
Hearing that you may need jaw surgery can make everything feel suddenly bigger than it was yesterday. The clicking, headaches, clenching, facial tension, poor sleep, or bite changes were already stressful enough. Then one consultation turns into a new fear: Will this require a major operation?
For some people, surgery is the right answer. But for many others, it isn't the first step, and it isn't the only step. A careful plan can often improve jaw function, reduce pain, support breathing, and stabilize the bite without moving straight to an operating room.
What matters most is asking a better question. Not just, “How do we fix my jaw?” but, “Why is my jaw overloaded in the first place?” When treatment starts there, the list of useful jaw surgery alternatives gets much wider and much more practical.
Is Surgery Really Your Only Option
A patient sits in my office after hearing the words "jaw surgery consult," and the fear is usually immediate. They are not only worried about the procedure itself. They are worried that they waited too long, that something is badly wrong, or that surgery is the only serious option left.
That conclusion is often premature.

Jaw surgery has a clear role. I refer for it when the problem is truly structural and conservative care will not create a stable result. But many patients who are told to "consider surgery" have never had a full functional workup of the airway, muscle pattern, tongue posture, sleep quality, cervical posture, and joint loading. If those drivers are missed, an operation may change anatomy without fixing the strain that created the symptoms.
A second look should answer practical questions:
- Is the main problem bone position, muscle strain, joint irritation, or a mix of the three?
- Are clenching, poor sleep, mouth breathing, or forward head posture keeping the jaw under constant load?
- Does the bite look off because the jaw is unstable, or is the jaw unstable because the muscles and airway are compensating?
- Would symptom control and better function change the treatment plan enough to delay or avoid surgery?
These details matter because the jaw does not function in isolation. A narrow airway can shift how a person holds the tongue and head. That change can increase muscle tension, alter the resting jaw position, and overload the joints. In the right patient, treating breathing and muscle function first can lower pain, improve bite stability, and make invasive treatment unnecessary.
I also encourage patients to understand how surgeons decide when an operation is appropriate. This overview of surgery for jaw realignment explains where surgical care fits within the wider treatment picture.
Before anyone commits to surgery, I want to know whether the system can calm down with less invasive care. That may include a well-designed orthopedic appliance, targeted physical therapy, myofunctional therapy, sleep and airway evaluation, nasal breathing support, and selective orthodontic planning. Used together, these options aim at the root cause rather than chasing the loudest symptom.
If you are trying to compare opinions, it can also help to review how another practice approaches Inspire Dental Group for TMJ. The key is not to collect the most opinions. It is to get the right diagnosis.
Surgery should be considered carefully, not assumed early.
Understanding Why Your Jaw Needs Help
Jaw pain rarely starts with “bad luck.” In many patients, the jaw is acting like the visible crack in a house wall while the deeper problem sits in the foundation.
If the tongue rests low, the lips stay apart, the head drifts forward, and breathing shifts through the mouth, the jaw joints and surrounding muscles have to compensate all day and all night. Teeth may still fit together on paper, but the system isn't balanced. That is why two people with a similar bite can have completely different symptoms.
The jaw doesn't work alone
The temporomandibular joints are small joints with a demanding job. They coordinate with the neck, airway, teeth, tongue, facial muscles, and nervous system. When one part starts adapting poorly, the others follow.
A simple way to look at it:
- Tongue posture affects palate shape and muscle tone
- Breathing pattern affects head and neck posture
- Head and neck posture affects jaw position
- Jaw position affects bite loading and joint stress
Many discussions of jaw surgery alternatives miss this chain. Yet soft tissue posture, including the tongue, palate, and neck, interacts closely with jaw position, and even modest reductions in upper airway size increase the risk of sleep apnea and craniofacial strain (Cleveland Clinic discussion of jaw surgery and airway considerations).
Why diagnosis gets oversimplified
Patients are often told they “have TMJ,” as if that is one single condition. It isn't. TMJ symptoms may come from disc displacement, irritated ligaments, overloaded muscles, unstable occlusion, airway strain, or a mix of all of them.
That's why a broad evaluation matters more than a label. If you want a helpful example of how clinicians frame these issues for patients, Inspire Dental Group for TMJ offers a useful overview of the kinds of symptoms and contributors that often travel together.
