
You may be reading this after hearing a sentence that lands hard: “You don't have enough bone for regular implants.”
For many people, that moment comes after years of loose dentures, failing bridges, repeated repairs, or long stretches of avoiding photos and certain foods. Some have already gone through extractions, bone loss, or even prior implant work that didn't hold up. Others were ready to move forward, only to learn that the upper jaw no longer has enough structure for standard implants.
That's where zygomatic bone implants enter the conversation. They aren't a routine implant option. They're a specialized surgical solution designed for severe upper jaw bone loss, especially when conventional implants or graft-based plans may not be practical.
The challenge is that these implants are often presented as a simple “no-graft” shortcut. Sometimes they are the right answer. Sometimes they are not. The decision depends on anatomy, sinus health, surgical skill, prosthetic planning, and your goals for function, comfort, and long-term maintenance.
When Traditional Implants Are Not an Option
A patient sits down after a consultation and says, “I thought I was finally ready to fix this, and now I'm being told there's no bone left.” That reaction is common, and it's understandable.
Upper jaw bone can shrink significantly after tooth loss. Dentures can become less stable over time. Old implant sites can fail. Prior grafting may not have delivered enough usable bone. At that point, a patient may feel pushed toward a choice they don't want, either living with a removable denture or signing up for a long, staged reconstruction.
The moment patients often arrive at
Many people who ask about zygomatic bone implants are not starting from scratch. They've already been through a lot.
- Long-term denture wear: The denture worked at first, then gradually loosened as the upper jaw changed.
- Repeated dental failure: A bridge failed, teeth were lost, and the next recommendation became more complex than expected.
- A difficult consultation: They came in asking for implants and left hearing they may need extensive reconstruction first.
A patient in this situation may first read about approaches such as all on four dental implants Las Vegas and wonder why a similar solution won't work for them. The answer often comes down to anatomy. Some patients still have enough front-jaw bone for conventional full-arch treatment. Others don't, especially in the upper jaw.
A severe loss of upper jaw bone doesn't mean treatment is impossible. It means the treatment plan has to change.
Why this option exists
Zygomatic implants were developed for patients with severe maxillary bone loss who could not receive conventional implants. They anchor in the cheekbone rather than relying on the weakened upper jaw. That makes them relevant in some of the hardest implant cases, including bone loss after tooth loss, trauma, tumor surgery, or congenital deformity, as described in the medical literature at this clinical review.
That doesn't make them easy. It makes them purposeful.
For the right patient, they can open a door that seemed closed. For the wrong patient, or in the wrong hands, they can create a new set of problems. That balance matters.
What Are Zygomatic Implants and How Do They Work
A simple way to understand zygomatic implants is to think about hanging a heavy shelf. If the drywall is weak, you don't keep adding screws into soft material. You find the structural stud behind it.
That's the logic of zygomatic bone implants. When the upper jaw doesn't offer enough bone for regular implants, the surgeon uses the zygomatic bone, or cheekbone, as the anchor.
