
If you've just been told you need your wisdom teeth out, your first reaction probably wasn't calm curiosity. It was closer to, “How bad is this going to be?”
That's a normal question. Patients aren't worried about the technical name of the procedure. They want to know whether they'll be in pain, how long they'll be down, whether something can go wrong, and whether an already cranky jaw will get even worse.
Wisdom tooth removal is common, but common doesn't mean meaningless. One source notes that about 10 million wisdom teeth are extracted in the U.S. each year, with more than 30 million days of lost work or school and over $3 billion in annual procedural costs, which shows how routine the surgery is and how real the recovery burden can be at scale (wisdom tooth extraction burden in the U.S.).
The Moment You Hear You Need Your Wisdom Teeth Out
A conversation like this often happens fast. You go in for pain, swelling, crowding, or a routine exam. Someone points at the X-ray and says the wisdom teeth should come out. By the time you leave, you're trying to sort through fear, scheduling, cost, and all the stories you've heard from friends.
Some patients are mostly worried about pain. Others are worried about sedation, missing work, or what happens if their jaw already clicks, locks, or aches. If you tend to spiral after medical news, it can help to pause before reading horror stories and use a grounding resource on how to stop overthinking and worrying.
The next question I hear a lot is whether removal is automatically necessary. It isn't always. If you're trying to sort out the decision itself, not just the recovery, this guide on whether everyone needs wisdom teeth removed is a useful place to start.
What people usually mean by “how bad”
When individuals ask how bad wisdom teeth removal is, they're usually asking four different things at once:
- How much will it hurt
- How hard will recovery hit my normal routine
- What are the risks
- Will this aggravate my TMJ, jaw tension, or facial pain
Those are not the same question. A person with a simple erupted tooth and a healthy jaw may have a very manageable week. A person with deep impaction, clenching habits, and pre-existing TMJ symptoms may have a tougher recovery even if the surgery itself goes smoothly.
Wisdom teeth removal is often routine. It's still surgery, and surgery deserves realistic expectations.
A balanced starting point
The honest answer is that wisdom teeth removal is usually very manageable, but it's not trivial. The procedure itself is designed to be comfortable because pain control is built into it. The harder part is the recovery window, especially the first few days, and that recovery can affect chewing, sleep, jaw opening, and facial muscle tension.
For patients with TMJ problems, that last point matters a lot. Sometimes the extraction sites heal normally, but the jaw muscles and joints become the bigger story.
Understanding the Pain During and After the Procedure
Patients don't feel pain during the actual removal. They feel pressure, tugging, vibration, and movement. That's very different from feeling sharp pain.

During the procedure
Your surgeon may use local anesthesia alone, local anesthesia with sedation, or a deeper anesthetic approach depending on the case and your health history. The purpose is the same. You shouldn't be sitting there feeling the tooth being cut out.
That distinction matters because people often picture the surgery itself as the worst part. In reality, the procedure is usually the controlled part. The body's inflammatory response afterward is what creates soreness, stiffness, swelling, and difficulty chewing.
Practical rule: Expect pressure during surgery, not pain. Expect soreness after surgery, not constant agony.
After the procedure
Post-operative pain is more like recovery from a minor oral surgery than a simple loose-tooth extraction. If the tooth was impacted or sectioned into pieces, the tissues around it have been stretched, cut, and manipulated. That creates a predictable healing response.
One patient-friendly source notes that the first 2 to 3 days are typically the most uncomfortable, with substantial improvement after that, and that full healing can take up to two weeks (typical discomfort and healing timeline). That matches what many patients experience. The burden is concentrated early, then it usually eases.
What helps and what doesn't
Pain control works best when patients treat it as a schedule, not a rescue mission after pain escalates. Your surgeon may recommend prescription medication, over-the-counter options, or both. This overview of medication for wisdom tooth extraction can help you understand the usual categories and why timing matters.
A few practical points usually make the biggest difference:
- Stay ahead of pain early by taking medications exactly as instructed
- Use cold packs in the early window if your surgeon recommends them
- Protect the blood clot by avoiding aggressive spitting, smoking, and straws
- Eat soft foods before you get overly hungry, because chewing can be tiring
What doesn't work well is trying to “tough it out” for hours, then chasing severe pain after the anesthetic has fully worn off. That approach often makes the first night harder than it needs to be.
Key Factors That Determine Your Recovery Severity
Two people can both say they had their wisdom teeth removed and mean very different procedures. One had a fully erupted tooth lifted out in a straightforward extraction. Another had an extensively buried tooth near important structures that required a surgical approach. Their recoveries won't look the same.