The jaw is often the victim, not the original problem.
Root causes that commonly get missed
Three patterns show up again and again in people who are trying to avoid surgery:
- Mouth breathing and poor nasal function These can pull the tongue down and change how the jaw is held at rest.
- Forward head posture This increases neck and facial muscle activity, especially in people who already clench.
- Unstable oral posture If the tongue, lips, and swallow pattern are dysfunctional, the jaw never gets consistent support.
When those patterns are corrected, pain often becomes easier to calm, the bite often feels less strained, and the case becomes clearer. Sometimes the patient still needs surgery. Sometimes they don't. But either way, the treatment plan becomes smarter.
Conservative Therapies for Foundational Support
The most overlooked jaw surgery alternatives are the ones that teach the body to stop recreating the same problem. They don't just cover symptoms. They change habits of breathing, posture, swallowing, and muscle recruitment that can keep the joints irritated.
A patient starting this kind of care usually expects something dramatic. Instead, the early work often feels surprisingly simple. Learning how the tongue should rest. Practicing nasal breathing when walking or working. Noticing how often the teeth touch during the day. Releasing neck and jaw guarding that has become automatic.
Myofunctional therapy
Orofacial myofunctional therapy focuses on oral posture and movement patterns. That includes where the tongue rests, how the lips seal, how swallowing happens, and whether the jaw is constantly bracing.
In practical terms, sessions often involve guided exercises, habit tracking, and progressions that reconnect breathing and muscle function. For the right patient, this matters far more than it sounds. If the tongue stays low and the mouth stays open, the jaw doesn't get stable support.
Physical therapy and postural work
Jaw-focused physical therapy isn't just “stretch your jaw and hope.” Good therapy looks at the neck, upper shoulders, rib position, head carriage, and how the mandible moves during opening and closing.
Patients often notice two things early. First, some of their “jaw pain” is muscle referral from the neck and chewing muscles. Second, posture changes are easier when breathing improves, because the body no longer needs the same compensations.
A useful self-education resource for people who suspect clenching is part of the cycle is this guide on managing nighttime teeth grinding. It can help you identify common behaviors that keep the system irritated between visits.
Guided bite correction and breathing retraining
Sometimes the jaw is not closing into its most comfortable or physiologic position. In those cases, clinicians may use postural bite correction, trial appliances, or guided mandibular positioning to reduce joint loading while the rest of the system is retrained.
The evidence here is meaningful. Studies using jaw tracking systems show that guided mandibular repositioning can reduce disk-mediated TMJ pain in 55 to 75% of patients over 3 to 6 months, especially when combined with training that improves tongue posture and nasal breathing. The broader point is important: coordinated myofunctional therapy and postural bite correction can help many patients bypass orthognathic surgery.
Practical rule: If a treatment changes the bite but ignores breathing and muscle function, expect the body to keep fighting back.
What patients often get wrong
People usually want to know which exercise, appliance, or therapy is “best.” That's the wrong target. Foundational therapy works when the pieces reinforce one another.
Here's what tends to help:
- Consistency beats intensity Brief daily drills usually outperform occasional heroic effort.
- Rest posture matters more than performance How you breathe and hold your jaw for the other hours of the day matters most.
- Symptom shifts aren't always linear Less clicking, less morning tension, fewer headaches, and easier nasal breathing may happen at different times.
These approaches do require participation. They are not passive. But for patients who want relief without jumping straight to surgery, that active role is often a strength, not a burden.
Appliance and Orthodontic Alternatives
A lot of anxious patients arrive expecting a simple answer. “Can I just get a guard?” or “Can braces fix this so I can avoid surgery?” Sometimes yes. Sometimes those tools help a great deal. But the right appliance only works when it matches the actual problem, whether that is joint compression, a strained bite, a narrow upper jaw, or an airway pattern that keeps pulling the system off course.
This part is often missed. Teeth, jaw joints, tongue posture, neck posture, and breathing habits affect one another. If treatment moves teeth but leaves mouth breathing, poor tongue posture, or heavy muscle tension unchanged, the result is often unstable.
