
If you're listening to your baby on the monitor and every breath sounds thick, rattly, or snuffly, you're not overreacting by paying attention. A 5 month old congested at bedtime can make even calm parents feel on edge, especially when feeding slows down, sleep gets choppy, and the noises seem louder in the dark.
Most of the time, congestion at this age is manageable with careful home care. What matters most is not how dramatic it sounds, but whether your baby is feeding well, staying hydrated, and breathing without struggle. The hard part is that babies often sound worse than they are because their nasal passages are small, so even a modest amount of mucus can create a lot of noise.
In clinic, I also see another layer that often gets missed. Some babies aren't just dealing with a passing cold. They may have recurrent stuffiness, noisy sleep, poor latch patterns, mouth-open posture, or signs that nasal breathing and oral function aren't working smoothly together. That doesn't mean something is seriously wrong, but it does mean the right question isn't always only, “How do I get the mucus out?” Sometimes it's also, “Why does this keep happening?”
The Worrying Sounds of a Stuffy Baby
It is often 2 a.m. when parents hear it most clearly. A rattly inhale. A snort through the monitor. A baby who settles, then stirs again because breathing through a blocked nose takes more effort than it should.
At 5 months, those sounds can be unsettling, but the sound alone does not tell the whole story. Small nasal passages make even a little swelling or mucus seem loud. What matters more is function. Can your baby feed with reasonable comfort, stay asleep for stretches, and breathe without pulling, flaring, or tiring out?
In clinic, I pay close attention to the pattern. A short run of congestion with a cold is common. Recurrent stuffiness, noisy sleep between illnesses, frequent popping off the breast or bottle, mouth-open posture, or chronic snoring points to a different question. The issue may not be mucus alone. It may be that nasal breathing is already restricted, or that oral function is not supporting an easy suck-swallow-breathe pattern.
What these sounds can mean
Parents usually notice the noise first, but the day-to-day changes are often more useful:
- Feeds become less efficient: Your baby pauses often, loses the seal, gulps air, or seems frustrated because breathing through the nose is harder.
- Sleep turns restless: A baby who was settling well may wake more often, especially after lying flat long enough for swelling and secretions to build up.
- Breathing sounds vary by position: Louder congestion on the back can happen with a simple cold, but it can also show up in babies who already struggle with nasal airflow.
- You hear congestion without much mucus: That can happen when the nose is inflamed, dry, narrow, or blocked higher up, not just when drainage is visible.
This is also where parents can miss the root cause. Some babies with persistent congestion are working around tongue restriction, a high palate, poor lip seal, or chronic nasal obstruction. Those babies may sound “always stuffy,” even when they are not acutely ill.
Home care still helps, but technique matters. Saline is often the first useful step because it loosens sticky mucus and reduces irritation. If you want a quick explanation of what is 0.9 saline, that overview covers the basics. For babies with recurring nasal stuffiness, parents also benefit from learning gentle breathing support strategies for nasal congestion so they can think beyond repeated suction alone.
One practical point matters here. A noisy baby may still be okay. A baby who feeds poorly, sleeps poorly, and seems to fight for nasal airflow needs closer attention, even if there is no dramatic cough or fever.
Your Step-by-Step Guide to Clearing Tiny Noses
When a 5 month old congested baby is struggling to feed or settle, parents often jump straight to suction. That usually isn't the best first move. Thick mucus doesn't come out well unless you loosen it first.
