
You wake up tired even after a full night in bed. Your jaw feels tight before breakfast. Your lips are dry. Your child snores, sleeps with an open mouth, or always seems congested. A lot of people assume these are separate problems. They often aren’t.
One habit can sit underneath all of them. Mouth breathing.
When breathing shifts away from the nose and becomes the body’s default pattern, the effects don’t stay in the airway. They show up in sleep quality, jaw tension, facial muscle strain, swallowing, oral posture, and daily energy. That’s why myofunctional therapy for mouth breathing matters so much. Done well, it isn’t a random set of tongue exercises. It’s part of a root-cause plan to help the mouth, jaw, airway, and nervous system work together the way they should.
The Hidden Habit Wrecking Your Health An Intro to Mouth Breathing
A common story sounds like this. An adult comes in because of clenching, headaches, snoring, or constant fatigue. A parent brings in a child for restless sleep, chapped lips, crowded teeth, or a tongue-tie evaluation. In both cases, the person has usually spent a long time treating symptoms one by one.
Then you notice the pattern. Lips part at rest. The tongue sits low. The head drifts forward. Breathing comes through the mouth, especially at night.
Why mouth breathing starts
Mouth breathing usually begins for a reason. Nasal congestion from allergies, chronic stuffiness, enlarged tonsils or adenoids, structural nasal issues, a restricted tongue, or long-standing oral habits can all push the body into compensation. Over time, that compensation becomes automatic.
That’s why “just close your mouth” rarely works. If the nose feels blocked, the jaw is unstable, or the tongue can’t rest where it should, the body will return to the easier route. Habit follows function.
Indoor triggers can matter too. If air quality is part of the problem, practical steps that help families breathe healthier may support the bigger picture, especially when nasal irritation keeps the mouth open at night.
Signs people often miss
Some signs are obvious. Others are easy to dismiss as personality, stress, or “just how my child sleeps.”
- Morning symptoms include dry mouth, sore throat, headaches, jaw tightness, and unrefreshing sleep.
- Daytime clues include lip separation at rest, frequent sighing, noisy breathing, fatigue, brain fog, and forward head posture.
- Childhood patterns can include open-mouth posture, drooling on the pillow, restless sleep, speech concerns, dental crowding, and a long, tired facial appearance.
- Functional signs include noisy chewing, poor lip seal, tongue thrust, and swallowing that recruits the lips and chin instead of staying smooth and efficient.
Mouth breathing is rarely an isolated habit. It usually reflects an airway, posture, tissue, or neuromuscular problem that the body has been compensating for.
There’s also evidence that changing this pattern can matter clinically. A 2024 review in PMC found that long-term data is still emerging, but one trial showed 38% of children who completed myofunctional therapy achieved a correct closed-lip posture compared with 25% of the untreated group. That doesn’t mean every patient gets a perfect long-term result. It does show a meaningful trend toward restoring habitual nasal breathing.
For readers who want a deeper look at practical next steps, this guide on how to stop mouth breathing is a useful companion.
What Is Orofacial Myofunctional Therapy
Orofacial myofunctional therapy, often shortened to OMT, is physical therapy for the muscles of the tongue, lips, cheeks, jaw, and face. The goal isn’t cosmetic. The goal is function.
When these muscles work out of sync, people compensate. They breathe through the mouth. They brace the lips to swallow. They overuse the jaw. They rest with the tongue low instead of supported against the palate. OMT retrains those patterns so healthy function becomes more automatic.
The three core goals
Most treatment centers around three foundational changes.
First, the tongue needs a stable resting place. In healthy oral rest posture, the tongue rests up against the palate instead of lying low in the mouth. That matters because tongue posture influences breathing, swallowing, and jaw stability.
Second, the body has to return to nasal breathing as the default. Nasal breathing supports better oral posture and helps the airway work more efficiently. OMT doesn’t force that switch. It trains the muscles and habits that make the switch possible.
Third, treatment works toward a proper swallow pattern. A functional swallow shouldn’t require lip strain, chin puckering, or tongue pressure against the teeth. When swallowing improves, many patients also notice less tension in the face and jaw.
What therapy feels like in real life
Most patients are relieved when they learn this isn’t a passive treatment. It’s active, teachable, and specific. Sessions usually involve assessment, guided practice, feedback, and a home program.
Some exercises look simple. That can be misleading. The challenge isn’t doing a movement once in the office. The challenge is repeating the correct movement until the body stops defaulting to the old one.
This short video gives a helpful visual overview of how oral posture and breathing exercises can look in practice.
