
You may be reading this because something feels off, but it doesn’t look dramatic enough to count as a “real” breathing problem. Maybe you get winded while sitting still. Maybe your partner says your breathing gets noisy at night, then suddenly quiet. Maybe you wake with a tight jaw, a dry mouth, a headache, and a strange sense that sleep didn’t restore anything.
That’s where respiratory rate becomes useful.
Respiratory rate is the number of breaths taken in a minute. It sounds basic, almost too basic. Yet it can reveal whether your body is calm, strained, compensating, obstructed, sedated, or struggling to maintain balance. Many individuals know their heart rate. Some know their blood pressure. Very few know how fast they breathe at rest.
That gap matters. In hospitals, clinicians have long recognized that an abnormal respiratory rate can be an early sign of serious decline. Outside the hospital, the same vital sign can indicate a different kind of problem. Not a sudden crisis, but a chronic pattern tied to snoring, sleep apnea, mouth breathing, facial tension, poor oral posture, anxiety, fatigue, and TMJ-related dysfunction.
A useful way to think about breathing rate: it’s your body’s “idle speed.” When you’re resting, your breathing tells you how hard the system is working even when you aren’t doing much.
If your breathing is too fast, too slow, irregular, or effortful, that pattern deserves attention. Sometimes it reflects infection, medication effects, or metabolic illness. Sometimes it reflects airway resistance, poor sleep, or the way the jaw, tongue, neck, and ribcage are working together.
Introduction
A common scenario goes like this. Someone notices they’re breathing through their mouth during the day, their shoulders lift when they inhale, and they feel tired even after a full night in bed. They assume it’s stress. Then someone points out their snoring, or they start waking with jaw pain and morning headaches, and suddenly the pattern looks less random.
Another version is quieter. A parent watches a child sleep and notices restless breathing, odd pauses, or noisy airflow. Or a dentist, orthodontist, ENT, or primary care clinician sees a patient with facial tension, poor oral posture, and fatigue, but the breathing rate never gets measured because the room isn’t an emergency department.
That’s one reason respiratory rate is so often missed. It’s simple, but it isn’t trivial. It can act like an early alarm bell long before lab work, scans, or symptoms become obvious. It can also be overlooked precisely because people associate breathing problems with dramatic distress rather than subtle dysfunction.
For patients with sleep-disordered breathing or TMJ symptoms, that oversight can keep the underlying driver hidden. A person may chase headaches, neck tension, clenching, or daytime fatigue for years without anyone asking whether they breathe too fast at rest, too shallowly through the chest, or too poorly through the nose.
Breathing sits at the intersection of airway structure, brain regulation, metabolism, posture, and pain. When the rate shifts, it often tells you that one of those systems is under strain.
What Is a Normal Respiratory Rate and Why Does It Matter
A resting respiratory rate is the number of times you fully inhale and exhale in one minute. Clinicians measure it when a person is calm, quiet, and not talking, because activity, conversation, pain, and anxiety can all push the number up for a short time.
Breathing rate works like an engine idle speed. When the body is running smoothly, the rate usually stays in a steady range at rest. If it has to speed up to keep oxygen delivery, carbon dioxide balance, or airway flow on track, that extra effort can be an early clue that something underneath is off.
For adults, a normal resting respiratory rate is 12 to 20 breaths per minute. A rate above that range deserves context, not dismissal. In emergency settings, a faster rate can be one of the earliest signs of serious illness. Outside the hospital, the same pattern can also show up in quieter problems such as chronic mouth breathing, nasal obstruction, poor diaphragm use, sleep-disordered breathing, or the strain pattern seen in some people with jaw and facial pain.
That wider view matters. Someone can have a breathing pattern that is abnormal for them long before they look acutely sick.
Normal ranges by age
| Age Group | Normal Range (Breaths/Minute) |
|---|---|
| Infants | 40 to 60 |
| Children | Higher than adults and gradually slows with age |
| Adults | 12 to 20 |
| Older adults | Usually interpreted using adult resting range |
Children breathe faster than adults because their bodies are smaller and their metabolic demands differ. The rate then slows with growth. In older adults, the adult resting range still guides interpretation, but the number should always be read alongside the full picture, including sleep quality, medication use, posture, pain, and cardiopulmonary health.
Why this number gets missed
Respiratory rate is simple to measure, yet it is often underused. Pulse and oxygen saturation get attention because monitors display them instantly. Breathing rate usually requires someone to slow down, watch, and count.
That gap creates blind spots.
A person may have normal oxygen saturation and still breathe too fast, too shallowly, or with too much upper chest effort. That is one reason chronic breathing dysfunction can hide in plain sight. Patients may be told their lungs sound clear while they continue to wake unrefreshed, clench their jaw, live with facial tension, or feel air hunger during the day. Some also have sleep-related airway resistance that falls short of classic obstructive sleep apnea but still disrupts rest, as seen in upper airway resistance syndrome.