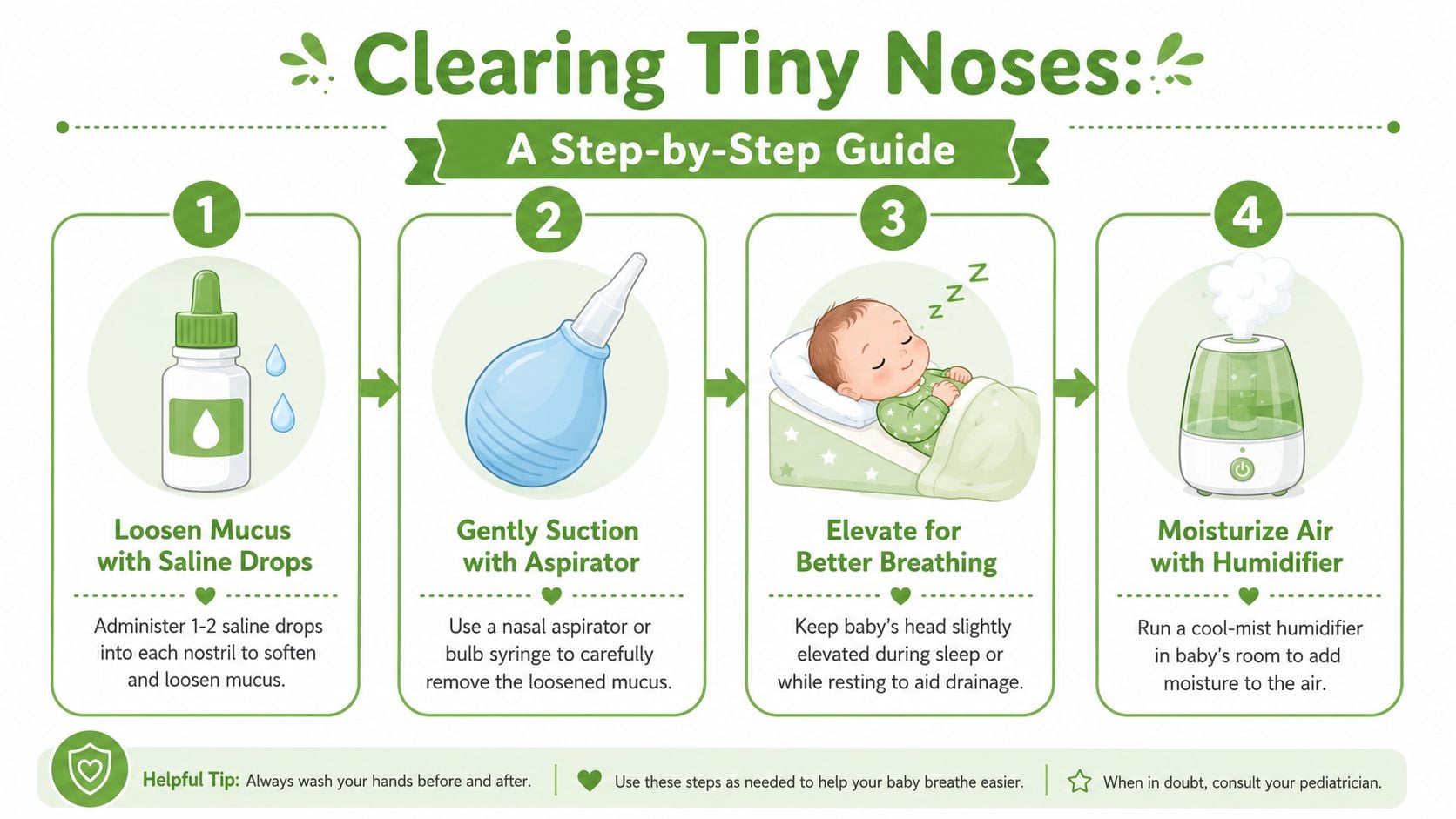
Pediatric guidance recommends a stepwise approach: use 2 to 3 saline drops in each nostril, then gentle suction with a bulb syringe or infant aspirator, and repeat only as needed to support feeding and sleep. It also specifically recommends suctioning before nursing or bottle-feeding because nasal blockage can interfere with intake, as outlined by the American Academy of Pediatrics guidance on stuffy noses and safe sleep.
The routine that works best
Use this as a short protocol, not an all-day cycle.
Start with saline
Place 2 to 3 saline drops in each nostril. This softens dried or sticky mucus so suction can remove it more effectively. If you've ever wondered about the type of saline used in infant nose care, this overview of what is 0.9 saline gives helpful background in plain language.
Wait briefly
Give the saline a little time to loosen secretions. You don't need to rush the next step.
Suction gently
Use a bulb syringe or infant aspirator with a light touch. With a bulb syringe, compress the bulb before placing it at the nostril opening, then release gently to draw mucus out. Don't insert the tip deep into the nostril.
Time it before feeds or sleep
Another pediatric source advises 2 drops of plain saline in each nostril, then suctioning, ideally about 15 minutes before feeding or naptime, and notes that cold medicine isn't recommended for children under 6 years. It also notes that small amounts of water are only discussed for babies at least 6 months old, which means a 5-month-old is still below that point, according to Children's Health guidance on nasal congestion in babies and toddlers.
