
You crawl into bed early because you're exhausted. Then your mind wakes up. You watch the clock, shift pillows, rehearse tomorrow's problems, and tell yourself you must sleep now. Hours later, you're still trying. The next day feels foggy, short-tempered, and strangely lonely because insomnia can make the whole world feel harder.
If that sounds familiar, you're not failing at sleep. You're probably stuck in a pattern that rewards effort in all the wrong ways. Many people with insomnia spend more and more time in bed hoping extra opportunity will produce extra sleep. Often, it does the opposite. Bed becomes the place where you worry, monitor, and struggle.
That's where sleep restriction therapy can help. It's a structured behavioral treatment used within CBT-I, and it asks you to do something that sounds backwards at first. You spend less time in bed so your sleep becomes more solid, more efficient, and more predictable. It isn't about punishing yourself or forcing deprivation. It's about retraining a sleep system that has gotten confused.
Struggling with Insomnia It's Time to Reclaim Your Nights
A common insomnia story goes like this. You go to bed at a reasonable hour because you want to “catch up.” You lie there awake. You finally drift off, wake again, check the time, and start calculating how ruined tomorrow will be. By morning, you've been in bed a long time but slept very little.
That pattern teaches the brain a painful lesson. Bed starts to mean frustration instead of sleep. The harder you try, the more alert you become.
Why basic advice often isn't enough
People often start with caffeine rules, blackout curtains, white noise, or articles about improving your sleep quality. Those can help at the edges. They usually don't fix chronic insomnia by themselves because the core problem is often a mismatch between time in bed and actual sleep ability.
If you've already tried routine changes, breathing exercises, or a calmer bedroom setup, it may help to look at a more structured behavioral approach such as natural ways to improve sleep quality that fit into a broader insomnia plan.
Sleep restriction therapy changes the goal from “try harder to sleep” to “create the conditions in which sleep happens again.”
A different way to think about treatment
The word “restriction” scares many people. Fair enough. Most hear it and assume it means getting less sleep on purpose. In practice, the target is different. You're reducing time in bed, especially the hours you spend awake and frustrated, so sleep becomes compressed into a tighter and more reliable window.
That's why many sleep clinicians describe it as retraining rather than forcing. You stop negotiating with the night. You use a schedule, a diary, and a set of adjustment rules. Over time, that consistency helps rebuild trust in your body's ability to sleep.
How Sleep Restriction Therapy Retrains Your Sleep System

Sleep restriction therapy works best when you understand two systems. One is sleep pressure. The other is your circadian rhythm, which is your internal body clock.
Think of sleep pressure like a tank that fills while you're awake. The longer you stay awake, the fuller that tank gets. If you get into bed too early, nap late, or spend long stretches half-awake in bed, the tank may not be full enough when you want sleep to happen.
The sleep pressure tank
With insomnia, people often do reasonable things that accidentally weaken sleep pressure. They go to bed early after a bad night. They sleep in when they can. They rest in bed because they feel worn down. Each move makes sense in the moment. Together, they can keep sleep fragmented.
Sleep restriction therapy tightens the sleep window so the body builds a stronger drive for sleep. The treatment is designed to strengthen homeostatic sleep pressure and reduce conditioned wakefulness by compressing time in bed. Clinical evidence suggests measurable improvements, including about a 12-minute reduction in sleep latency and a 5% to 10% increase in time asleep while in bed, as described in this clinical review of sleep restriction therapy.
Your internal clock still matters
The second system is your circadian rhythm. That's the timing system that influences when your body feels ready for sleep and ready for wakefulness. Sleep restriction therapy doesn't replace the body clock. It works with it by giving sleep a consistent place to land.
If your wake time changes constantly, your brain gets mixed signals. If your bed becomes a place for worrying, scrolling, watching shows, or trying very hard to sleep, your brain also learns that bed is a place for wakefulness. SRT tries to reverse that learning.
Here's the plain-language version:
- Less drifting in and out of bed: Your body gets one clear sleep window.
- More built-up sleep drive: You're sleepier when bedtime arrives.
- Stronger bed-sleep connection: Bed stops being a battleground.
- Better consolidation: Sleep becomes less scattered.