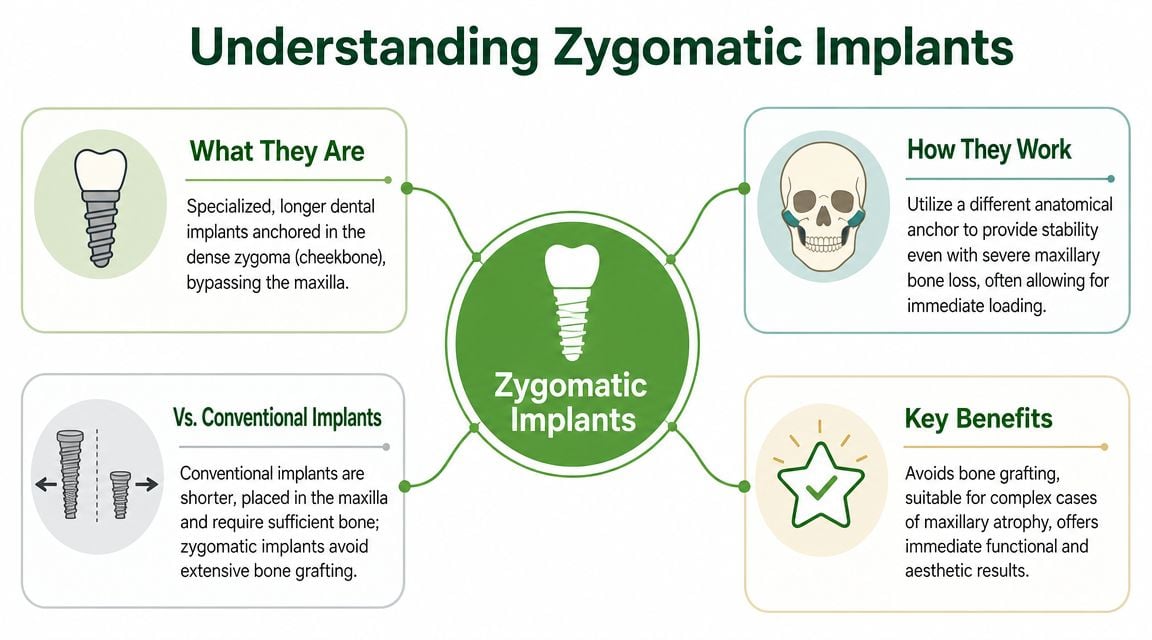
The anatomical difference
Standard implants are placed into the upper jawbone. Zygomatic implants follow a different path and engage the cheekbone instead. That matters because the zygomatic bone is highly dense. One clinical article describes it as having 98% density as a favorable site for implant placement, and the published literature commonly reports success in the 97% to 98% range worldwide for modern zygomatic protocols, according to Dimensions of Dental Hygiene.
That density is one reason these implants can support a fixed upper prosthesis in cases that would otherwise require major grafting.
Why they're different from regular implants
Zygomatic implants are not just “longer implants.” They represent a different surgical strategy.
They are used when the problem isn't minor bone thinning. They are used when the upper jaw has lost so much support that standard placement is no longer predictable.
Here's the practical difference:
| Feature | Conventional upper implants | Zygomatic implants |
|---|---|---|
| Anchor point | Upper jaw | Cheekbone |
| Main requirement | Enough jaw bone | Usable zygomatic bone and careful planning |
| Typical purpose | Routine implant replacement | Severe upper jaw bone loss |
| Common advantage | Familiar technique | May avoid extensive grafting |
How they support teeth
Once the implants engage the cheekbone, they can provide the foundation for a fixed upper restoration. In some cases, a full bridge can be stabilized with as few as four zygomatic implants, based on published clinical descriptions in the same article above.
Practical rule: If someone describes zygomatic implants as “the same as regular implants, just longer,” they're leaving out the most important part. The anatomy, planning, and risk profile are different.
Patients often get confused about whether this means the implant sits in the cheek. It doesn't work that way visually. The implant is placed internally along a planned trajectory so that the prosthetic teeth emerge in a usable position inside the mouth. The goal is a stable smile and bite, not a visible hardware change in the face.
Who Is an Ideal Candidate for Zygomatic Implants
The best candidate is more than “someone with bone loss.” The best candidate is someone whose upper jaw anatomy makes conventional implants unreliable, and whose overall condition supports a complex surgical reconstruction.
Patients who often qualify
These implants are most often considered in a narrow set of situations:
- Severely resorbed upper jaw: There isn't enough maxillary bone for conventional implants to be placed predictably.
- Failed prior treatment: Previous implants or grafting attempts didn't provide a stable path forward.
- Complex reconstruction needs: Bone loss followed trauma, tumor surgery, or congenital differences.
- Need to reduce grafting burden: The patient wants to avoid, or isn't a strong candidate for, a prolonged graft-based plan.
