
You wake up with an ache near your jaw. By lunch, it feels like pressure under your cheekbone. By evening, a quick stab shoots toward your ear when you chew. Then someone tells you it’s probably your teeth, someone else says sinus pressure, and another person wonders if it’s stress.
That confusion is common. Facial pain rarely stays in one neat box.
As a specialist, I can tell you that facial pain is less like a single condition and more like a message. Your body is signaling that something in the system is irritated, inflamed, overloaded, or not working the way it should. The challenge is that the face is packed with joints, muscles, teeth, nerves, airways, and sinuses that sit very close together. When one part struggles, another part often feels it.
Your Guide to Understanding Facial Pain
Many patients arrive feeling worn down, not just by the pain itself, but by the uncertainty around it. They’ve tried ibuprofen, changed pillows, seen a dentist, maybe even taken antibiotics, yet the pain keeps shifting or returning. That experience can make you wonder if the pain is “real enough” or if you’re somehow missing something obvious.
You’re not missing it. Facial pain is genuinely complex.
One person may describe a dull pressure in the cheeks that turns out to be jaw muscle strain. Another may feel lightning-like pain near the lip or chin that points toward nerve irritation. A third person may think they have a sinus problem, when the underlying issue starts with clenching at night or an unstable bite pattern. The location of the pain doesn’t always reveal the source.
Facial pain often behaves like a false address. The pain shows up in one place, but the cause may live somewhere else.
That’s why “what causes facial pain” isn’t a simple question. The answer can involve the jaw joint, the muscles of chewing, dental problems, sinus pressure, headaches, or the trigeminal nerve, which carries sensation across much of the face. In some people, the missing piece is even more overlooked, such as airway strain, poor oral posture, or clenching tied to sleep-disordered breathing.
A better approach starts with patterns.
- When does it happen. During chewing, on waking, in cold air, after stress, or with light touch?
