
You may be reading this because bedtime has changed in a way you can't ignore. You lie down, and within minutes you feel chest pressure, air hunger, or an urge to sit up. Maybe you've started stacking pillows without thinking much about it. Maybe two pillows now feel necessary, not optional.
That pattern has a medical name. 2 pillow orthopnea means you're short of breath when you lie flat, but you breathe more comfortably once your upper body is raised on two pillows. That sounds simple, but clinically it matters. It's often a clue that your body isn't handling lying flat the way it should.
As a sleep and pain specialist, I'd frame this clearly and calmly. Pillows can help symptoms. They don't explain the cause. The important question isn't just “What pillow should I use?” It's “Why can't I breathe comfortably flat anymore?”
Why "How Many Pillows?" Is a Critical Health Question
A lot of patients assume pillow count is just a comfort preference. In medicine, it often isn't. When a clinician asks how many pillows you need to sleep, they're trying to understand whether lying flat changes your breathing in a meaningful way.
Orthopnea is shortness of breath in the recumbent position that improves when you sit or stand up, as described in the NCBI clinical reference on dyspnea and orthopnea. That same reference notes that asking about pillow count is part of the standard history because it works as a practical severity marker.
Why two pillows matters
If someone says, “I'm fine as long as I sleep on two pillows,” that tells me the body needs some degree of elevation to reduce breathing difficulty. It doesn't make the problem dramatic by itself, but it does make it real.
Needing one or two pillows can fit with earlier or milder symptoms. Needing to sleep upright is more concerning. The key point is that 2 pillow orthopnea is not just a bedtime habit. It's a bedside clue that deserves context.
Practical rule: If your pillow needs changed because your breathing changed, treat that as a health signal, not just a sleep setup problem.
What patients often notice first
The sensation varies. Some people describe it as chest heaviness. Others say they “can't get a deep breath” once they're flat. Some notice they drift off, then wake and shift upward. Many don't use the word shortness of breath at all. They say, “I sleep better propped up.”