The anatomy matters
The biggest driver of recovery is often how difficult the tooth is to access and remove. Deep impactions usually require more tissue manipulation than erupted teeth. Roots that curve or sit close to important anatomy can make the surgery more delicate. Position matters too. A tooth angled awkwardly in the jaw often creates a different surgical challenge than one that's upright.
Expert surgical guidance notes that risks such as injury to the lingual or inferior alveolar nerve, and in rare cases jaw fracture, increase when impactions are deep, roots are near nerves, or the patient is older because denser bone makes removal more mechanically difficult (surgical factors that increase extraction risk).
Why age changes the experience
Older patients often ask why their surgeon sounds more cautious than when a teenager gets the same recommendation. The answer is mechanical. Bone tends to become denser with age, roots may be more fully formed, and the surrounding tissues may not forgive surgical stress as quickly.
That doesn't mean adults can't do well. They often do. It means the procedure may be less forgiving, and soreness or jaw stiffness may last longer.
A simple comparison
| Situation | What recovery often feels like |
|---|---|
| Erupted tooth with easy access | More local soreness, easier mouth opening, faster return to normal chewing |
| Soft tissue impaction | Noticeable swelling and tenderness, but often manageable with standard aftercare |
| Full bony impaction or awkward root position | More swelling, more stiffness, more need for rest and jaw protection |
Other variables patients feel right away
Some factors don't change the surgical plan much, but they change how recovery feels in real life:
- How many teeth are removed at once can affect eating and sleeping because more areas are sore.
- Your baseline pain system matters. People with migraines, facial pain, or clenching often feel recovery more intensely.
- Your stress level matters too. Anxious patients often carry more muscle tension in the jaw, neck, and temples before surgery even starts.
The X-ray doesn't just show teeth. It often explains why one person says recovery was “no big deal” and another says it took over their week.
The Connection Between Wisdom Teeth Removal and TMJ Pain
This is the part many general articles skip. The extraction sites can be healing normally while the jaw joint and chewing muscles are miserable.
Why the jaw can flare after surgery
To remove wisdom teeth, the mouth has to stay open for a sustained period. For some patients that's just uncomfortable. For others, especially people with a history of clicking, locking, clenching, headaches, or facial muscle tenderness, it can overload the temporomandibular joint and the surrounding muscles.
That strain can show up as aching in front of the ears, temple headaches, limited opening, painful chewing, or a sense that the bite feels “off” because the muscles are guarding. Post-operative swelling can add to it. When the body protects an irritated area, the chewing muscles often tighten, and that tightness can spread into the face, scalp, and neck.
Who needs to mention TMJ history before surgery
Tell your oral surgeon if you have any of these before the procedure:
- Jaw clicking or popping
- Episodes of locking
- Pain with wide opening
- Morning jaw soreness from clenching
- Frequent temple headaches or facial muscle pain
That information changes planning. Your team may be more careful about jaw positioning, more attentive to post-op muscle guarding, and more realistic with you about what kind of soreness is from the extraction versus the joint and muscles.
What TMJ-related pain feels like after extraction
Extraction pain is usually localized to the surgical area. TMJ or myofascial pain tends to feel broader. Patients often describe it as fatigue in the jaw, pain near the ears, headache, a pulling sensation into the cheeks, or trouble opening fully even when the extraction site itself looks acceptable.
If you're trying to sort out those patterns, this overview on understanding TMJ issues gives a helpful plain-language explanation of how the joint and surrounding muscles behave.
When a patient says, “My teeth are out but my whole jaw hurts,” I don't assume something went wrong. I first think about muscle guarding, joint strain, and limited jaw motion after a prolonged opening procedure.
What usually helps TMJ patients recover better
The key is not forcing the jaw. Gentle, progressive return to motion tends to work better than repeated wide opening to “test” it. Soft foods, heat or cold as directed, medication as prescribed, and conscious relaxation of clenching are usually more useful than chewing through pain.
For some patients, the hardest part isn't the socket. It's sleeping with a tense jaw and waking up sore from overnight clenching while the tissues are still inflamed.
Your Typical Recovery Timeline and Aftercare Plan
A good recovery plan is less about heroics and more about rhythm. Rest, pain control, swelling control, gentle hygiene, and protecting the extraction sites help ensure a successful recovery.