Splints and orthotics
A custom oral appliance can reduce pressure on the temporomandibular joints, settle overworked muscles, and help identify a jaw position that feels more stable and repeatable. In practice, I often use an appliance as both a treatment tool and a diagnostic test. If symptoms ease when the joints are unloaded and the muscles stop guarding, that tells us something important about the source of the problem.
Device choice matters.
A store-bought guard may protect enamel from grinding, but it usually does not address joint mechanics, airway strain, or the muscle patterns driving the clenching in the first place. A poorly designed appliance can also increase joint irritation if it holds the jaw in a position your muscles cannot support. Patients comparing options usually benefit from reading about alternatives to mouth guards for TMJ and airway-related problems, because simple tooth protection and full-jaw stabilization are not the same thing.
Orthodontic camouflage
Braces and clear aligners can improve bite fit, tooth position, and appearance without surgery in selected cases. That approach is called camouflage orthodontics. It means the teeth are moved to function better within the existing skeletal pattern, rather than surgically changing the jaw bones themselves.
That can be a reasonable choice for mild to moderate discrepancies, especially when the patient wants less invasive care and the joints are stable. It also has limits. Camouflage can improve contacts between the teeth, but it cannot fully correct a large skeletal mismatch, a restricted airway, or a jaw position that keeps overloading the TMJs. The key question is not just “Can the teeth be straightened?” It is “Will the bite work better with the joints, muscles, and airway after treatment is finished?”
MARPE and MSE
For adults with a narrow upper arch, crowded dental arches, or signs that limited maxillary width is contributing to airway strain, mini-screw assisted rapid palatal expansion, or MARPE, and related systems such as MSE may offer a non-surgical path.
These devices aim to widen the upper jaw more than standard orthodontics can. In the right patient, that can create space for the tongue, improve nasal breathing, and reduce the compensations that keep the jaw and neck working too hard. I do not view expansion as a tooth-straightening project alone. It is often part of a larger effort to improve how the patient breathes, swallows, and holds the jaw at rest.
Candidacy still has to be checked carefully. Age, bone maturity, gum support, root position, and bite goals all matter. Expansion also needs follow-through. If the arch is widened but the tongue stays low and the patient still breathes through the mouth, the body may keep pulling toward the old pattern.
Comparing non-surgical structural treatments
| Treatment | Primary Goal | Best For | Type of Intervention |
|---|---|---|---|
| Custom splint or orthotic | Reduce joint and muscle overload | TMJ pain, clenching, unstable jaw position | Removable appliance |
| Clear aligners or braces | Reposition teeth for better bite function and esthetics | Mild to moderate discrepancy, dental compensation cases | Orthodontic treatment |
| MARPE or MSE | Widen the maxillary arch and improve transverse space | Narrow upper jaw, selected adult expansion cases | Skeletal anchorage expansion |
A practical way to judge these options is to ask three questions. Are we trying to calm the joint, improve tooth position, or create more room in the upper jaw? Are breathing and muscle habits being addressed at the same time? And will this plan still make sense six months from now, not just on the day the appliance is delivered? Those answers usually tell you whether you are looking at a true alternative to surgery, or only a temporary workaround.
Regenerative Medicine for Joint Healing
Some patients don't primarily need their jaw moved. They need irritated tissues to heal. That is where regenerative medicine enters the discussion.

Think of the TMJ like a worksite with frayed ligaments, inflamed tissue, and a repair crew that has stalled. Regenerative therapies aim to signal that crew to get back to work. They are not merely numbing pain. They are intended to support tissue repair and reduce inflammatory overload.
What these treatments are trying to do
Common options include:
- Prolotherapy This uses an irritant solution to stimulate a healing response in lax or painful connective tissue.
- Platelet-Rich Fibrin or PRF This uses your own blood-derived growth factors as a concentrated healing support.
- Cold laser therapy This applies light-based treatment to support tissue recovery and reduce irritation.
These tools are often considered when the joint capsule, ligaments, or surrounding soft tissues seem to be part of the problem, especially when pain keeps recurring despite appliance support or exercise-based care.