That's one reason this symptom gets missed. People often focus on bedding first. And yes, comfort matters. If you're also trying to find your perfect pillow, that can help support your neck and upper body. But when pillow stacking becomes necessary for breathing, it's time to think beyond comfort and look for the reason.
A second pillow can be a temporary workaround. It should not become the end of the conversation.
What Happens in Your Body When You Lie Down
When you stand or sit upright, gravity helps keep more fluid pooled in the lower body. When you lie flat, that fluid redistributes toward the torso. In a healthy system, the heart and lungs usually handle that shift without much trouble. In someone with reduced cardiac reserve or another breathing problem, that extra volume can create a kind of fluid traffic jam in the chest.
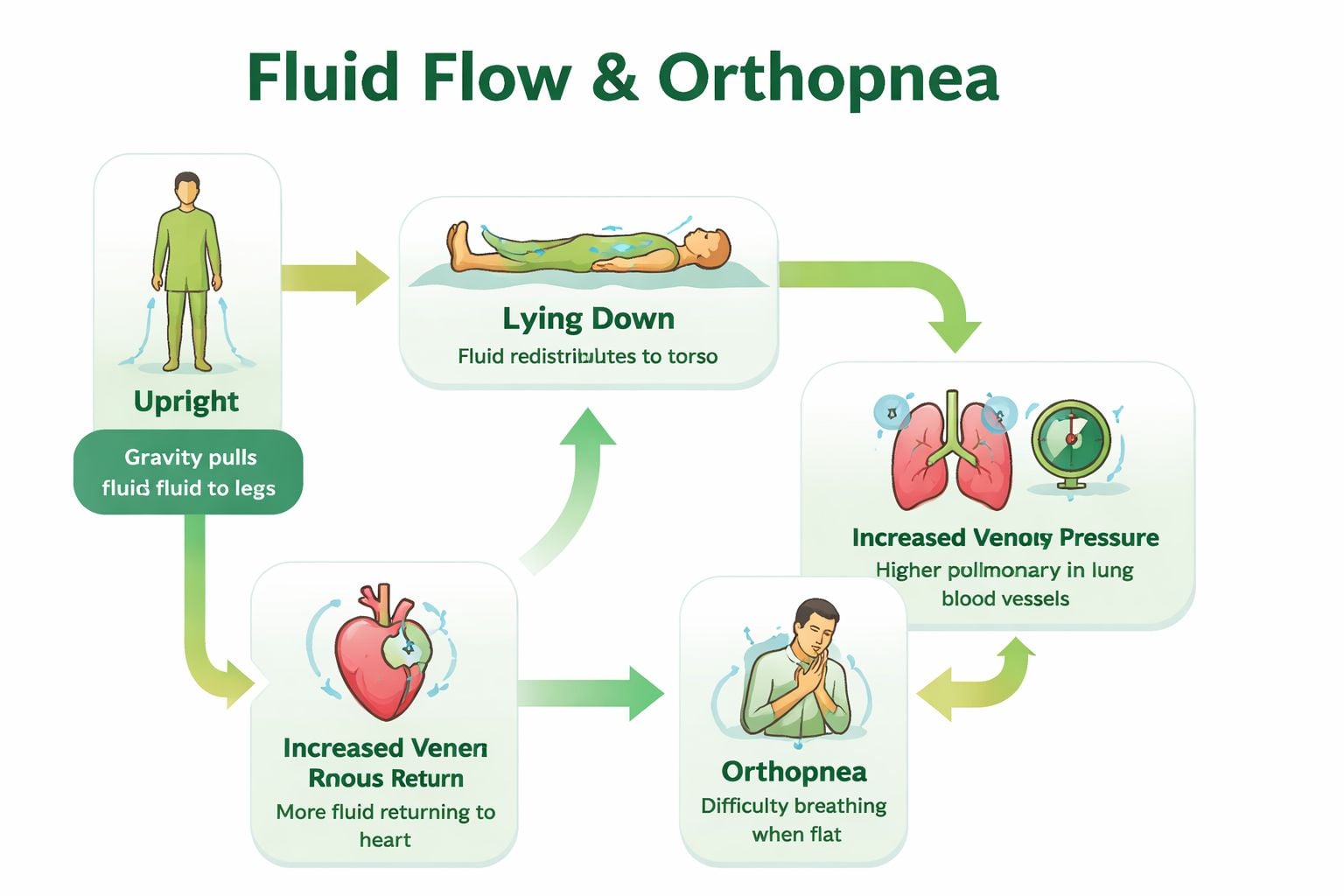
The NCBI reference describes “2 pillow orthopnea” as a clinical way of describing orthopnea that is mild enough to be controlled by sleeping propped up on two pillows, and explains that when a person lies flat, blood volume shifts from the legs and abdomen toward the lungs, which can contribute to pulmonary congestion and breathlessness in people with impaired cardiac function. That's why clinicians ask about pillows at night in the first place.
The fluid traffic jam idea
Think of the lungs and heart as a roadway that already has limited capacity. Lying flat sends more traffic into that space. If the system is already strained, pressure rises, the lungs become less comfortable to expand, and breathing starts to feel labored.
That's also why sitting up helps. Elevation changes the mechanics. It reduces how much fluid shifts into the chest and can make breathing feel less effortful.
Why pillows help, but only partly
Pillows don't treat the underlying condition. They change body position enough to reduce symptoms. In practical terms, they open the chest a bit, reduce the pressure effect of lying fully flat, and make ventilation easier.
For some patients, the sensation overlaps with what people call air hunger. If that term feels familiar, this explanation of air hunger symptoms may help you put language to what you're feeling.
The relief you get from propping up is useful information. It tells us position matters. Then we need to ask why position matters so much for you.