The Foundation for Oral Rehabilitation notes that a common pattern is one zygomatic implant per side combined with 2 to 4 conventional anterior implants, and that in fully resorbed maxillae the plan may expand to a Quad Zygoma design with four zygomatic fixtures. The same guidance states that zygomatic implants are suitable for two-stage and immediate loading, though they are usually immediately loaded with a fixed bridge, as outlined at the Foundation for Oral Rehabilitation.
Patients who need extra caution
At this point, decision-making gets more honest.
A patient may be technically eligible from a bone standpoint but still be a poor fit if sinus health is unstable, if there is active infection, or if the patient can't commit to follow-up and prosthetic maintenance. Referring doctors should also pause when the patient has ongoing facial pain, complicated airway issues, or a history that makes postoperative symptoms harder to interpret.
Questions about candidacy often overlap with broader implant planning. A patient trying to sort through the basics may benefit from reading are dental implants right for you, then bringing those questions into a specialist consultation focused on severe upper jaw loss.
A practical referral checklist
For patients and referring clinicians, these signs should trigger a zygomatic implant discussion:
- The upper denture has become progressively unstable.
- The patient has been told sinus lift or grafting would be extensive or uncertain.
- Prior implant or graft treatment in the upper jaw has failed.
- CBCT imaging suggests severe posterior maxillary deficiency.
- The patient wants fixed teeth, but standard full-arch planning won't reliably hold.
The ideal candidate isn't just someone who wants to skip grafting. It's someone whose anatomy and health make a zygomatic plan safer or more realistic than the alternatives.
The Zygomatic Implant Procedure from Start to Finish
Patients usually feel better once the process is broken into parts. This surgery is advanced, but the pathway is understandable.
A good zygomatic implant case starts long before the day of surgery. Planning is where much of the safety lives.
Planning the surgery