Practical rule: SRT is not “stay up forever and hope for the best.” It's a measured way to line up sleep pressure, body clock timing, and bed association.
Why it feels backwards
People get confused because “spend less time in bed” sounds like advice for making insomnia worse. But insomnia is not limited to a shortage of hours in bed. It's often a shortage of sleep that happens efficiently within those hours.
That's why a shorter, more realistic sleep window can outperform a long, hopeful one. You're not shrinking your chance to sleep. You're removing the hours that have turned into wakeful struggle.
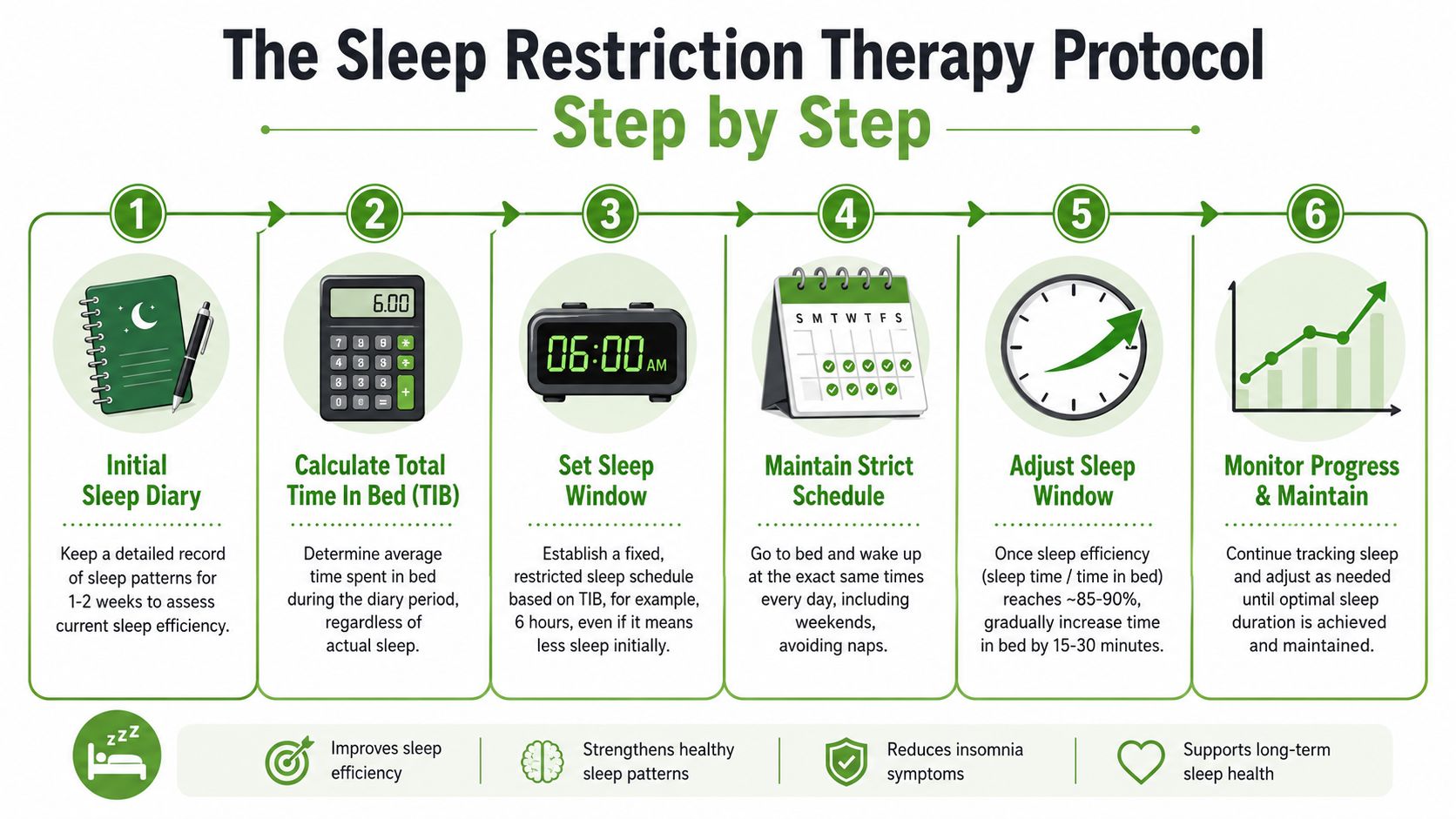
The Sleep Restriction Therapy Protocol Step by Step
You have been exhausted for weeks, so going to bed later can sound wrong at first. Yet that is often how sleep restriction therapy begins. The method is structured, data-based, and a little uncomfortable by design.