Clinical perspective: OMT works best when it targets function, not just strength. Strong muscles with the wrong pattern still create strain.
For that reason, myofunctional therapy for mouth breathing is often part of a wider plan. If nasal blockage, tongue restriction, sleep-disordered breathing, or TMJ instability is present, those issues need attention too.
How Myofunctional Therapy Retrains Your Body for Nasal Breathing
Myofunctional therapy works through neuromuscular re-education. That means it doesn’t just strengthen muscles. It teaches the brain and body a new default pattern.
A person can understand that nasal breathing is better and still keep sleeping with an open mouth. That’s not a motivation failure. It’s usually a patterning problem. The tongue drops, the lips part, the jaw loses support, and the body repeats what it has practiced for years.
What changes during treatment
OMT uses specific exercises to improve how the tongue, lips, jaw, and soft tissues coordinate. As these patterns improve, breathing often becomes quieter, more stable, and less effortful.
A key piece of evidence comes from a Level 1 randomized controlled trial summarized here. It showed that oropharyngeal exercises in myofunctional therapy directly modify tongue tone, increase oxygen saturation, and reduce oral breathing. The same review explains the mechanism clearly. Better tongue tone helps raise the soft palate and stabilize the airway, which counters the collapse that mouth breathing can contribute to during sleep.
The body systems involved
This is why the effects can reach far beyond the mouth.
- Tongue posture supports the palate and influences how the airway behaves.
- Lip seal reduces habitual open-mouth posture and supports nasal airflow.
- Jaw stability lowers compensatory muscle overuse in the face and neck.
- Swallow coordination reduces strain patterns that keep pulling the mouth and tongue out of position.
OMT is not just muscle work. It is repeated practice that turns a conscious correction into an unconscious habit.
That’s also why random online exercises often disappoint people. If the exercise doesn’t match the dysfunction, the body rehearses the wrong thing more efficiently. Assessment matters first, then precision, then repetition.
Why consistency changes outcomes
Patients often ask why the same movement needs so many repetitions. The answer is simple. Old habits are automatic because they’ve been repeated thousands of times. New habits need enough correct reps to compete.
A structured home program helps bridge that gap. These orofacial myofunctional therapy exercises show the kind of targeted work that may be used, but the right sequence still depends on the individual. Someone with a low resting tongue posture needs a different emphasis than someone whose main issue is poor lip seal or jaw compensation.
What works is specific, consistent practice tied to actual function. What doesn’t work is trying to force nasal breathing while the rest of the system still pulls in the opposite direction.