What not to do
Over-treatment is one of the biggest mistakes I see. More suction doesn't always mean more relief.
- Don't suction too often: Repeated suction can irritate the nasal lining and increase swelling.
- Don't use cold medicine: Supportive care is the standard approach for infants. Medication isn't the fix here.
- Don't improvise harsh tools: The nose lining is delicate. Gentle technique matters more than device brand.
- Don't assume dry air is helping: Dry rooms often make sticky mucus harder to clear.
Practical rule: If suctioning leaves your baby more upset, more swollen, and not much clearer, back off and focus on saline, humidified air, and another attempt later.
A cool-mist humidifier can help keep secretions from drying out overnight. That won't remove mucus on its own, but it often makes the saline-and-suction routine work better and keeps the room more comfortable.
The short video below walks through the general process many parents find easier after seeing it done once.
For families dealing with ongoing nasal stuffiness, I also encourage looking beyond the immediate clean-out routine and paying attention to breathing habits during the day. Simple airway-focused strategies can matter over time. This overview of breathing exercises for nasal congestion may be useful for understanding the broader breathing side of the problem, especially in households where congestion tends to recur.
Ensuring Safe Sleep for a Congested Baby
The strongest instinct many parents have at night is to prop the baby up a little. It feels logical. Adults often breathe more comfortably with their upper body somewhat lifted, so parents assume a baby will too.
That is where safety has to come first.

Authoritative guidance for a congested infant is clear: babies should still sleep flat on their back, not on an incline and not in a changed sleep position just to reduce congestion sounds. Guidance discussed by the AAP emphasizes that congestion can make babies sound worse than they are, and the safer response is supportive care, not repositioning during sleep, as explained in this AAP discussion on congested babies and sleep position.
Unsafe fixes parents are often tempted to try
These are common, and they aren't the answer:
- Crib elevation: Raising one end of the crib can create an unsafe sleep setup.
- Side-sleeping: Babies should still be placed on their back.
- Inclined sleepers or loungers: These aren't substitutes for a flat, firm sleep surface.
- Sleeping on a couch or armchair with a parent: This is especially risky, even if a baby seems more settled upright.
What actually helps at night
Instead of changing the sleep surface, improve the conditions around it.
A cool-mist humidifier may help keep the air from drying the nose further. Feeding matters too. If congestion is disrupting intake, offer feeds more frequently so hydration stays steady. At this age, routine water isn't the fallback. Milk feeds are still the main support.
A safer crib beats a quieter-sounding night. Noise alone isn't the reason to trade away safe sleep.
Parents who want a broader refresher on room setup, sleep environment, and practical safety basics may find this parent's guide to baby sleep safety useful. The core principle is simple and worth repeating: congestion is uncomfortable, but the crib rules don't change because of it.
Red Flags When to Call the Pediatrician
It is 2 a.m., your 5 month old sounds packed up, feeds poorly, and seems harder to settle than usual. The question is no longer what color the mucus is. The question is whether breathing, hydration, or energy level has changed enough that your baby needs medical care.