Before starting, it helps to use a formal sleep quality assessment if you are not sure insomnia is the full picture. Snoring, restless legs, circadian problems, pain flares, and medication effects can all change what is safe or useful. That is one reason SRT is sometimes started with professional guidance, especially for people with more than one sleep or health issue.
Step 1 and Step 2
Start with a sleep diary for 1 to 2 weeks. Write down when you got into bed, how long it seemed to take to fall asleep, how often you woke up, how long you were awake, and when you got up for the day. The goal is to estimate your average total sleep time. That number matters more than the time you hoped to be asleep.
Then pick a fixed wake-up time that you can keep every day, including weekends. In SRT, wake time is the anchor. Bedtime is calculated from it, not chosen by fatigue or frustration on a given night.
This can feel strict. It is. A shifting wake time is like resetting a clock every morning and expecting it to keep accurate time.
Step 3 and Step 4
Next, set your initial sleep window based on your recent average sleep time. Many protocols also set a lower limit so the window does not become too short. If your sleep diary suggests you are sleeping about 6 hours per night, your first schedule may allow 6 hours in bed.
Here is a practical example. If your fixed wake time is 6:30 a.m. and your starting sleep window is 6 hours, your target bedtime becomes 12:30 a.m. The late bedtime often surprises people, but the logic is simple. You are trying to match time in bed to the amount of sleep your body is producing right now, not the amount you wish it were producing.
For some people, a gentler version called sleep compression is a better place to begin. Instead of cutting time in bed quickly, sleep compression reduces it more gradually over time. That approach may fit better if you are older, already very sleepy during the day, living with chronic pain, or worried that a sudden schedule change could make you unsafe.
Step 5 with a simple example
Now you track sleep efficiency, which means total sleep time divided by total time in bed. It is a way of asking, “How much of this sleep window is being used for sleep?”
A simple example helps. If you sleep 5 hours and 15 minutes during a 6-hour sleep window, your efficiency is high. If you spend large parts of that window awake, your efficiency is lower. Each week, the schedule is adjusted based on that pattern, usually in small increments such as 15 to 30 minutes.
A practical version looks like this:
| Situation | What it means | Typical adjustment |
|---|---|---|
| Efficiency is 85% or higher | You are sleeping through most of the window | Add 15 to 30 minutes to time in bed |
| Efficiency is below 80% | Too much of the window is still awake time | Reduce time in bed by 15 to 30 minutes |
| In between | The schedule may be close, but not stable yet | Often keep the same window and keep tracking |
This weekly adjustment is the part people often want to rush. Try not to. SRT works more like tuning an instrument than flipping a switch. Small changes give you clearer feedback.
Step 6 and the part people underestimate
The hardest part is following the plan on rough nights.
- Keep the wake time fixed: Get up at the scheduled time, even after a poor night.
- Avoid sleeping in: Extra morning sleep can weaken the sleep pressure you are trying to build.
- Track the pattern: Imperfect diary entries are still useful. Missing several days makes decisions much harder.
- Watch daytime safety: If you feel too sleepy to drive, work safely, or think clearly, the schedule may be too aggressive.
- Get help if other conditions are involved: SRT can be harder and sometimes riskier when insomnia overlaps with bipolar disorder, seizures, untreated sleep apnea, chronic pain, heavy sedating medications, or fall risk.
If you wake at 3 a.m., do not redesign the plan in the dark. Log what happened. Follow the schedule the next morning. Review the whole week before making changes.
That balance matters. SRT can be very effective, but it is not the right starting point for every person. If sleep loss could worsen another condition, or if pain and sleep problems keep feeding each other, a specialty pain and sleep clinic can help decide whether full SRT, a gentler compression plan, or a different behavioral approach makes the most sense.