Start with the broad view:
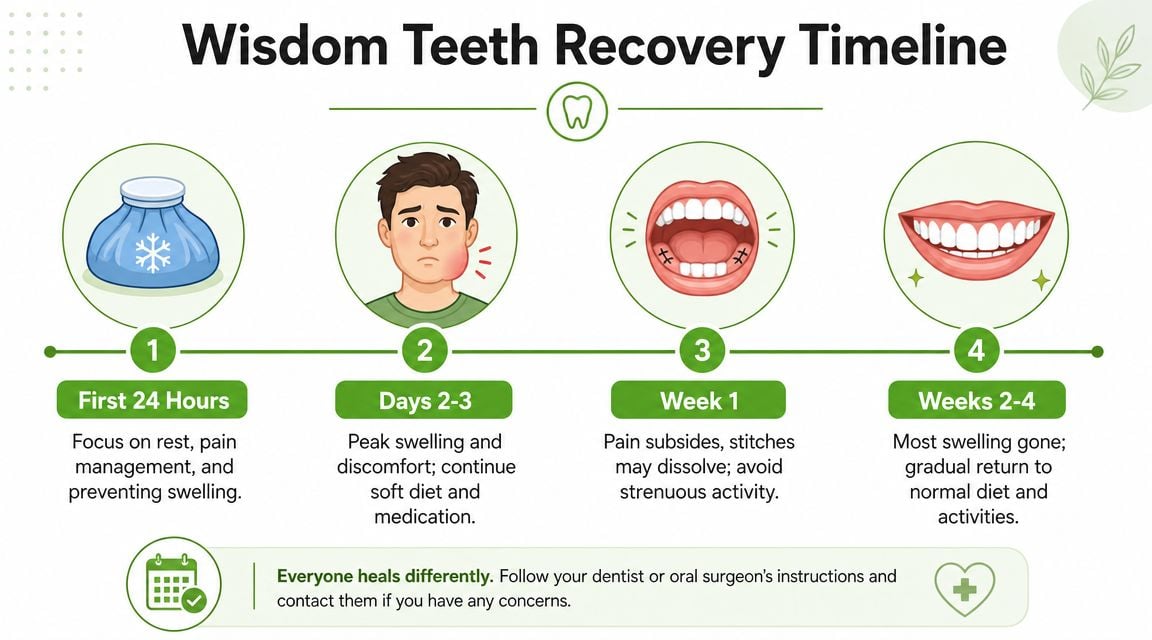
First day
The first day is about control, not productivity. You want bleeding to settle, numbness to wear off safely, and pain medication to start working before discomfort builds.
Focus on these basics:
- Rest with your head propped up if your surgeon advises it
- Use gauze as instructed and don't keep changing it obsessively
- Stick to cool or lukewarm soft foods
- Avoid smoking, straws, and forceful rinsing
The biggest mistake on day one is doing too much because you feel okay while still numb.
A visual walk-through can help if you like step-by-step recovery explanations:
Days two and three
This is often the rough patch. Swelling and stiffness usually become more obvious, and many patients notice that chewing and talking feel tiring. If you also have TMJ symptoms, this is often when the muscles start complaining.
A practical menu helps more than generic “eat soft foods” advice. Think yogurt, applesauce, mashed potatoes, scrambled eggs, smoothies eaten by spoon, oatmeal once tolerated, and soups that aren't too hot. The right diet is the one that lets you nourish yourself without forcing wide opening or heavy chewing.
Your job for these days is simple. Keep inflammation calm, keep the area clean, and don't test your limits.
Days four through seven
Patients often start turning the corner here. Pain usually shifts from sharp soreness to tenderness and stiffness. Jaw opening may still feel limited, especially in patients who clench or have pre-existing TMJ issues.
Helpful habits in this phase include:
- Continue gentle oral hygiene exactly as instructed
- Add movement gradually instead of trying to yawn wide or chew tough foods
- Return to work or school based on function, not just determination
- Watch for delayed worsening, because that's different from slow improvement
For infection prevention and general hygiene awareness, a plain-language public health read like BacteriaFAQ on staph prevention can reinforce the broader principle that clean hands, clean habits, and avoiding contamination matter during healing.
Week two and beyond
By this point, many people are functioning much better even if the tissues are not fully settled. Normal eating often returns gradually, not all at once. If the extraction sites are doing well but the jaw still feels off, the issue may be residual muscle guarding rather than the teeth themselves.
In that situation, targeted support can be useful. Pain and Sleep Therapy Center evaluates TMJ-related jaw dysfunction, facial pain, and muscle tension patterns that may linger after dental procedures, which can help patients distinguish socket healing from a separate jaw mechanics problem.
Recognizing Complications and When to Call Your Doctor
Most recoveries are straightforward. Still, wisdom tooth removal has a real complication profile, and patients do better when they know what deserves attention.