The surgeon studies the anatomy with CBCT-guided planning. That imaging helps map a precise path from the upper jaw toward the zygomatic bone while accounting for the sinus, orbit, and nearby nerves. Published procedural guidance describes zygomatic implants as typically 30–52 mm long and emphasizes that their trajectory must be carefully planned because they bypass deficient maxillary bone and engage the cheekbone through a very different path than standard implants, as summarized by American Dental Institute.
This is also where anesthesia planning matters. A case like this is not approached casually. Patients who are anxious about surgery often want to understand the difference between IV sedation, deeper sedation, and general anesthesia. A clear overview of oral surgery anesthesia options can help frame that discussion before the final surgical consult.
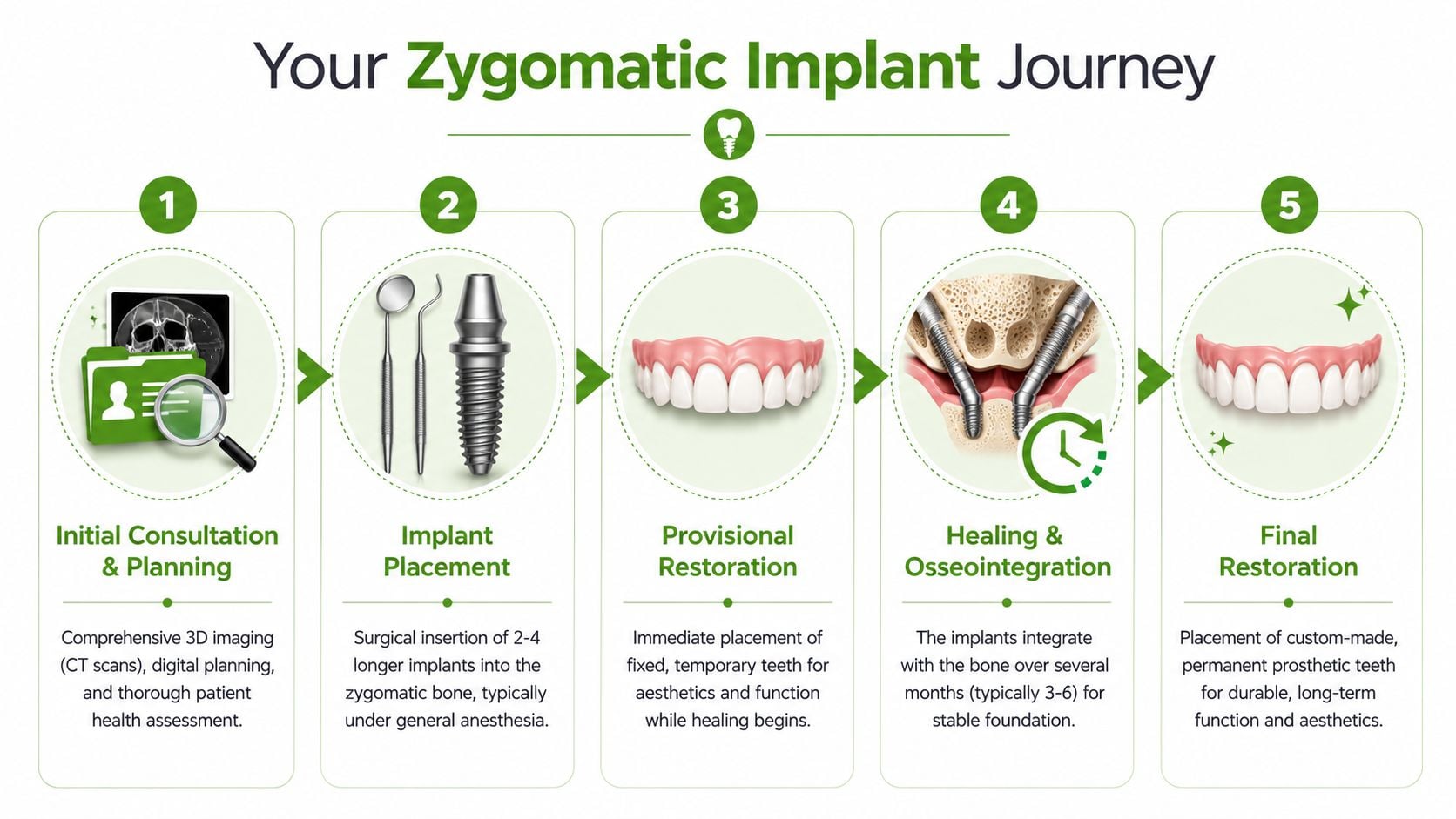
To help visualize the sequence, this overview is useful:
What happens on surgery day
The operation is performed by a surgeon with specific experience in this technique. After anesthesia is established, the implants are placed along the planned trajectory to achieve anchorage in the zygomatic bone.
The patient doesn't need to understand every drill sequence. What matters is the purpose. The surgeon is creating stable support where the upper jaw alone can't provide it.
A helpful video can make the sequence less abstract:
Immediate teeth and the healing phase
One major reason people pursue this option is the possibility of immediate loading. In plain terms, that means a fixed temporary bridge is often attached soon after surgery rather than waiting months with no teeth.
That benefit is real, but it can create confusion. “Immediate teeth” does not mean “fully healed.” It means you may leave surgery with fixed teeth in place while the implants integrate and the final prosthetic phase is completed later.
A typical timeline includes:
- Consultation and imaging: Detailed planning and risk review.
- Surgery: Placement of zygomatic implants, sometimes combined with anterior conventional implants.
- Provisional bridge: A fixed temporary restoration when the case is stable enough for immediate loading.
- Healing and review: Monitoring integration, soft tissue response, and sinus symptoms.
- Final restoration: Replacement of the provisional with the definitive prosthesis.
Patients often expect the hardest part to be the surgery. In reality, long-term success depends just as much on planning, prosthetic design, and disciplined follow-up.