- What does it feel like. Pressure, burning, stabbing, throbbing, tightness, or electric shocks?
- Where does it spread. Jaw to temple, tooth to ear, cheek to eye, or one side only?
- What else comes with it. Clicking, popping, headaches, congestion, dry mouth, numbness, or sleep issues?
Those details turn a vague symptom into a trail of clues. Once you understand the categories, the problem becomes much less mysterious.
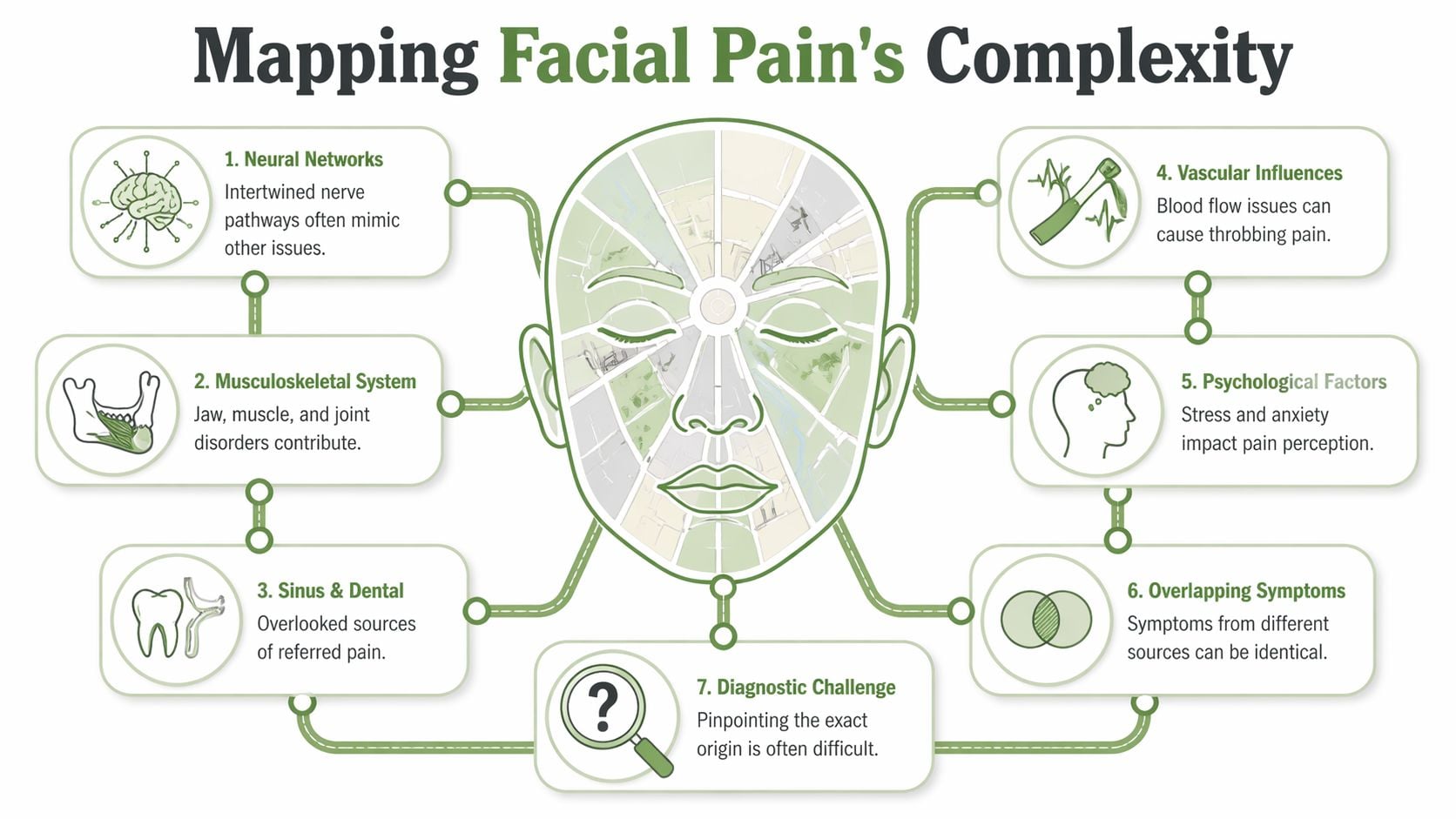
Mapping the Complex World of Facial Pain
Think of your face like a crowded city. Roads, power lines, water pipes, and traffic signals all run close together. If one intersection fails, the whole neighborhood can feel the impact. Facial pain works the same way.
The musculoskeletal system is the city’s framework. That includes the jaw joint, surrounding ligaments, and the muscles that open and close your mouth. The nervous system is the electrical grid. It carries pain, touch, and temperature signals. The sinuses and dental structures act a bit like plumbing and hidden utility lines. Then there are blood vessels, headache pathways, and even stress responses that can change how strongly pain is felt.
Why the source is easy to misread
Pain in the face doesn’t always stay local. A jaw muscle can refer pain into the temple. A cracked tooth can create a deep ache in the cheek. A compressed nerve can feel like a problem in the gums or lips. In an extensive study of orofacial pain symptoms, toothache was the most prevalent at 57.6%, while TMJ region pain affected 8.4% of males and 6.4% of females, which shows how broad the list of possible pain sources really is, as reported in this orofacial pain study.
Patients often get confused because several causes can create nearly identical symptoms:
| Symptom | Could point to |
|---|---|
| Pressure in the cheek | Sinus issue, tooth problem, jaw muscle tension |
| Ear pain without ear infection | TMJ disorder, referred muscle pain |
| Sharp pain with light touch | Nerve pain, severe sensitization |
| Headache at the temple | Clenching, TMJ strain, migraine |
| Pain when chewing | Dental issue, jaw joint disorder, muscle overload |
That overlap is why quick assumptions often fail.
The main categories clinicians sort through
A careful evaluation usually starts by organizing facial pain into broad groups.