Where they fit in a real plan
Regenerative treatments work best when they are part of a broader strategy. If a patient still clenches heavily, breathes through the mouth, or closes into an unstable bite, injections or laser therapy may help but won't necessarily hold.
Healing the joint without changing the forces on the joint is often incomplete care.
Patients who want a clearer overview of this category can review regenerative medicine for joint pain. The main value of these therapies is that they create another path between symptom management and surgery.
They are not right for every case. But for selected patients, they can reduce pain enough to make myofunctional work, breathing retraining, and bite stabilization more successful.
Weighing Your Options Surgery vs Alternatives
A patient sits in my chair after being told surgery is the next step. They are worried about recovery, worried about getting it wrong, and often unsure whether anyone has fully explained why their jaw is struggling in the first place.
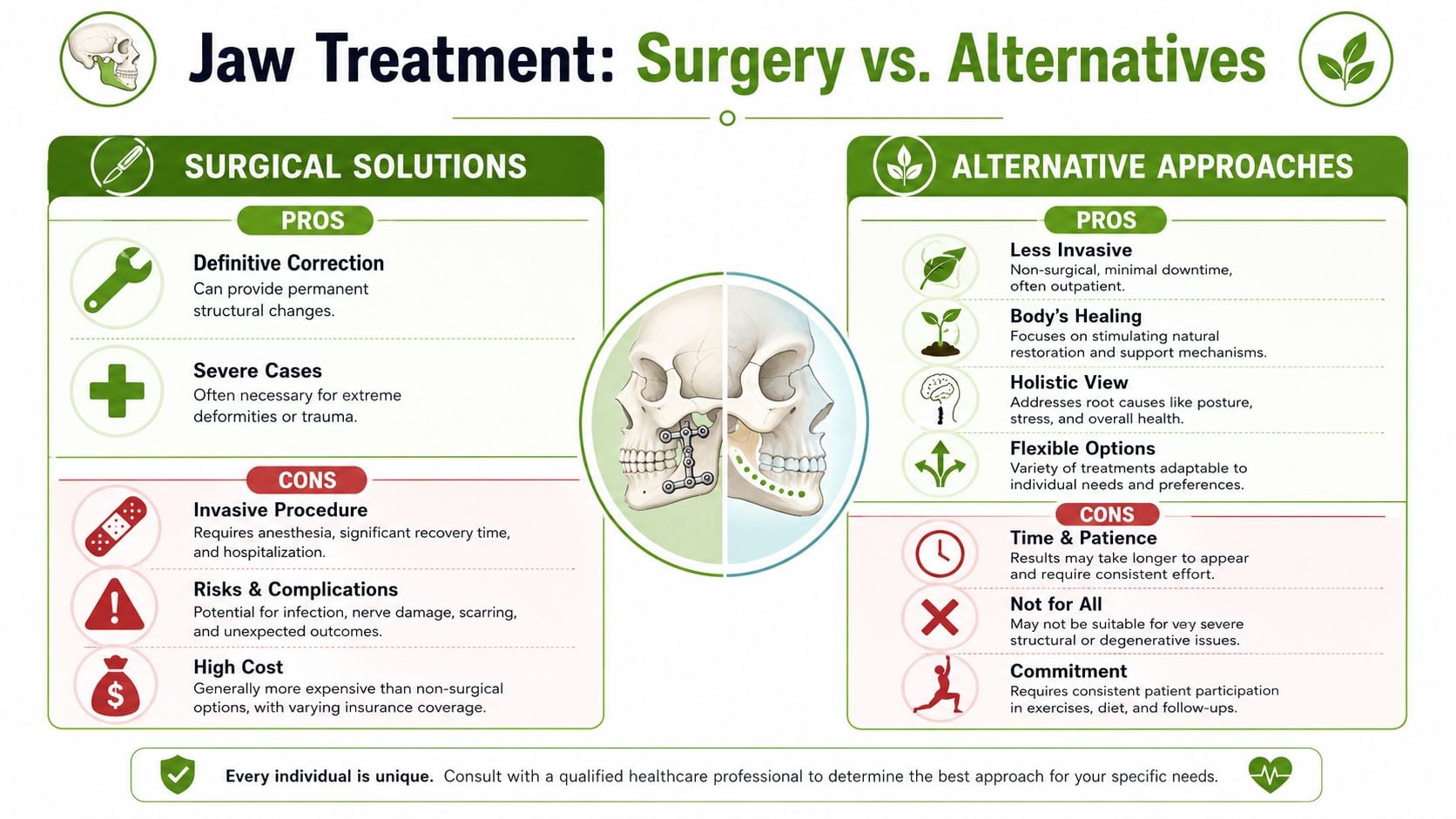
The decision usually comes down to matching the treatment to the driver of the problem. If the main issue is a severe skeletal mismatch, major asymmetry, trauma, or a structural airway problem that cannot be changed conservatively, surgery may be the right tool. If the jaw is being overloaded by poor tongue posture, mouth breathing, neck tension, clenching, unstable bite forces, or joint irritation, surgery may not be the first place to start.