Benefits of a Graftless Solution and Potential Risks
A patient with severe upper jaw bone loss often hears one phrase first: “You can avoid grafting.” That can be true, and it matters. Shorter treatment, fewer surgeries in some cases, and a faster path back to fixed teeth can change daily life in a meaningful way.
But “graftless” should be understood as a change in strategy, not a shortcut.
Zygomatic implants shift the source of support from weakened upper jaw bone to the cheekbone. For the right patient, that can avoid large bone grafts and staged sinus lift procedures. It can also open the door for people who have already been told they have “no bone” for traditional implants. Patients exploring average costs of dental implants and full-arch options often focus on price first, but the more important question is whether the anatomy supports a safer, more predictable plan.
Why a graftless plan can be attractive
The benefits are practical, not just promotional.
- Fewer surgical stages in selected cases: Some patients can avoid major graft reconstruction.
- Earlier fixed teeth: A provisional bridge may be possible soon after surgery when stability is strong enough.
- An option after severe bone loss: Treatment may still be possible even when standard upper implants are no longer realistic.
That said, a graftless plan does not mean a simple plan. It replaces one set of challenges with another. Instead of rebuilding bone and waiting for it to mature, the surgeon must place long implants through a demanding anatomical pathway and manage the prosthetic and sinus consequences carefully over time.
Understanding the actual risks
The main concern is not whether zygomatic implants are “good” or “bad.” The concern is whether they fit this patient's anatomy, medical history, sinus condition, and goals.
Complications reported in clinical practice include soft tissue irritation, prosthetic complications, cleaning difficulty around the restoration, and sinus-related problems. Sinusitis gets special attention for a reason. The implant pathway is close to the maxillary sinus, and even technically successful surgery can become frustrating if the patient later develops pressure, drainage, congestion, or recurrent infection.
This is one reason experienced teams avoid treating zygomatic implants as another version of full-arch treatment. They are a separate category of surgery with a different risk profile.
The sinus question should be front and center
For a patient with a history of chronic congestion, facial pressure, sleep-disordered breathing, or prior sinus disease, sinus health should shape the treatment plan from the beginning. A CBCT scan is not just for measuring bone. It is also used to study sinus anatomy, membrane condition, septa, drainage pathways, and any findings that could complicate healing.
Patients and referring doctors should ask:
- What does the sinus look like before surgery?
- Is there a history of sinusitis, allergy-related blockage, or prior sinus surgery?
- What surgical path is being planned in relation to the sinus?
- Who will evaluate and treat postoperative sinus symptoms if they appear?
- How will facial pain or pressure be distinguished from routine healing?
That conversation matters as much as the promise of same-day teeth.
For some patients, the best decision is still zygomatic implants. For others, staged grafting, another posterior support strategy, or even non-implant solutions for missing teeth may create a better balance of risk and long-term maintenance. The strongest treatment plans are usually the ones that make room for both possibilities.
Comparing Zygomatic Implants to Other Dental Solutions
Patients do better when they compare options by tradeoffs, not by slogans. Referring doctors do better when they match the treatment to the anatomy instead of defaulting to the latest full-arch label.
Some people need zygomatic implants. Some don't. Some are better served by grafting, standard full-arch treatment, or another posterior support strategy.
Zygomatic Implants vs. Alternative Full-Arch Solutions
| Solution | Ideal Candidate | Typical Treatment Time | Key Advantage | Primary Tradeoff |
|---|---|---|---|---|
| Zygomatic implants | Severe upper jaw bone loss with limited conventional support | Often shorter overall because grafting may be reduced or avoided | Can provide fixed support in extreme maxillary atrophy | High surgical complexity and important sinus considerations |
| Traditional implants with sinus lift or grafting | Patient with insufficient bone who can tolerate staged reconstruction | Longer because graft maturation is usually needed before final implant loading | Uses familiar conventional implant positions | More treatment stages and more healing time |
| Standard All-on-4 | Patient with enough available bone for angled conventional implants | Often streamlined when anatomy is favorable | Fixed full-arch option without the complexity of zygomatic anchorage | Not suitable when upper jaw bone loss is too advanced |
| Pterygoid implants | Selected posterior maxillary cases needing alternative anchorage | Varies by anatomy and overall prosthetic plan | May expand graftless options in skilled hands | Technique sensitive and not interchangeable with zygomatic planning |
The key decision point
The biggest mistake is treating all “teeth in a day” options as if they solve the same problem. They don't.