- Musculoskeletal causes include TMJ disorders, muscle trigger points, bite overload, and strain from clenching or grinding.
- Neuropathic causes involve irritated or injured nerves. These pains tend to burn, zap, shock, or fire suddenly.
- Dental and ENT causes include tooth infection, abscess, cracked teeth, sinus inflammation, and related pressure problems.
- Referred pain means the place you feel the pain isn’t the place the problem began.
Practical rule: If pain keeps returning after treatment aimed at only one area, the original diagnosis may have been incomplete rather than “wrong.”
Why root-cause thinking matters
If someone only looks at where it hurts, they may miss why it hurts. A patient with “sinus pain” may have jaw tension from nighttime clenching. Someone with “tooth pain” may have nerve irritation. Someone told they have “just TMJ” may also be dealing with poor sleep, airway strain, or a headache disorder that keeps the system inflamed.
That’s why specialists try to map the whole city, not just the street where the traffic jam showed up.
The Usual Suspects TMJ Dental and Sinus Issues
The most common facial pain problems usually come from structures people use all day without thinking about. You chew, talk, swallow, yawn, tense your face during stress, and sleep with your jaw in some position for hours. If one part of that system gets overloaded, the symptoms can spread fast.

TMJ disorders and jaw muscle overload
Temporomandibular joint and muscle disorders, often shortened to TMJ disorders or TMJDs, are the most common non-dental cause of facial pain. They affect 5% to 12% of the population, and parafunctional habits like nighttime clenching have been documented in up to 80% of TMJ patients, according to Baystate Health’s overview of facial pain.
The jaw joint works like a hinge with a sliding track. It has to coordinate with muscles, ligaments, teeth, and posture. When that system is strained, pain doesn’t stay limited to the joint itself. It can spread to the cheeks, temples, ears, neck, and even create headaches.
Common clues include:
- Pain with chewing that worsens through the day
- Morning jaw soreness suggesting nighttime clenching
- Temple headaches that feel muscular or pressure-like
- Clicking, catching, or locking in the jaw
- Ear fullness or pain even when the ear exam is normal
Some patients notice jaw popping before they notice pain. That doesn’t always mean damage, but it can be a clue that the joint is under strain or that the disc and jaw movement aren’t coordinating well. If you’re trying to recognize patterns, this overview of TMJ dysfunction symptoms can help you compare what you’re feeling with common presentations.
What TMJ pain often feels like
TMJ-related pain is usually mechanical. That means it changes with use.
It may flare when you eat chewy foods, hold your mouth open at the dentist, clench during stress, or sleep in a position that loads the joint. Some people describe a sore, bruised, tired feeling in the face. Others feel pressure around the ears or pain that wraps from the jaw into the temple.
Here’s where readers often get tripped up: TMJ pain can feel like a tooth problem, and a tooth problem can feel like TMJ. The systems share nerve pathways.
A painful jaw joint can “broadcast” into nearby muscles and teeth. That’s one reason self-diagnosis goes wrong so often.
Dental causes that radiate beyond the tooth
Dental pain isn’t always a simple cavity. A cracked tooth, inflamed nerve inside the tooth, bite interference, or abscess can send pain across the face. Some patients can’t even identify which tooth hurts because the nervous system blends the signal.
Dental pain often becomes more suspicious when:
- Temperature triggers it, especially cold or heat
- Biting on one side causes a sharp or deep ache
- One tooth feels “high” or hits first
- Swelling, tenderness, or gum changes appear
- The pain throbs and seems to pulse
A dental abscess may create significant pressure and can mimic sinus or cheek pain. A cracked tooth can produce brief but intense pain during chewing, especially when pressure is released. Bite imbalance can also overload the jaw muscles and set up a cycle where the teeth and jaw both start to hurt.