What to Expect on Your SRT Journey
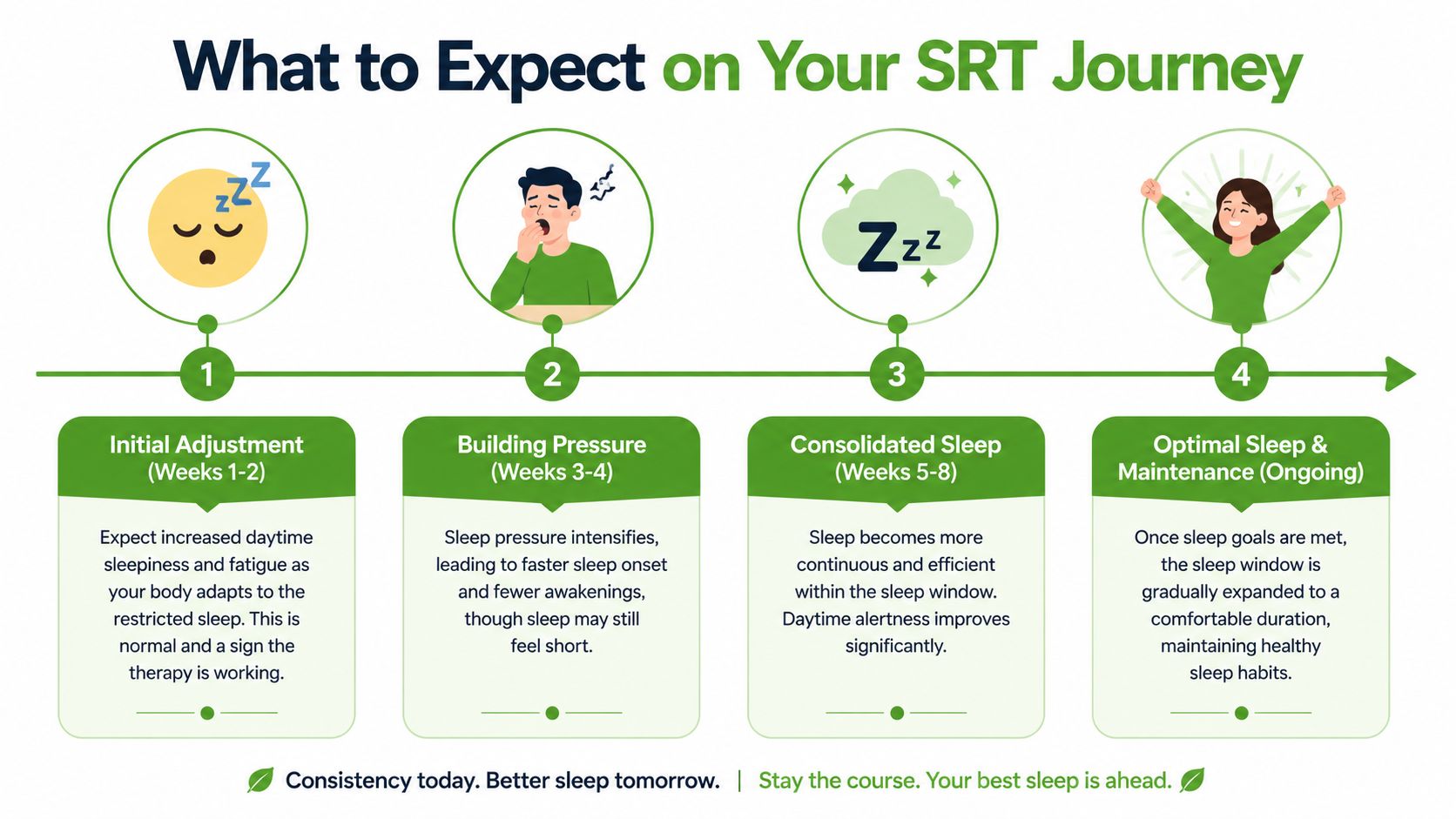
The early stretch of sleep restriction therapy is often the hardest. You may feel more tired during the day. That doesn't automatically mean the treatment is failing. Often, it means your body is finally building stronger sleep pressure instead of scattering it across the day and night.