Heart, Lungs, or Something Else? Key Causes
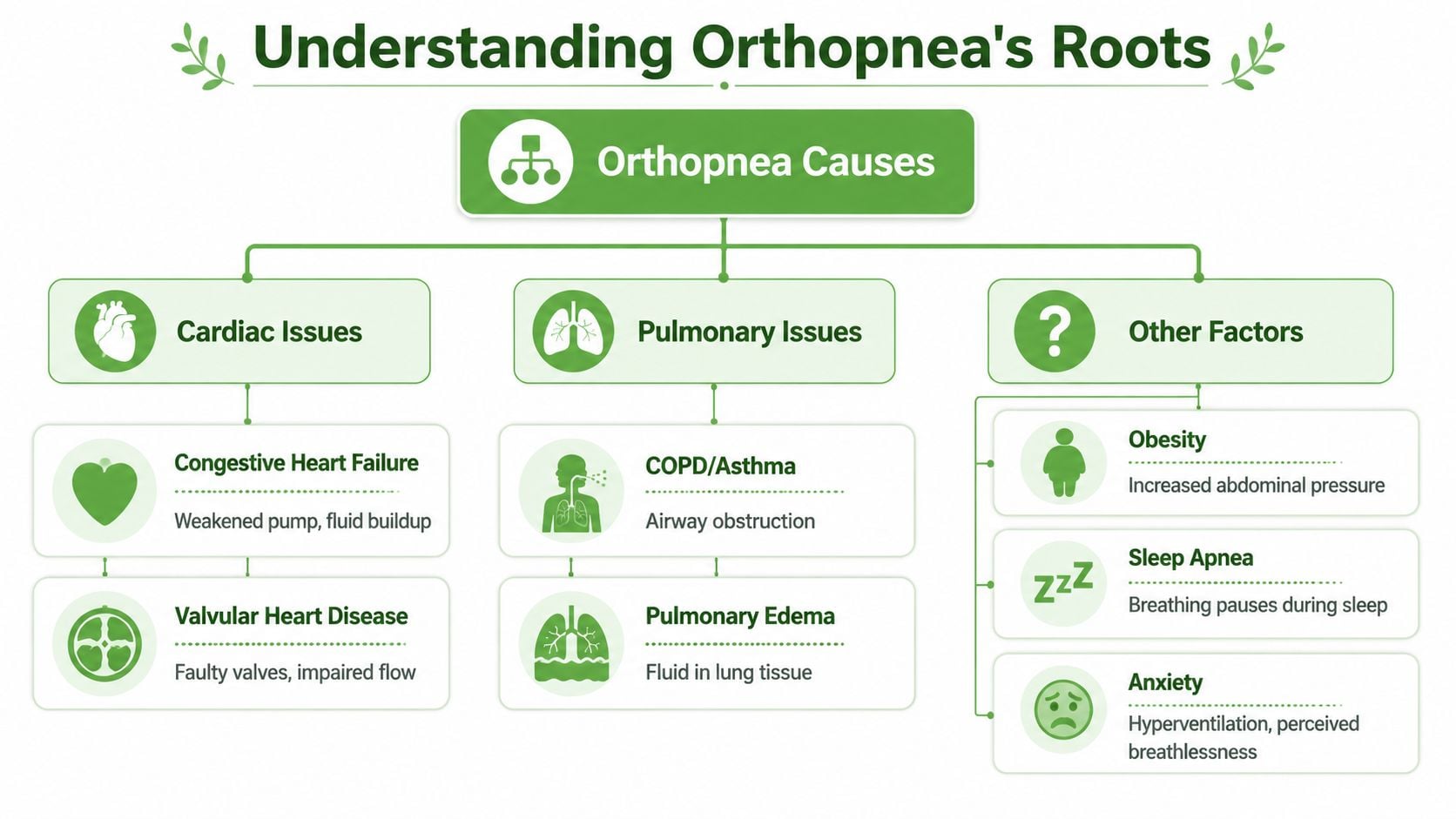
Historically, orthopnea has been tied most strongly to heart failure, but current clinical guidance also recognizes pulmonary disease, obesity, and sleep-related breathing disorders as possible causes. A plain-language overview from Healthline's orthopnea guide notes that if someone can no longer lie flat comfortably and needs two pillows, clinicians consider fluid overload, heart failure, pulmonary disease, obesity, or sleep-related breathing disorders and investigate further.