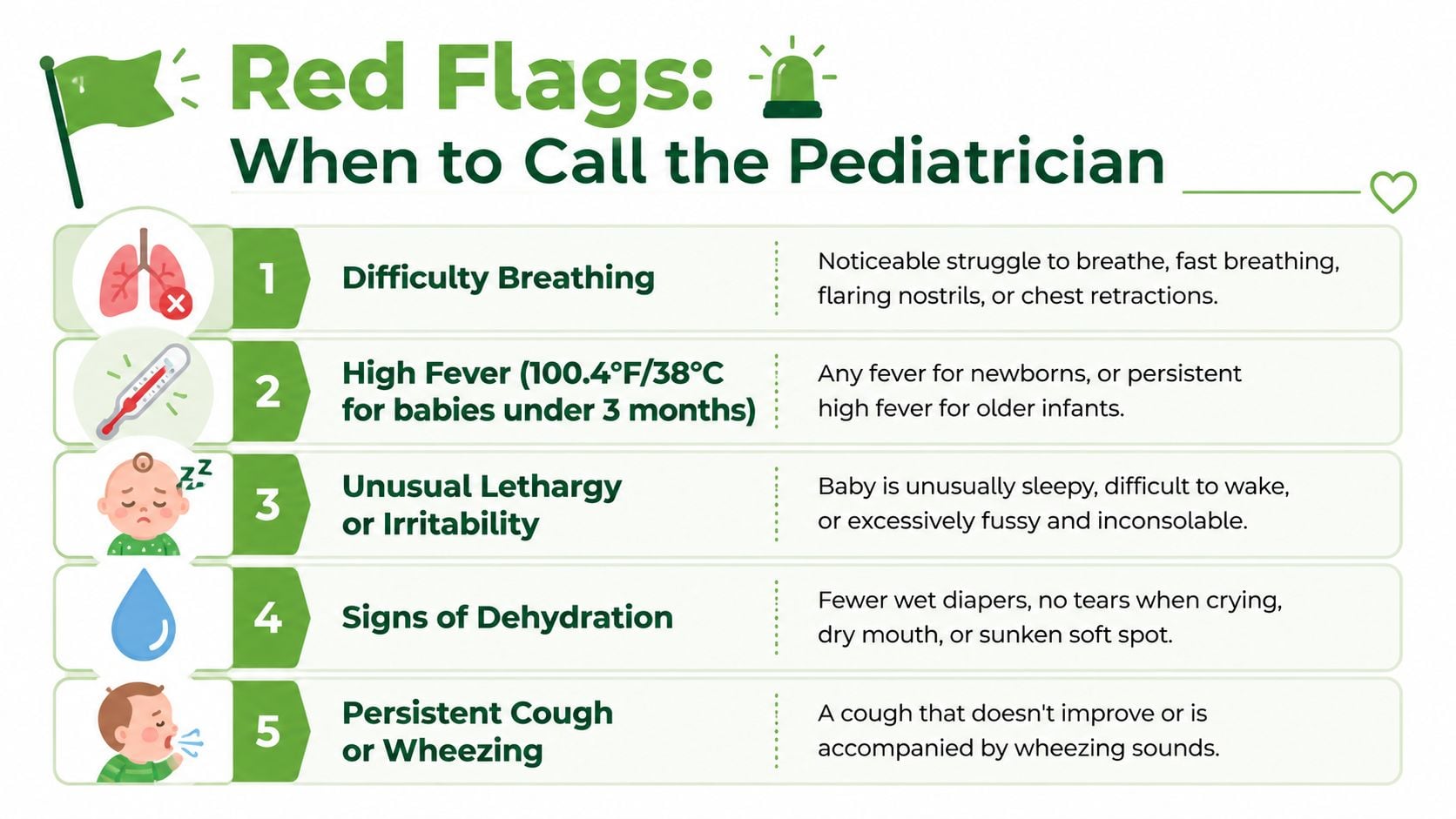
At this age, many stuffy noses are still caused by a short-lived virus. What concerns me more in clinic is visible breathing effort, a drop in feeding, fewer wet diapers, fever, or congestion that lingers instead of clearly improving. Recurrent episodes also matter. A baby who sounds congested over and over may need more than routine home care.
Red Flag Symptoms Checklist
| Symptom Category | What to Look For |
|---|---|
| Breathing trouble | Fast breathing, chest pulling in, nostrils flaring, grunting, pausing, or breathing that looks labored instead of just noisy |
| Hydration concerns | Fewer wet diapers, poor intake, dry mouth, crying with few tears, or tiring out before finishing feeds |
| Color change | Blue, gray, or pale color around the lips or face |
| Fever or worsening illness | Fever with congestion, unusual sleepiness, irritability that is hard to soothe, or a baby who seems increasingly unwell |
| Ongoing symptoms | Congestion that persists, worsens, or keeps coming back rather than following a simple cold pattern |
When I tell parents not to wait
Call promptly if your baby's breathing looks different from their normal. Parents often notice this before they can name it clearly. If you are watching the ribs pull in, the nostrils flare, or the baby struggle to coordinate sucking and breathing, that deserves attention.
Feeding changes are another major clue. A congested infant may latch, pull off, swallow more air, or fatigue early at the breast or bottle. If that pattern leads to lower intake or fewer wet diapers, the threshold for calling gets much lower.
Blue lips, pauses in breathing, marked lethargy, or a baby who cannot feed should be treated as urgent.