A patient might say, “I'm going to bed later, and I don't love that.” Fair response. But after the first rough period, many people notice something important. They fall asleep faster, spend less time staring at the ceiling, and stop dreading the bed itself.
The first phase feels uneven
The beginning can be emotionally noisy. One better night may be followed by a messy one. That doesn't mean you should keep redesigning the plan every day.
What helps during this phase is support and structure. Some people pair SRT with calming routines or simple sleep breathing exercises to reduce the urge to tense up when bedtime approaches.
“The goal isn't a perfect night right away. The goal is a more stable pattern.”
Why people stay with it
A large randomized trial found that people assigned to sleep restriction therapy had a lower Insomnia Severity Index score than a sleep hygiene group after 6 months, with scores of 10.9 versus 13.9, as reported in this summary of the randomized trial. The same report noted a 95.3% probability that SRT was cost-effective in a publicly funded health system.
That matters for patients because it suggests this isn't just a clever idea. It can produce meaningful improvement and can be delivered in a way that scales beyond one specialist office.
The long-term payoff
The reward isn't just more sleep on paper. It's what changes during the day:
- Less clock-watching: You stop monitoring every minute.
- More confidence: A bad night feels less catastrophic.
- Fewer “rescue behaviors”: Less napping, less going to bed extra early, less bargaining with sleep.
- A calmer relationship with bedtime: Bed starts to feel boring again, which is good.
People often want SRT to erase all bad nights. No treatment can promise that. A better goal is this: fewer wakeful hours in bed, more trust in your schedule, and a sleep pattern that no longer controls your whole mood.
Is Sleep Restriction Therapy Safe for You?
You are exhausted, and someone tells you the treatment involves spending less time in bed at first. That can sound backwards, even harsh. The logic is real, but so are the trade-offs.
Sleep restriction therapy works like resetting a miscalibrated thermostat. The short-term cost is usually more sleepiness before sleep becomes more predictable. For a healthy person with straightforward insomnia, that trade can be reasonable. For someone with chronic pain, heavy daytime sleepiness, a shifted body clock, or a job where one drowsy hour could cause harm, it may be the wrong place to start.
A review on sleep restriction therapy implementation challenges notes that sticking with the protocol can be hard, and that extra caution is needed for people with fatigue, safety-sensitive responsibilities, chronic pain, or circadian rhythm problems, as discussed in this review on sleep restriction therapy and implementation challenges.
When caution matters most
The first question is not, “Can SRT help insomnia?” The first question is, “Can I do this safely?”
Use extra caution if any of these fit:
- Safety-sensitive work: driving, operating machinery, clinical care, shift supervision, or any role where slower reaction time could hurt you or someone else
- Chronic pain: pain can wake you repeatedly, which means the problem may not be time in bed alone
- Circadian rhythm problems: delayed sleep phase, rotating shifts, or irregular sleep timing can make a strict window harder to place correctly
- Severe daytime impairment: if you are already fighting to stay awake, an initial increase in sleepiness may be too much
Those are not signs that you are failing treatment. They are signs that the treatment needs fitting, the way a brace or medication plan needs fitting.
Why coexisting conditions change the decision
Insomnia often overlaps with other problems. Snoring, mouth breathing, jaw clenching, TMJ pain, frequent awakenings, and a revved-up stress response can all blur the picture. In that situation, SRT can be too blunt if used alone.
A specialty clinic can sort out what is driving the awakenings. For example, Pain and Sleep Therapy Center evaluates sleep-related breathing concerns, TMJ symptoms, and related sleep complaints, which can matter when insomnia sits beside pain or airway issues. If sleep loss is colliding with more than one problem, guided treatment is usually safer than trying to force a strict schedule on your own.
A practical self-check before you start
Ask yourself four plain questions:
- Could extra sleepiness create a safety risk at work, on the road, or at home?
- Do pain, breathing issues, or an irregular schedule seem to be part of my sleep problem?
- Am I so fatigued already that even one harder week would be difficult to manage?
- Would a slower approach, such as sleep compression, fit my body and responsibilities better?
If several answers raise concern, get professional guidance first.