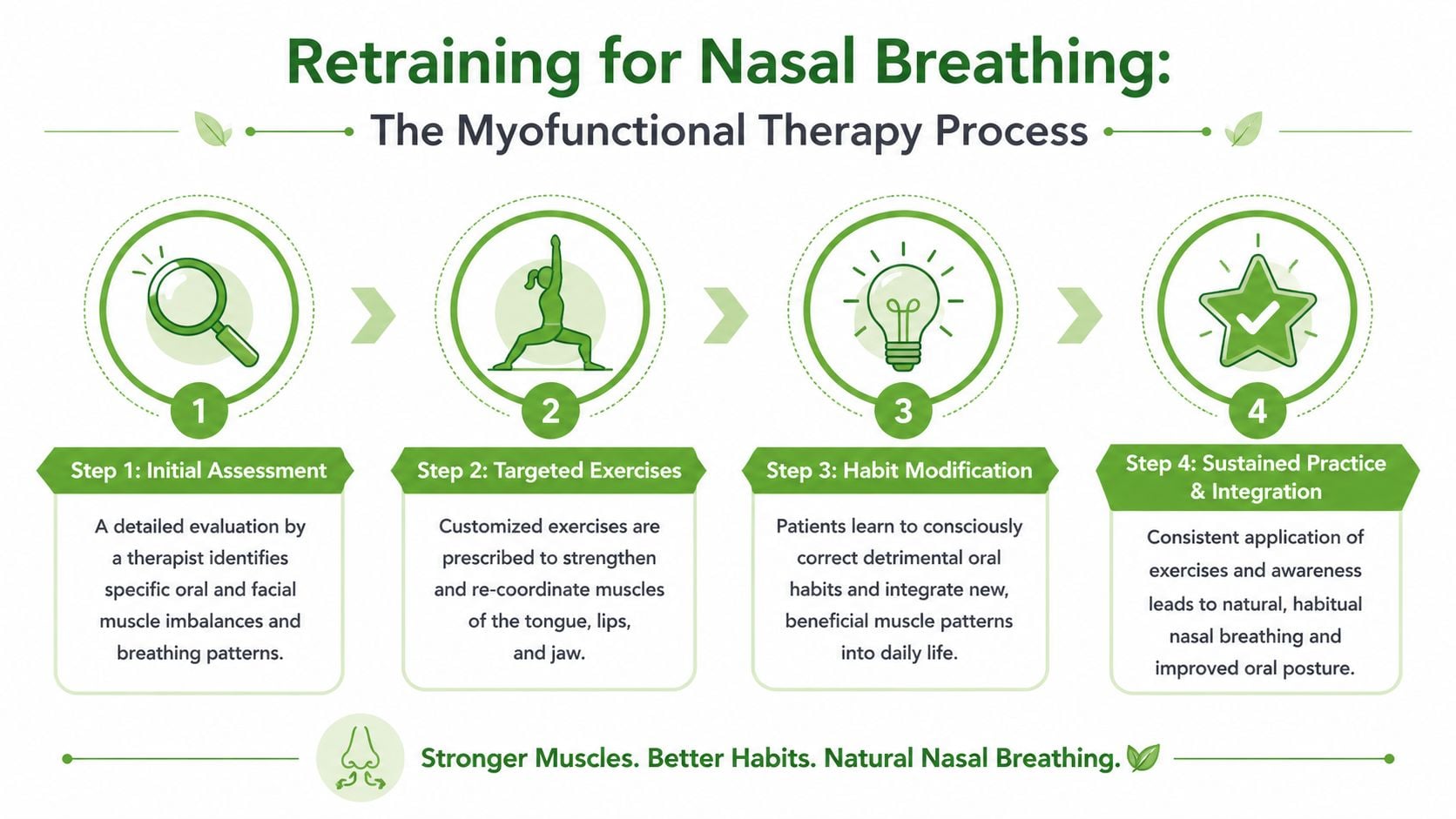
Your Path to Healthier Breathing The OMT Treatment Process
The treatment process is straightforward, but it requires commitment. Most patients do best when they understand two things early. First, this is personalized care. Second, progress depends heavily on what happens between visits.
What the first phase looks like
An initial evaluation usually looks at oral rest posture, breathing pattern, lip function, tongue mobility, swallowing, jaw behavior, and contributing habits. If there are signs of airway obstruction, sleep-disordered breathing, tongue restriction, or TMJ overload, those findings help shape the plan.
From there, therapy is built in phases rather than thrown at the patient all at once. Early work often focuses on awareness and foundational control. Later work reinforces automaticity during speaking, eating, sleeping, and daily life.
A realistic timeline
One of the biggest mistakes people make is expecting a short burst of exercises to permanently erase a long-standing habit. In practice, OMT often unfolds over months, not days.
According to this overview on what to expect from myofunctional therapy, programs often involve exercises for about 12 months, but long-term adherence rates aren’t well documented. That’s an important reality check. Permanent change depends on building strong habits, not finishing a checklist.
What I tell patients: Don’t measure success by how hard an exercise feels. Measure it by whether your body starts using the new pattern when you’re not thinking about it.
Sample Myofunctional Therapy Exercises and Timeline
| Phase | Typical Duration | Focus | Sample Exercise |
|---|---|---|---|
| Foundation | Early phase | Awareness of oral rest posture and nasal airflow | Tongue-to-spot hold |
| Coordination | Middle phase | Lip seal, tongue control, and jaw stability | Lip closure drills |
| Functional retraining | Middle to later phase | Swallowing without lip or chin compensation | Controlled water swallow practice |
| Integration | Later phase | Carryover into meals, speech, and sleep routines | Rest posture checks during daily activities |
The names of exercises vary by provider, and not every patient needs the same sequence. A child with a tongue-tie history may need a different progression than an adult with chronic clenching and open-mouth sleep posture.
What helps and what stalls progress
Patients usually move faster when they:
- Practice daily with short, focused repetition instead of occasional long sessions.
- Track triggers such as congestion, stress, poor sleep, or daytime mouth opening.
- Follow referrals if the therapist identifies nasal obstruction, sleep issues, or structural limits.
- Treat this as skill-building rather than as a quick fix.
Progress often slows when someone relies on office visits alone, skips home practice, or tries to power through unresolved airway or tissue restrictions.
That isn’t failure. It’s feedback. If the plan isn’t sticking, the question becomes why.