A patient exploring broader solutions for missing teeth may see full-arch implant terms grouped together, but the underlying questions are different. One plan depends on available front-jaw bone. Another depends on graft success. Zygomatic treatment depends on a surgeon's ability to use the cheekbone safely and on the patient's sinus status.
Peer-reviewed evidence also warns against assuming that bypassing grafting means bypassing risk. Published discussion of complications notes that sinusitis can be a significant complication and may be difficult to treat, underscoring that this is a specialist procedure rather than a simple shortcut, as discussed at this peer-reviewed article.
Cost and complexity are not the same thing
Patients often ask which route is “better.” That isn't the best question. A better question is which route is more appropriate for the anatomy, timeline, and risk tolerance.
Someone comparing pathways may also want a broader look at average cost of dental implants because treatment planning often involves balancing surgical complexity, prosthetic needs, and the number of stages involved. Cost matters, but it shouldn't be the only filter for a case this technical.
The best option is rarely the one with the shortest marketing message. It's the one that fits the anatomy and can be maintained over time.
Recovery, Aftercare, and Questions for Your Surgeon
Recovery after zygomatic implant surgery usually involves swelling, soreness, fatigue, and a temporary change in diet. Most patients expect that. What they often underestimate is how much healing depends on following instructions carefully and keeping postoperative review appointments.
What recovery usually involves
The early focus is protecting the surgical sites and the provisional bridge.
- Soft-food eating: You'll likely need a gentle diet while the implants and soft tissues settle.
- Sinus awareness: Sneezing, pressure, congestion, or unusual drainage should be reported rather than ignored.
- Careful hygiene: Cleaning around a full-arch prosthesis takes instruction and consistency.
- Scheduled follow-up: The team needs to monitor healing, fit, and any signs of sinus or soft tissue trouble.
Patients who have gone through major facial surgery sometimes find it helpful to review general principles from recovery after double jaw surgery. The procedures are different, but many of the recovery themes overlap, including swelling control, rest, diet progression, and respecting the healing timeline.
Three questions worth asking directly
Will my face shape or smile look different?
The goal is usually to restore support, lip position, and smile function, not to make your face look unnatural. Changes in prosthetic tooth position and upper lip support can affect appearance, so this should be reviewed during planning.
What are the long-term effects on my sinuses?
This is one of the most important questions. Ask how your sinus anatomy affects your case, what symptoms would be concerning later, and whether your surgeon works with ENT colleagues when needed.
How do I judge whether a surgeon is qualified for this?
Ask how often they perform zygomatic cases, how they plan them, how they manage complications, and who handles the prosthetic phase. You're not being difficult. You're asking the right questions for an advanced procedure.
If a consultation focuses heavily on speed and barely addresses sinus health, keep asking questions.
Good zygomatic implant care doesn't end when the bridge is delivered. It becomes an ongoing partnership between surgery, prosthetics, hygiene, and long-term surveillance.
If you're dealing with complex facial pain, jaw dysfunction, airway concerns, or questions about how sinus and oral structures affect treatment decisions, Pain and Sleep Therapy Center offers a root-cause approach that brings together expertise in TMJ disorders, facial pain, breathing, and oral function. Their team helps patients and referring providers think beyond isolated symptoms so treatment decisions support comfort, stability, and long-term health.