Sinus pain that imitates other conditions
Sinus-related facial pain usually comes from inflammation or blockage that creates pressure in air-filled spaces around the nose and cheeks. But not every feeling of pressure is a sinus problem. That’s where many patients lose time.
True sinus-related pain often clusters with symptoms like congestion, facial fullness, pressure when bending forward, or tenderness around the cheeks and eyes. It may feel heavy rather than electric. People often describe it as a “packed” sensation.
This quick comparison helps:
| Pattern | More suggestive of |
|---|---|
| Dull ache with chewing and jaw use | TMJ or muscle pain |
| Sharp pain on biting one tooth | Dental source |
| Fullness with congestion and pressure | Sinus involvement |
| Morning tight jaw and temple pain | Clenching-related strain |
The overlooked link between structure and habit
The “usual suspects” are common for a reason. They’re influenced by daily habits. Clenching, mouth breathing, poor sleep, one-sided chewing, and posture can keep loading the same tissues again and again. So even when the pain starts in the joint, a tooth, or the sinuses, the long-term solution usually depends on identifying the behavior or body pattern keeping the area irritated.
That’s the difference between temporary relief and actual progress.
When Nerves and Headaches Are the Hidden Cause
When facial pain feels sudden, searing, or strangely out of proportion to touch, clinicians start thinking less about joints and more about the face’s electrical wiring.
Trigeminal neuralgia and other nerve pain
The trigeminal nerve carries sensation from much of the face. If it becomes irritated, the pain can feel less like soreness and more like an electrical short circuit. That’s the hallmark of trigeminal neuralgia.
Trigeminal neuralgia is rare, but it’s one of the most severe facial pain disorders. Its incidence is about 12 new cases per 100,000 people each year, and in roughly half of cases a blood vessel is found compressing the trigeminal nerve, according to OHSU’s explanation of facial pain.
Patients often describe it as:
- Electric-shock pain
- Sudden stabbing or shooting episodes
- Pain triggered by brushing teeth, washing the face, chewing, or a breeze
- Pain on one side of the face
- Brief attacks with fearful anticipation of the next one
That pattern differs from TMJ. TMJ usually builds with use and feels sore, tight, or pressure-like. Trigeminal neuralgia tends to strike fast and intensely.
If facial pain started after dental treatment or seemed to change character after a procedure, a closer look at trigeminal nerve pain after dental work can be useful because post-procedure symptoms don’t always come from the tooth itself.
Headaches that show up in the face
Not all facial pain starts in the face. Some headaches project pain into the cheeks, behind the eyes, or around the jaw. This is especially confusing when there’s no obvious “headache” feeling.
Migraines can create facial pressure, sensitivity, throbbing, nausea, or light sensitivity. Other headache patterns may bring pain near one eye, tearing, congestion, or restlessness. A patient may say, “My cheek hurts,” when the underlying cause is a headache pathway involving blood vessels and facial nerves.
When pain comes with light sensitivity, nausea, tearing, or a clear attack pattern, the diagnosis may belong in the headache family rather than the dental or jaw category.
Here’s a simple contrast:
| Feature | TMJ or muscle pain | Nerve pain | Headache-related facial pain |
|---|---|---|---|
| Quality | Achy, tight, sore | Electric, stabbing, burning | Throbbing, pressure, deep ache |
| Trigger | Chewing, clenching, jaw use | Light touch, breeze, brushing | Attack pattern, sensory triggers |
| Location | Jaw, temple, ear area | Along nerve pathway | Around eye, temple, cheek, forehead |
| Behavior | Can linger and build | Sudden bursts | Episodic or cyclical |
A brief visual explanation can make these distinctions easier to understand.
Why this distinction matters
Muscle pain, nerve pain, and headache pain can all involve the same real estate, but they don’t respond the same way to treatment. A mouthguard won’t fix classic trigeminal neuralgia. A sinus rinse won’t solve a neurovascular headache. And repeated dental work won’t help if the nerve itself is the source of the pain signal.