The common buckets
Some causes are classic. Others are under-discussed.
| Condition | How it Causes Orthopnea | Other Common Symptoms |
|---|---|---|
| Heart failure | Lying flat can worsen congestion in the chest and make breathing harder | Swelling, fatigue, waking short of breath |
| Pulmonary edema | Fluid in lung tissue interferes with comfortable breathing when recumbent | Cough, chest heaviness, breathlessness |
| COPD or other chronic lung disease | Reduced respiratory reserve makes flat positioning harder to tolerate | Wheeze, cough, exertional shortness of breath |
| Obesity | Extra abdominal and chest wall loading can limit diaphragmatic movement when lying down | Snoring, reflux, nonrestorative sleep |
| Obstructive sleep apnea | Airway narrowing or collapse can make breathing more unstable in sleep, especially in certain positions | Loud snoring, witnessed pauses, dry mouth, daytime sleepiness |
| Sleep-related breathing dysfunction beyond classic OSA | Nasal obstruction, poor airway mechanics, or abnormal breathing patterns can make recumbency feel worse | Mouth breathing, fragmented sleep, morning headaches |
The overlooked sleep connection
Many patients often receive partial answers. They're advised to sleep in a raised position, and that may help. But if the person also snores, mouth breathes, wakes unrefreshed, or feels worse on their back, obstructive sleep apnea or compromised airway function may be part of the picture.
That doesn't mean every person with 2 pillow orthopnea has sleep apnea. It means the overlap is clinically important. Position changes can reduce symptoms from more than one mechanism at the same time. A patient may be easing recumbent breathlessness, reducing snoring intensity, and improving reflux pressure, all with the same stack of pillows. That can mask how significant the underlying issue really is.
If those patterns sound familiar, a review of sleep apnea causes and symptoms can help you identify whether your nighttime breathing fits a broader airway problem.
If you need elevation to sleep and also have snoring, frequent waking, or daytime fatigue, don't assume it's “just how you sleep.”
The Diagnostic Journey From Symptom to Solution
When a patient reports 2 pillow orthopnea, I don't jump straight to one cause. I build the story first. The symptom matters, but the pattern around it matters just as much.
A medical dictionary entry on two-pillow orthopnea describes it as a clinically useful severity marker and notes that clinicians are explicitly advised to ask how many pillows a patient needs at night because the number helps gauge severity and functional limitation.