That does not mean you have no behavioral options. It may mean starting with a gentler method, especially sleep compression, where the sleep window is reduced more gradually. SRT can be highly effective, but safety and follow-through matter as much as theory.
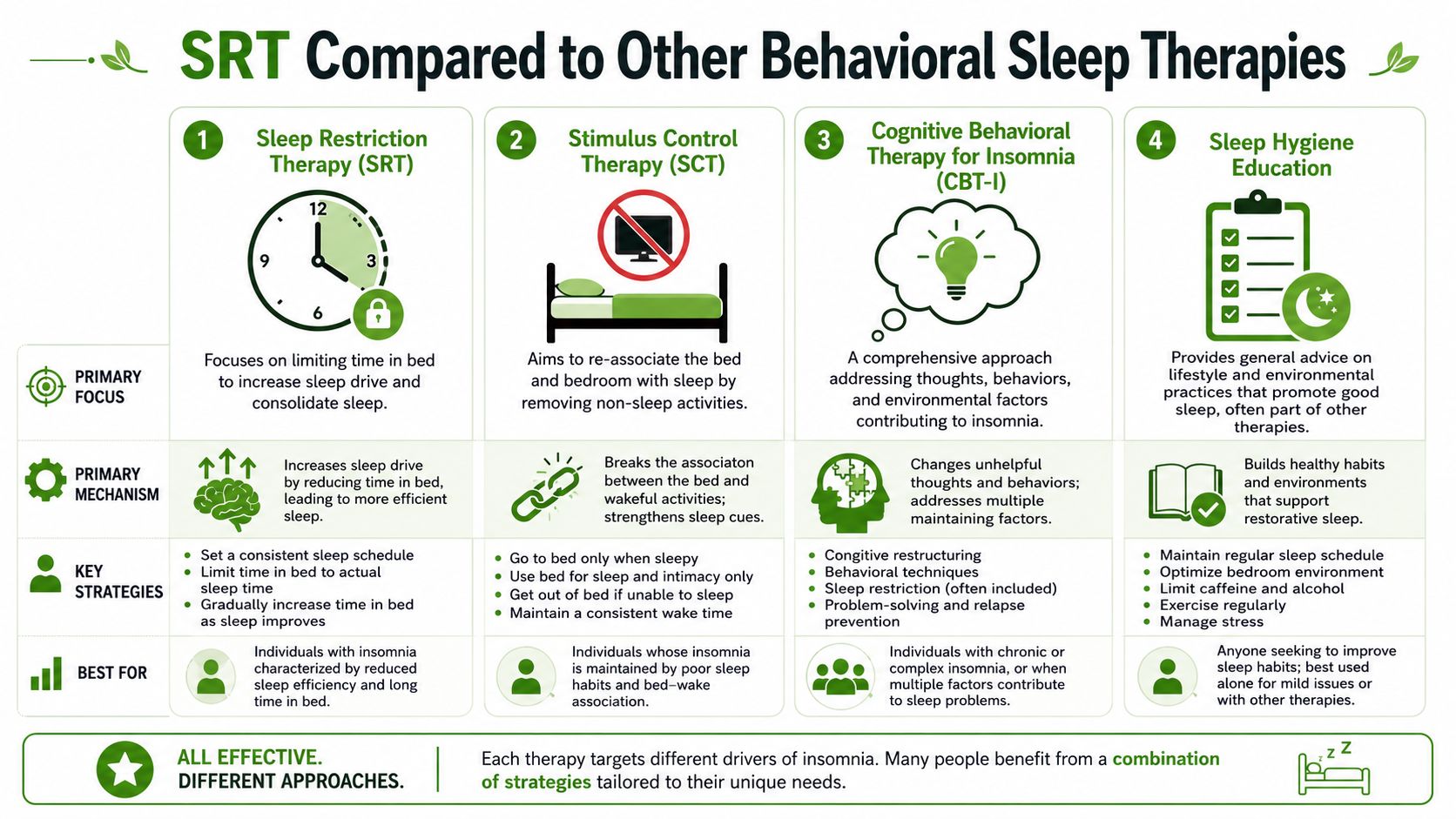
SRT Compared to Other Behavioral Sleep Therapies
Sleep restriction therapy gets a lot of attention because it's concrete and often effective. But it isn't the only behavioral option. For many people, the better question isn't “Does SRT work?” It's “Which insomnia tool fits my body, schedule, and tolerance level?”