That’s why the quality of pain matters so much. Not just where it hurts, but how it hurts.
The Path to a Clear Diagnosis
A good diagnosis usually starts long before any scan. It starts with a conversation detailed enough to separate patterns that look similar on the surface.
The history tells you where to look
When I evaluate facial pain, I want the timeline first. Did it begin suddenly or slowly? Was there dental work, an injury, a stressful period, a change in sleep, or a new headache pattern? Does the pain wake you up, worsen with chewing, react to cold air, or appear the moment you touch your face?
These details matter because facial pain conditions often reveal themselves through behavior. A mechanical problem changes with motion. A nerve problem reacts to light triggers. A systemic inflammatory problem may come with symptoms outside the face.
If you’ve never heard the term differential diagnosis, it means making a careful list of reasonable possibilities and then narrowing them down with history, exam findings, and tests. That process is essential in facial pain because the first answer isn’t always the right one.
What the physical exam can reveal
A thorough exam often includes:
- Jaw movement testing to see whether opening, closing, or side-to-side motion triggers pain
- Muscle palpation to identify tender bands or referred pain patterns
- Joint loading checks to see whether the TMJ itself is irritated
- Cranial nerve screening when pain suggests neuropathic involvement
- Dental and bite review to check for local triggers or overload
- Airway and oral posture assessment when clenching, mouth breathing, or poor sleep may be involved
This part is more revealing than many patients expect. If pressing on a chewing muscle recreates the exact pain in your temple or cheek, that’s meaningful. If the pain appears without movement and follows a nerve distribution, that points elsewhere.
The exam isn’t just about finding what hurts. It’s about finding what reproduces your specific pain pattern.
Imaging and testing add structure
When imaging is needed, the test depends on the question.
A CBCT scan can help show jaw joint structure, teeth, bony anatomy, and sometimes airway relationships. An MRI is more useful when a clinician needs to look at soft tissues, discs, nerves, or possible vascular compression. Sometimes blood work becomes important if symptoms suggest inflammation or autoimmune disease rather than a purely local jaw problem.
One commonly missed category involves systemic disease. Sjögren’s syndrome and scleroderma can cause inflammatory trigeminal neuropathy, which can mimic classic trigeminal neuralgia, as discussed in this review of medical causes of facial pain. That’s why dry eyes, dry mouth, skin changes, fatigue, or widespread symptoms shouldn’t be brushed aside as unrelated.
What patients can do before the visit
Bring specifics. They help more than vague summaries.
- Track triggers such as chewing, touching, yawning, cold air, stress, or waking
- Note timing including morning pain, nighttime flares, or brief shock episodes
- List prior treatments and whether they helped, worsened symptoms, or did nothing
- Mention sleep and breathing if you snore, mouth-breathe, grind, or wake unrefreshed
The clearest diagnoses often come from putting those clues together, not from relying on one symptom in isolation.
Modern Treatment Pathways for Lasting Relief
Once the cause is clearer, treatment should match the mechanism. That sounds obvious, but many people have only experienced symptom-chasing. They’ve tried pain medicine for muscle overload, antibiotics for non-infectious pain, or dental procedures for a nerve disorder. Lasting relief usually comes from treating the driver, not just the alarm signal.

Foundation treatments that reduce strain
For many jaw and muscle-based cases, the first layer of care is conservative and practical.
- Custom oral appliances can reduce harmful loading in selected patients with clenching or unstable jaw mechanics.
- Physical therapy or jaw-focused rehab can improve motion, reduce guarding, and calm overworked muscles.
- Diet and habit changes such as softer foods during flares, avoiding gum chewing, and reducing extreme jaw opening can give tissues a chance to settle.
- Headache management becomes important if a neurovascular pattern is amplifying facial symptoms.
These approaches work best when they’re tied to a specific diagnosis. A night guard isn’t a cure-all, but for the right patient it can be one useful tool in a larger plan.