A major review found 101 complications in 1,202 extractions, an overall rate of 8.4%, with dry socket at 4.2%, temporary sensation disorders at 1.0%, persistent sensation disorders at 0.5%, abscesses at 1.25%, and post-operative bleeding at 0.4%. A later clinical study reported a 10.0% postoperative complication rate, including dry socket at 3.2%, inferior alveolar nerve injury at 1.7%, wound infection at 1.4%, and lingual nerve injury at 0.2%, supporting the practical takeaway that overall complication rates are around 8% to 10% and usually involve pain, infection, or nerve symptoms rather than catastrophic events (systematic review of wisdom tooth extraction complications).
The three problems patients most often miss
Dry socket usually isn't “a little extra soreness.” It tends to feel like pain that intensifies instead of easing, often with a deep, radiating quality.
Infection may show up as increasing swelling, foul taste, drainage, or worsening pain after a period when you expected improvement.
Persistent numbness or tingling in the lip, chin, or tongue deserves prompt follow-up, especially if it isn't fading.
If you want more context on nerve-related symptoms after dental treatment, this page on trigeminal nerve pain after dental work can help you understand why altered sensation shouldn't just be ignored.
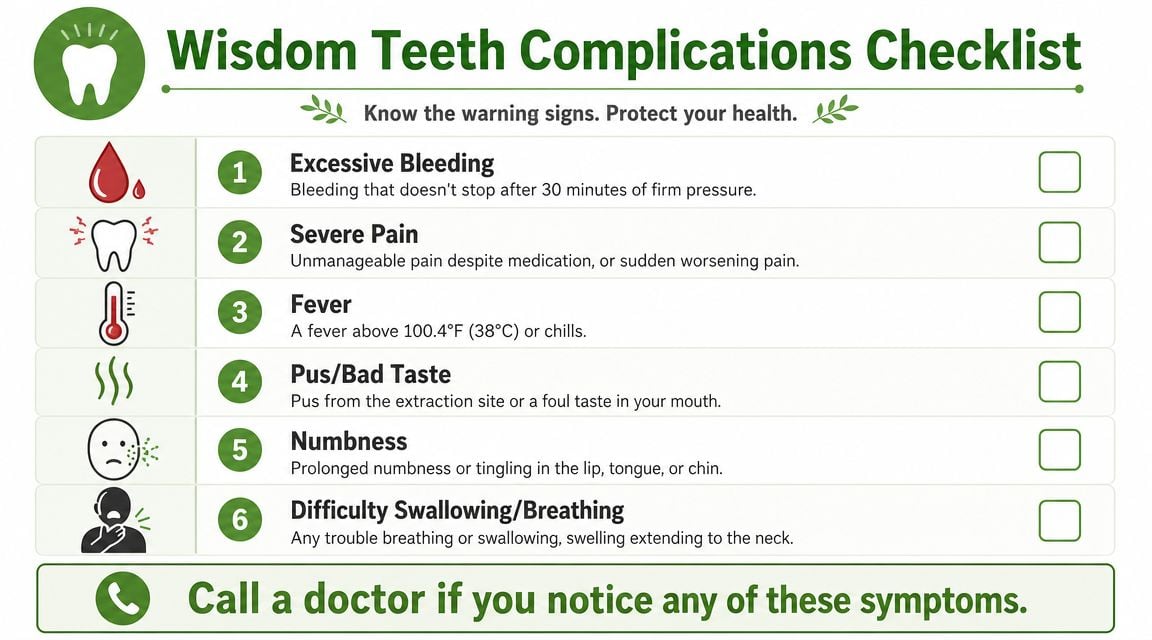
When I'd tell a patient to call
Call your surgeon promptly if you notice any of the following:
- Pain that worsens instead of improves
- Bad taste, drainage, or signs that concern you for infection
- Bleeding that doesn't settle with the instructions you were given
- Numbness, tingling, or altered feeling that persists
- Trouble swallowing, breathing, or swelling that seems to spread
If something feels significantly worse than the written recovery instructions prepared you for, contact the office. It's better to ask early than to wait and guess.
The safest mindset is simple. Respect the procedure, follow the aftercare plan, and don't normalize red flags just because someone told you wisdom tooth removal is “routine.”
If wisdom teeth removal has left you with lingering jaw pain, facial muscle tension, headaches, or TMJ symptoms that don't fit a normal healing pattern, Pain and Sleep Therapy Center offers evaluation for TMJ disorders, orofacial pain, and jaw dysfunction. For patients in Charlotte and surrounding areas, that can be a useful next step when the extraction sites may be healing but the jaw still isn't functioning comfortably.