That distinction matters.
Many patients who search for jaw surgery alternatives are not trying to avoid necessary care. They are trying to find out whether a less invasive plan could address the actual source of pain, locking, fatigue, bite strain, or sleep-disordered breathing. In my experience, that is a reasonable question. A phased plan can reduce symptoms, improve function, and clarify whether the remaining problem is truly structural or largely functional.
A practical decision framework
Non-surgical care often makes sense first when:
- Symptoms are driven mainly by muscle tension, joint irritation, or habit patterns
- Breathing, tongue posture, and head and neck posture are part of the picture
- The discrepancy is present but not clearly severe
- The patient wants to improve function before making an irreversible decision
Surgery deserves stronger consideration when:
- The skeletal discrepancy is large enough to limit chewing, speech, airway support, or bite stability
- There is significant asymmetry or trauma-related deformity
- Imaging and clinical exam show structural limits that appliances, therapy, or orthodontics cannot correct
- Good conservative treatment has already been tried and the remaining deficit is still substantial
The missed step in many treatment discussions is the connection between jaw mechanics and airway function. A jaw that sits back, a tongue that rests low, and a patient who breathes through the mouth at night often develop a cycle of muscle guarding, clenching, poor sleep, and joint overload. If those forces stay in place, even a technically successful procedure may leave part of the original strain unresolved. If those forces are addressed early, some patients improve enough that surgery becomes unnecessary, or at least much more targeted.
For a visual walkthrough, this video is a helpful starting point.
The right treatment should solve the underlying problem with the least force necessary.
Frequently Asked Questions About Jaw Treatment
How long do non-surgical treatments usually take
It depends on the driver of the problem. Muscle and breathing changes may start to shift symptoms earlier than orthodontic or expansion changes. Joint healing and habit retraining usually require patience, because the goal isn't just short-term relief. It's a more stable pattern.
Will insurance cover these options
Coverage is often fragmented. Some parts may fall under medical benefits, some under dental, and some may be out of pocket. Patients usually do best when they ask for a written treatment outline, diagnosis language, and billing categories before starting.
How do I know if a provider is looking at root causes
Ask direct questions. Do they evaluate breathing, tongue posture, neck posture, clenching habits, and sleep symptoms, or only your bite? Do they explain why your jaw is overloaded, or do they jump straight to a device or procedure?
Can non-surgical care still help if I was told I'm a surgical case
Sometimes yes. Even when surgery remains likely, conservative treatment can still reduce pain, improve breathing, stabilize muscles, and clarify what surgery would or would not fix. That often leads to a better outcome and a more informed decision.
What should I bring to a consultation
Bring imaging reports if you have them, a list of symptoms, notes about headaches or sleep issues, and any past appliance history. Also write down what worries you most. Pain, appearance, sleep, joint sounds, or fear of surgery each push the plan in different directions.
What is a good first goal
A good first goal is not “avoid surgery at all costs.” It's “understand the true source of the problem.” Once that becomes clear, the next step usually becomes much less overwhelming.
If you're dealing with jaw pain, facial tension, headaches, clenching, snoring, or sleep-related breathing concerns, Pain and Sleep Therapy Center offers a root-cause approach that looks beyond the bite alone. Their team focuses on TMJ function, airway health, oral posture, and non-surgical therapies that can help many patients find relief before considering invasive treatment.