Airway and myofunctional factors deserve more attention
One of the most overlooked answers to “what causes facial pain” is dysfunctional breathing and oral posture. Emerging research connects airway dysfunction and myofunctional habits, including clenching related to sleep-disordered breathing, to chronic facial pain, and notes that orofacial myofunctional therapy and regenerative options like Prolotherapy are showing promise for these root causes, as described in this discussion of common causes of craniofacial pain.
That matters because some people don’t clench only out of stress. They clench because their body is trying to stabilize the jaw or airway during sleep. If you only treat the sore muscles and ignore the breathing pattern, the cycle often returns.
Orofacial myofunctional therapy focuses on retraining:
- Tongue posture
- Lip seal
- Swallow pattern
- Nasal breathing habits
- Jaw resting position
Buteyko breathing techniques may also help selected patients reduce overbreathing patterns and improve breathing awareness. In the right setting, these therapies shift the body from compensation toward more efficient function.
If clenching is your body’s workaround for a breathing problem, the jaw won’t fully calm down until the breathing problem is addressed too.
Regenerative and non-surgical options
Some patients need more than exercise and habit change, especially when ligaments, joint tissues, or chronically irritated structures haven’t healed well. That’s where non-surgical regenerative care may fit.
Common examples include:
| Treatment | General purpose |
|---|---|
| Prolotherapy | Stimulates healing response in weakened supportive tissues |
| PRF injections | Uses the patient’s own blood-derived healing components |
| Cold laser therapy | Aims to calm irritated tissues and support recovery |
These options aren’t one-size-fits-all. They work best when the diagnosis identifies a structural target, such as overloaded joint support tissues or persistent inflammation around the TMJ and surrounding muscles.
One example of a clinic using this root-cause model is Pain and Sleep Therapy Center, which evaluates TMJ pain, facial pain, airway-related contributors, and sleep-disordered breathing, and may combine tools such as regenerative therapy, myofunctional therapy, and breathing-based care depending on the findings.
Treatment works better when it’s layered
The most durable care plans usually combine categories rather than relying on one intervention.
A patient with jaw pain might need an oral appliance, muscle rehab, and better sleep breathing. Someone with referred facial pain might need dental stabilization plus headache treatment. A person with persistent symptoms after years of clenching may improve only when therapy addresses both the joint tissues and the habit pattern that keeps reloading them.
That layered approach is what moves care from temporary relief toward actual healing.
When to See a Specialist for Your Facial Pain
Facial pain deserves specialist attention when it keeps returning, changes in character, or doesn’t match the treatment you’ve already tried. The longer pain goes unexplained, the more likely people are to bounce between partial answers.
Some symptoms shouldn’t wait.
Red flags that need prompt evaluation
- Fever with facial swelling because infection needs urgent assessment
- Sudden severe new pain especially if it feels dramatically different from prior episodes
- Vision changes such as blurred vision, double vision, or eye pain
- Difficulty swallowing or speaking
- Numbness or weakness in the face
- Shock-like one-sided pain triggered by light touch
- Persistent pain after dental treatment when the tooth itself no longer seems to explain it
If your symptoms have become chronic, it may help to consult a clinician who focuses on jaw disorders, nerve-related facial pain, headaches, and airway-associated patterns. This guide to finding a facial pain specialist near you can help you understand what kind of expertise to look for.
How to advocate for yourself
When you speak with your primary care doctor, dentist, or ENT, be specific. Don’t just say, “My face hurts.” Say what triggers it, where it travels, how long it lasts, and what hasn’t worked.
That level of detail helps the right referral happen faster.
Facial pain is real. It’s diagnosable. And in many cases, relief starts when someone stops treating it like a mystery and starts tracing it back to the system that’s driving it.
If you’re dealing with jaw pain, headaches, facial muscle tension, or symptoms that may be tied to sleep and breathing, Pain and Sleep Therapy Center offers evaluation focused on finding the root cause and matching treatment to the pattern behind your pain.



