy can also affect cost planning. If weight is a meaningful driver of airway obstruction, a clinician may discuss weight-loss treatment as part of the plan. Some insurance plans cover those medications narrowly. Others exclude them. That does not make the conversation less important. It means the patient should separate medical appropriateness from insurance generosity and discuss both.
Bring your insurance card, medication list, and any prior sleep study reports to the treatment-planning visit. That often prevents repeat testing and delays.
Questions worth asking the office staff
Office staff hear these questions every day. Patients should ask them plainly.
- “Will you verify my benefits before I commit?”
- “Does my plan require that I try CPAP first?”
- “Which supplier will provide the device, and are they in network?”
- “If this option is denied, do you help with appeals?”
- “Do you offer payment plans for costs insurance does not cover?”
One more point matters. The cheapest option up front is not always the lowest-cost choice over time. A treatment that you can use consistently, that controls the apnea, and that does not create repeated restart costs is usually the better value. Financial planning should support that decision, not distort it.
Your Next Steps Toward Better Sleep in Austin
If you suspect sleep apnea, don't wait for the problem to become unbearable before acting. The hardest part is usually not treatment. It's getting from vague suspicion to a real diagnosis and a plan that fits.
Use this checklist:
- Write down your symptoms. Include snoring, morning headaches, fatigue, dry mouth, witnessed pauses, and any blood pressure concerns.
- Ask your bed partner what they've noticed. Their observations often fill in the gaps you can't see while asleep.
- Schedule a visit with your primary care doctor, ENT, or sleep specialist. Bring your symptom list and ask whether a sleep study is appropriate.
- Get the right test. Home testing is often a practical first step, but some patients need an in-lab study.
- Review the results with treatment in mind. Don't stop at “you have sleep apnea.” Ask which options match your severity, anatomy, and tolerance.
- Check insurance before committing. Confirm coverage, pre-authorization, and supplier details.
- Choose the treatment you can live with. Long-term use matters more than a perfect-sounding plan that sits in a drawer.
Sleep apnea treatment in Austin is no longer limited to one pathway. CPAP still helps many patients. Oral appliances help some. Inspire fits a narrower group. Surgery and medical therapy have a place too. The key is matching the treatment to the person.
If you're exploring non-surgical or airway-focused care for snoring, obstructive sleep apnea, jaw-related issues, or facial pain, Pain and Sleep Therapy Center offers evaluation and treatment for sleep-disordered breathing as part of its broader specialty practice. It can be one option to consider if you want a more detailed look at oral appliance therapy, TMJ-related airway factors, and personalized sleep support.