OMT for All Ages Treating Kids Adults TMJ and Sleep Apnea
A child who sleeps with an open mouth, an adult who wakes up exhausted, and a patient with persistent jaw pain may look like three different cases. In practice, I often see the same pattern underneath. Poor oral rest posture, low tongue posture, airway strain, and muscle compensation can show up at any age, then drive pain, poor sleep, and fatigue in different ways.
Pediatric care and developing faces
In children, mouth breathing can influence far more than daytime habits. It can affect chewing, swallowing, sleep quality, speech patterns, and the way the jaws and dental arches grow over time. That is why early care matters. The goal is not cosmetic change. The goal is to support healthy development before strained breathing patterns become the child’s normal.
Children also need a team approach more often than adults do. Enlarged tonsils, chronic congestion, tongue restriction, and sleep-disordered breathing can all interfere with progress. OMT helps a child learn better lip seal, tongue posture, and swallowing mechanics after those barriers are identified and addressed.
The therapy has to fit the child, not the other way around. Younger patients do better with simple cues, short practice, and strong parent follow-through. If home routines are unrealistic, progress usually stalls.
Adults with fatigue snoring and tension
Adults commonly come in after trying to solve isolated symptoms. They may have changed pillows, used a night guard, treated stress, or accepted snoring and fatigue as part of aging. Meanwhile, the mouth still falls open during sleep, the tongue stays low, and the jaw and neck muscles keep overworking.
That pattern matters because OMT can support the bigger treatment plan, not just provide a few exercises. For adults with airway collapse, snoring, unrefreshing sleep, or CPAP intolerance, it can improve oral posture and muscle function in a way that supports better nighttime breathing. Patients exploring that part of care can review this page on myofunctional therapy for sleep apnea.
Results vary. Adults with untreated nasal obstruction, significant sleep apnea, or high stress loads may need medical or dental treatment alongside therapy. That is often the difference between short-term effort and lasting relief from fatigue.
Where TMJ and facial pain fit
TMJ symptoms rarely exist in isolation. A low tongue posture can leave the jaw less supported at rest. Chronic mouth breathing can encourage forward head posture, lip strain, clenching, and overuse in the cheeks, temples, and neck. Over time, patients may notice clicking, tension headaches, facial soreness, and pain with chewing.
Proper evaluation matters here. If the jaw is painful because the airway is unstable, a splint alone may not solve the problem. If sleep is fragmented, muscles never get much chance to recover. For patients trying to connect those dots, this guide to understanding myofascial pain syndrome can help explain why muscle pain often spreads beyond one small area.
This is one reason I treat myofunctional therapy as a foundation of root-cause care rather than a stand-alone add-on. In the right case, it supports jaw stability, better breathing mechanics, more efficient swallowing, and improved sleep quality at the same time. That integrated effect is what patients care about most. Less pain. Better sleep. More energy during the day.
One example of that model is Pain and Sleep Therapy Center, which evaluates TMJ disorders, facial pain, sleep-related breathing issues, and myofunctional patterns together rather than treating each complaint separately.
How to Choose a Qualified Myofunctional Therapy Clinic
The right clinic does more than hand you a worksheet of exercises. It identifies why you’re mouth breathing, what’s preventing change, and how success will be measured over time.
Questions worth asking
Start with the basics, then go deeper.
- Who evaluates me. Ask whether the provider assesses oral rest posture, swallowing, breathing pattern, jaw function, and contributing airway factors.
- How personalized is the plan. A generic sequence may miss the underlying driver, especially if tongue restriction, nasal obstruction, or sleep apnea is involved.
- Do you work with other specialists. ENTs, sleep physicians, dentists, orthodontists, pediatric providers, and bodywork professionals may all be relevant depending on the case.
- How do you track progress. A clinic should be able to explain what it’s watching for clinically, not just tell you to “keep practicing.”
Why an integrated approach matters
An isolated approach often breaks down in more complex cases. If the nose is blocked, exercises won’t overcome anatomy by willpower alone. If the patient has untreated sleep-disordered breathing, fatigue can sabotage compliance. If the jaw is unstable or painful, the mouth may keep compensating despite effort.
That’s why interdisciplinary care is so valuable. Good clinics know when OMT is the main treatment and when it needs support from airway evaluation, TMJ care, tongue-tie management, or sleep treatment.
Look for clinics that think predictively
Advanced care also means better patient selection, as not every patient responds the same way or on the same timeline.
As noted in this discussion of predictive outcomes in myofunctional therapy care, a key differentiator is using data to predict outcomes. For example, top-tier clinics may look at which OSA severity levels respond best to OMT or use sleep study metrics to identify who is most likely to benefit before starting a program that may last 12 months.