SRT versus sleep compression
Sleep compression is often presented as the gentler cousin of sleep restriction therapy. Both aim to reduce excessive time in bed. The difference is pace. Compression usually narrows that window more gradually, which can feel more manageable for people who fear the initial fatigue of SRT.
According to this expert discussion of sleep compression versus sleep restriction, sleep compression may be easier to tolerate for some patients and may improve adherence, while traditional SRT may work faster and more effectively for many cases of insomnia. This is the fundamental trade-off. Faster improvement versus easier tolerability.
A quick comparison helps:
| Therapy | Main idea | Best fit for | Main drawback |
|---|---|---|---|
| Sleep restriction therapy | Tightens time in bed more directly | People ready for a structured, disciplined approach | Early fatigue can be hard |
| Sleep compression | Reduces time in bed more gradually | People worried about worsening daytime sleepiness | Progress may feel slower |
Where stimulus control fits
Stimulus control therapy targets a different insomnia driver. It works on the learned link between bed and wakefulness. If your brain has started treating the bed like an office, a theater, or a worry station, stimulus control helps reset that connection.
Typical ideas include using bed mainly for sleep, getting out of bed when you're awake for a long stretch, and returning only when sleepy. SRT and stimulus control often pair well because one builds sleep pressure and the other repairs the bed-sleep association.
How these fit inside CBT-I
CBT-I is the umbrella treatment. It often includes SRT or sleep compression, stimulus control, and work on unhelpful sleep beliefs and habits. Sleep hygiene by itself is usually the lightest-touch piece. It can support treatment, but it rarely carries the whole load for chronic insomnia.
Here's a practical way to choose:
- Choose SRT when: you want a structured plan and can tolerate a tougher start.
- Choose sleep compression when: you're concerned that abrupt restriction will backfire because of fatigue, pain, or fear of feeling worse.
- Use stimulus control when: your bed has become a place for wakefulness, frustration, or scrolling.
- Think in combinations: many people do best with more than one behavioral tool.
The “best” therapy is often the one you can follow consistently enough for your brain and body to relearn sleep.
Starting SRT Your Questions Answered
People usually hesitate for sensible reasons. They're not resisting treatment. They're trying to protect themselves from feeling worse.
Will I be too tired to function at work
You might feel more tired early on. That risk matters most if your job requires sharp reaction time, driving, or safety decisions. If that's your situation, don't start on your own. Get guidance first and consider whether a gentler option, such as sleep compression, fits better.
What if I have a terrible night and can't stick to the schedule
One bad night doesn't mean the plan failed. The danger is reacting to every rough night by sleeping late, going to bed early, or changing the schedule midstream. SRT works from weekly patterns, not panic-based daily corrections.
Can SRT help if anxiety or pain is part of my insomnia
Sometimes yes, but that depends on what's driving the awakenings. If anxiety, chronic pain, jaw tension, facial pain, snoring, or breathing problems are part of the picture, the insomnia plan may need to be modified. That's where specialty care becomes important. Treating only the insomnia behavior while ignoring pain or airway issues can leave the root problem untouched.
Do I need professional help
If your insomnia is straightforward, some people can begin with education and careful tracking. If your situation includes pain, daytime impairment, irregular schedules, or suspected sleep-disordered breathing, professional help is the safer path.
Sleep restriction therapy is one of the clearest examples of a treatment that can be both highly effective and hard to do well without support. The method is simple on paper. Real life is not. Coexisting conditions change the plan, and that's especially true when insomnia overlaps with TMJ symptoms, facial pain, or breathing-related sleep disruption.
If your sleeplessness overlaps with jaw pain, headaches, facial tension, snoring, mouth breathing, or suspected sleep apnea, Pain and Sleep Therapy Center offers evaluation and treatment for those connected problems. Their team focuses on root-cause assessment for TMJ disorders, facial pain, and sleep-related breathing issues, which can be an important next step when insomnia isn't happening in isolation.