It also helps to know what more serious breathing trouble can look like. This page on airway obstruction symptoms gives a useful frame for recognizing when noisy breathing may be crossing into true distress.
For families who want more confidence in urgent illness situations, a review of first aid for children can help you respond more calmly while you contact your pediatrician.
One more point matters here. If your baby repeatedly gets labeled as "just congested" but the pattern includes noisy feeds, chronic mouth opening, restless sleep, or symptoms that return between colds, ask for a closer look. In some infants, the red flag is not a dramatic emergency. It is the repeat pattern that suggests an airway or oral-function issue underneath the congestion.
When Congestion Is More Than Just a Cold
This is the part many parents don't hear enough about. Some babies get congested with ordinary viral illnesses and improve with time. Others seem to be stuffy again and again, sound blocked without much mucus, feed noisily, sleep with an open mouth, or struggle with latch and oral coordination.

Public guidance often covers urgent warning signs well, but it doesn't always explain that persistent or recurrent congestion can reflect non-viral causes such as anatomy, reflux-related irritation, or environmental triggers, which may need evaluation rather than more home care, as discussed in this review of newborn congestion without obvious mucus.
Patterns that deserve a closer look
In an airway-focused practice, I pay attention to patterns like these:
- Congestion without much visible mucus
- Repeated feeding struggle that improves only briefly after suction
- Noisy sleep that returns between illnesses
- Mouth-open posture or difficulty maintaining nasal breathing
- Recurrent waking that seems tied to breathing discomfort
A simple cold can cause some of those features for a few days. A repeating pattern raises a different question.
Where oral function can fit in
Oral function and nasal breathing are closely connected. If a baby has inefficient latch mechanics, restricted tongue movement, poor oral seal, or compensatory mouth-open posture, the entire breathing-feeding-sleep system can get less efficient. In some infants, a tongue-tie or other oral restriction may not cause congestion directly, but it can contribute to the way feeding, swallowing, and airway behavior interact.
That doesn't mean every congested baby needs a tongue-tie evaluation. It does mean recurrent congestion shouldn't always be treated as a standalone nose problem.
Environmental irritation and reflux can also play a role. A baby may not have dramatic spit-up and still show signs of upper airway irritation. When stuffiness keeps returning, the useful question is whether the nose is the source of the problem or only the place where the problem shows up.
One practical caution applies here too: don't move from saline to medicated nasal products on your own. Parents sometimes ask about stronger decongesting sprays because they want fast relief, but medication choices around infants need clinical guidance. For older children and nursing parents who are sorting through medication questions, this article on Afrin and breastfeeding gives a good example of why nasal medications deserve more thought than is typically given.
For families who need a more root-cause evaluation, clinics that assess airway development, oral function, feeding mechanics, and sleep-related breathing may be helpful. Pain and Sleep Therapy Center is one such option for pediatric airway and oral-function assessment when recurrent symptoms suggest the issue may be broader than a temporary cold.
Your Path to Peaceful Breathing and Sleep
A congested baby can make a household feel tense fast. The best response is calm, observant, and practical. Clear the nose with good technique, keep feeds going, use humidified air, and avoid the common mistakes that create more irritation than relief.
At the same time, don't dismiss what your instincts are telling you. If breathing looks harder, intake drops, wet diapers decrease, or the illness lingers beyond the usual window, get medical help. Parents often notice the shift before anyone else does.
The other takeaway is just as important. If your baby seems congested often, sounds blocked without much mucus, or struggles repeatedly with feeding and sleep, it may be time to think beyond “just another cold.” Nasal breathing, oral function, feeding mechanics, and airway comfort are connected. When one part isn't working well, the whole system can look congested.
Calm care works best when it's paired with careful observation. Relief is important, but so is asking why the problem keeps showing up.
You don't need to solve everything in one night. You do need a safe plan, a clear sense of red flags, and the willingness to look deeper when the pattern doesn't add up.
If your child's congestion seems persistent, recurrent, or tied to feeding, oral function, or sleep disruption, Pain and Sleep Therapy Center offers airway-focused evaluation that looks beyond temporary symptom relief. Their team works with families who want a clearer picture of how nasal breathing, oral posture, tongue function, and sleep may be interacting so the next step is based on root cause, not guesswork.