A qualified clinic should be comfortable saying, “This is what OMT can help, this is what it cannot fix by itself, and this is how we’ll know whether it’s working.”
That kind of honesty protects patients. It keeps expectations realistic and makes treatment more efficient.
Common Questions About Myofunctional Therapy
Patients usually want to know three things before they start. Will it hurt, how long will it take, and can it make a real difference in sleep, jaw pain, and daily energy. Those are the right questions, because myofunctional therapy works best when expectations are clear from the start.
Understanding the treatment experience
OMT is usually gentle. The work is active and focused, more like skill training than a procedure. You may feel muscle fatigue, increased awareness of tongue or lip tension, or the strange sensation of using muscles that have been compensating for years. Pain is not the goal. If a patient already has TMJ tenderness, limited tongue mobility, or facial pain, I adjust the program so we improve function without provoking symptoms.
Sessions are practical. We review what happened between visits, correct exercise form, and connect each drill to a daily task such as nasal breathing at rest, swallowing without strain, clearer speech patterns, or keeping the mouth closed during sleep. Children often need shorter, more visual sessions with parent support. Adults usually do better when they understand why each exercise matters and how it connects to poor sleep, jaw tension, morning headaches, or fatigue.
Home practice matters because the body changes through repetition. A weekly visit can guide the process, but it cannot replace the daily work that turns a new pattern into an automatic one. That is true whether the patient is six years old and mouth breathing through the night or an adult with snoring, clenching, and unrefreshing sleep.
How long change takes, and why it varies
Some people notice early wins within the first phase of care. Their lips stay together more easily, nasal breathing feels less effortful, or they catch themselves before dropping into open-mouth posture during the day. Lasting change takes longer because the goal is not a temporary performance in the clinic. The goal is a different default pattern during sleep, meals, speech, exercise, and stress.
The timeline depends on what is driving the problem. A patient with a habit-based mouth breathing pattern may progress faster than someone with chronic congestion, sleep-disordered breathing, a restricted tongue, or an unstable jaw. That difference matters. If the airway is compromised or the jaw is compensating, exercises alone may improve function but may not fully resolve the pattern.
Where OMT fits in a larger treatment plan
Myofunctional therapy can stand on its own in the right case, but many patients need it as part of a root-cause plan. That is one of the most important points in this entire guide.
If mouth breathing is primarily a learned oral posture problem and nasal breathing is available, OMT may carry much of the treatment load. If the patient also has sleep apnea, upper airway resistance, TMJ dysfunction, significant tongue restriction, or developmental concerns in a child, OMT becomes the foundation that supports the rest of care. It helps the mouth, tongue, jaw, and airway work the way they were designed to work. That can improve the results of sleep treatment, reduce strain on the TMJ system, and support healthier facial growth in children.
This integrated view is why OMT has value beyond “exercises.” It addresses a functional pattern that affects sleep quality, facial pain, chewing, swallowing, speech, and how restored you feel when you wake up.
Common concerns about results, cost, and children
Patients with snoring or sleep apnea often ask whether OMT can help. It often can, especially when low tongue posture, oral breathing, and poor airway muscle coordination are part of the picture. The degree of improvement depends on severity and on whether other treatment is also needed. For mild cases, OMT may provide meaningful support. For more complex cases, it usually works best alongside sleep medicine, dental airway treatment, ENT care, or TMJ treatment.
TMJ patients ask a similar question. OMT can reduce one of the drivers of chronic jaw irritation when poor tongue posture, clenching patterns, muscle overuse, or dysfunctional swallowing are keeping the jaw overloaded. It does not replace every form of TMJ care, but it often helps the system calm down because the muscles stop fighting the same dysfunctional pattern all day and all night.
Parents usually do not walk in saying, “My child has an orofacial myofunctional disorder.” They come in because they see signs that something is off. Open-mouth posture, snoring, drooling on the pillow, restless sleep, speech concerns, messy swallowing, dental crowding, and a history of tongue-tie all justify an evaluation. Early assessment matters because breathing and oral posture influence development, not just comfort.
Insurance coverage is less predictable. Some services may fall under dental benefits, medical benefits, out-of-network reimbursement, or no coverage at all, depending on diagnosis, documentation, and provider type. A good clinic should explain fees early, describe how services are coded, and help patients understand what they may be able to submit. Clear financial planning reduces stress and helps families commit to care without surprises.
Pain and Sleep Therapy Center provides evaluation and treatment for TMJ disorders, facial pain, sleep-related breathing problems, and orofacial myofunctional dysfunction, with care plans built around the factors driving the problem rather than symptom relief alone.