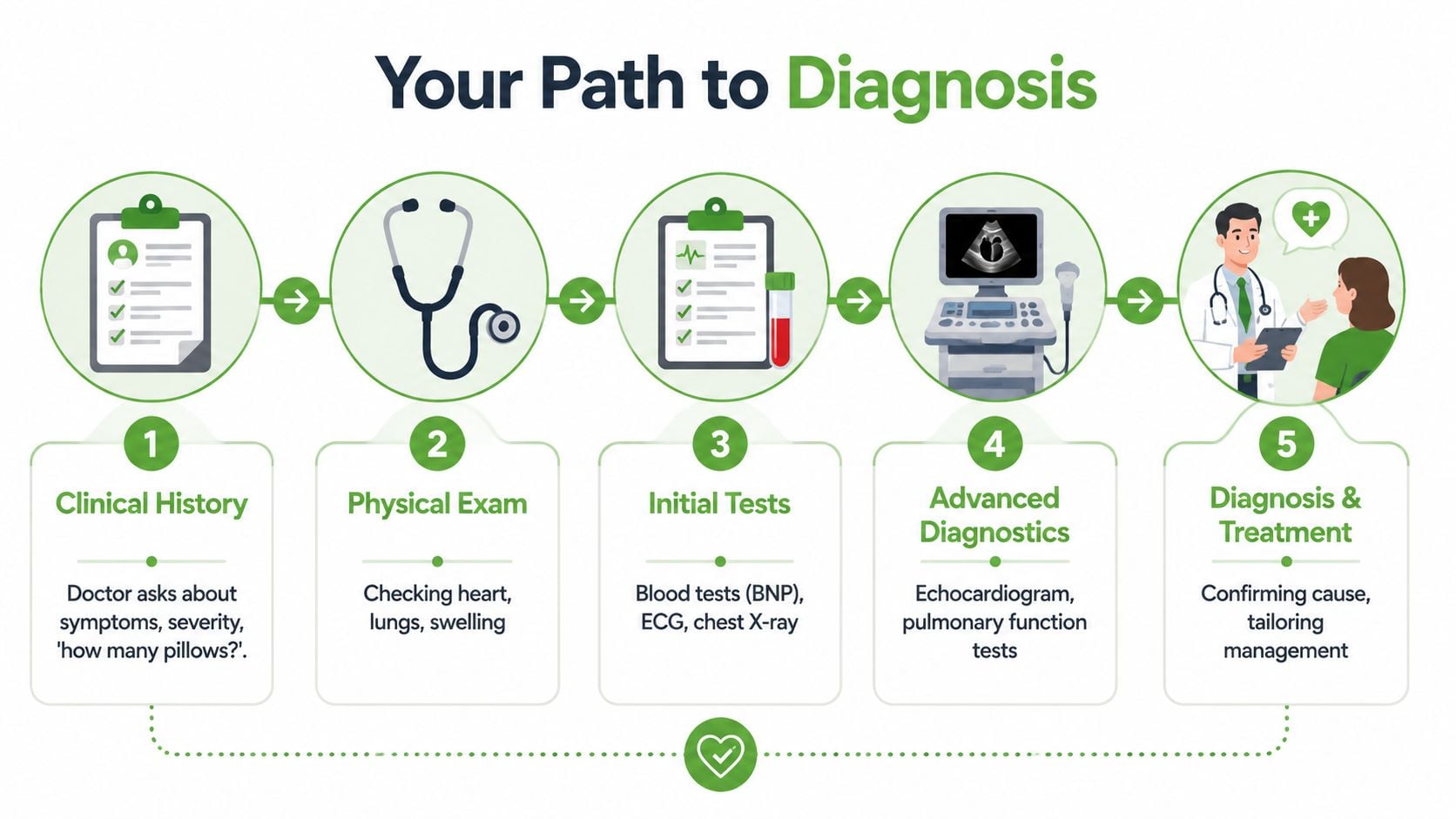
Step one is the conversation
The questions are usually straightforward:
- When did this start? A new symptom has a different meaning than a long-standing pattern.
- Is it only when you lie flat? That helps distinguish position-related breathing difficulty from constant shortness of breath.
- Has your pillow count increased? That can suggest change over time.
- Do you snore, gasp, or wake often? Those details raise the possibility of sleep-disordered breathing.
- Do you have swelling, cough, chest symptoms, or exercise intolerance? Those clues point toward heart or lung causes.
Step two is the exam
A clinician may listen to the lungs and heart, check for leg swelling, assess breathing effort, and look at nasal and oral airway features if sleep breathing issues seem possible.
In an airway-focused evaluation, I also want to know how you breathe during the day. Nasal breathing, mouth posture, tongue position, and jaw structure can all affect sleep-related airflow. Those findings don't replace a medical workup for cardiac or pulmonary disease, but they can sharpen the picture.
Step three is targeted testing
Testing depends on the history and exam. A primary care doctor, cardiologist, pulmonologist, or sleep specialist may order studies based on the most likely cause.
Common next steps can include:
- Cardiac evaluation: ECG, chest imaging, and echocardiography when heart-related causes are suspected
- Pulmonary evaluation: lung testing or imaging if chronic lung disease is in the differential
- Sleep evaluation: home or lab-based testing when symptoms suggest sleep apnea or another sleep-breathing disorder
If the airway side of the story stands out, information about how to diagnose sleep apnea at home can help you understand what that process looks like.
A good workup doesn't stop at “sleeping propped up.” It identifies the driver.
Practical Tips for More Comfortable Sleep
The goal at night is simple: breathe with less effort while you wait for the medical workup to identify why lying flat is a problem. Comfort matters, but the setup should also avoid creating new strain in the neck, jaw, or upper back.

A consumer sleep resource from Sleep Foundation on orthopnea explains why head and torso support can help. A more upright position can reduce the discomfort some people feel after lying down, but symptom relief still needs to be paired with diagnosis. That is especially true when the pattern may involve more than the heart or lungs alone. In practice, I also consider obstructive sleep apnea, nasal blockage, mouth breathing, and other airway limitations that can make a flat position feel immediately harder.
What usually works better than stacking loose pillows
Pillow piles often fail for mechanical reasons. They slide apart, push the chin toward the chest, and support the head more than the rib cage. Many patients sleep better with a setup that raises the upper body as one unit.
- A wedge pillow: This often gives a steadier incline than two or three standard pillows.
- An adjustable bed: This can raise the chest and head together and reduce awkward neck flexion. If you are comparing options, these DME Superstore insights on beds give a practical overview of adjustable-bed features.
- Side sleeping, if comfortable: Some people with sleep-disordered breathing notice less airway collapse on their side than on their back.
- Nasal airflow support: If one side of the nose is blocked, or you rely on mouth breathing at night, that deserves attention. A more upright position may help temporarily, but it does not correct the airflow problem itself.
Common mistakes that make sleep harder
Small adjustments can help. Poor positioning can also leave you sore and still short of breath.
- Using too many soft pillows: This often bends the neck sharply without raising the chest enough.
- Choosing a setup you cannot maintain all night: If the position collapses after an hour, it is not doing its job.
- Ignoring clues beyond bedtime: Breathlessness with activity, swelling, cough, loud snoring, witnessed pauses in breathing, or waking with a dry mouth all add useful diagnostic information.
- Treating pillow height as the answer: Needing more support over time can signal progression of the underlying problem.
Here's a useful overview of sleep positioning concepts:
Comfort measures that support the bigger plan
Keep the bedtime setup consistent for several nights so you can notice whether symptoms are stable, improving, or getting worse. That pattern helps your clinician far more than a vague report that you are "using extra pillows."
Do not force yourself to lie flat just to prove you can do it. If a position reliably makes breathing worse, avoid it.
It also helps to notice what kind of discomfort wakes you up. A sensation of chest heaviness, coughing, wheezing, congestion, choking, snoring, or abrupt gasping can point in different directions. That distinction matters because two-pillow orthopnea is not always only a fluid issue. In some patients, the airway is part of the story.
Elevation can improve comfort for the night. It does not identify or fix the cause.
Your Next Steps and When to See a Specialist
If 2 pillow orthopnea is new, worsening, or paired with other symptoms, see your doctor. That is the right next step. Pillow elevation can help, but the Cleveland Clinic overview of orthopnea warns that new or worsening orthopnea should trigger a cardiac or pulmonary workup, especially because elevating the head can also be a sign of sleep-disordered breathing.
When it's urgent
Get urgent medical attention if you have any of the following with trouble breathing when lying down:
- Chest pain: especially if it's new or concerning
- Severe shortness of breath at rest: not just when fully flat
- Bluish lips or marked distress: any sign you're struggling to oxygenate
- Rapid worsening: especially over a short period
- Confusion, faintness, or inability to speak comfortably: those are not routine symptoms
Which specialist makes sense
Different patterns point in different directions.
A primary care clinician is often the best first stop because they can sort out whether your symptom pattern looks more cardiac, pulmonary, sleep-related, or mixed.
A cardiologist becomes especially important if there are signs of fluid overload, exercise intolerance, swelling, or concern for heart failure.
A pulmonologist is a good fit when chronic lung disease, wheezing, cough, or another respiratory problem seems likely.
A sleep medicine specialist matters when the nighttime story includes snoring, gasping, mouth breathing, nonrestorative sleep, morning headaches, or positional breathing changes that suggest obstructive sleep apnea or another airway problem.
The decision I want patients to make
Don't judge this symptom only by how well two pillows fix it. Judge it by what it may be telling you. Breathing comfortably flat is generally something one should be able to do. If you can't, your body is giving you information.
You don't need to panic. You do need to follow the clue.
If you're dealing with nighttime breathlessness, snoring, mouth breathing, or suspected sleep apnea, Pain and Sleep Therapy Center offers evaluation for sleep-related breathing issues and airway-focused care aimed at identifying the root cause behind disrupted sleep.