What “abnormal” really means
An abnormal respiratory rate is not just a high number.
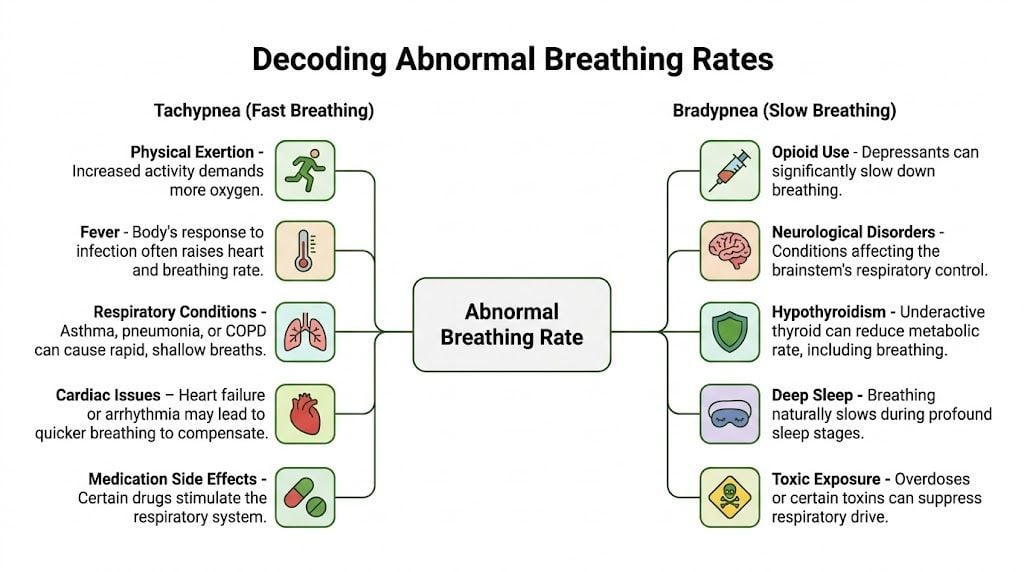
- Too fast means tachypnea. In adults, that generally means a resting rate above the normal range.
- Too slow means bradypnea. In adults, under 12 breaths per minute can signal a problem in the right context.
- Irregular means the rhythm or spacing of breaths is inconsistent.
- Effortful means the number may look acceptable, but the mechanics are strained. The neck lifts, the shoulders rise, the mouth stays open, or the chest does most of the work.
That last pattern is easy to miss and highly relevant in chronic care. A patient can sit in a dental chair or primary care exam room with a respiratory rate that does not trigger alarm, yet still show a dysfunctional breathing style that feeds poor sleep, muscle guarding, jaw overuse, and persistent fatigue.
People often associate breathing trouble only with dramatic shortness of breath. In practice, abnormal breathing can be loud and obvious, or quiet and habitual. The body adapts for a while. Then the downstream effects start showing up somewhere else: sleep, pain, focus, endurance, headaches, or TMJ symptoms.
Respiratory rate matters because it is often the first visible sign that the system is compensating. Sometimes that compensation points to urgent illness. Sometimes it points to a chronic, treatable pattern that has been overlooked for years.
Decoding the Causes of an Abnormal Breathing Rate
A patient can look calm in the exam chair, answer questions normally, and still be breathing in a way that signals strain. Another patient arrives in obvious distress, breathing fast because the body is fighting to keep oxygen, carbon dioxide, and pH in balance. Both patterns matter. One is easier to spot.
A useful way to sort the causes is to ask three questions. Is the whole body under stress? Is the brain changing the breathing rhythm? Is the airway or breathing mechanics making each breath less effective? That framework helps connect emergency medicine causes with the slower, often-missed patterns seen in sleep problems, jaw tension, and chronic facial pain.
Systemic medical causes
Breathing rate often rises because the body is trying to correct a chemistry problem.
Fever, infection, asthma, pneumonia, COPD, and heart failure can all make gas exchange less efficient. When each breath does less work, the body often responds by taking more breaths. Metabolic problems can do the same thing. In acidosis, for example, faster breathing helps remove carbon dioxide so the blood can move back toward a safer pH range.
This is why respiratory rate can act like an early warning light on a dashboard. The number itself is not the diagnosis. It is a clue that the body is compensating.
If someone reports chest tightness, air hunger, or shortness of breath, the lungs are only one place to look. Cardiac strain, infection, medication effects, blood sugar problems, and poor sleep can all shape the pattern.
Neurological and psychological causes
Breathing is automatic, but it is not simple.
The brainstem sets the baseline rhythm, then adjusts it based on carbon dioxide, oxygen, pain, posture, and alertness. The NCBI overview of respiratory physiology describes the pre-Botzinger complex as a key rhythm-generating area. When brain function, consciousness, or chemical signaling changes, breathing can become too slow, too fast, or irregular.
A few examples are common in clinical practice:
- CNS depressants: Opioids and sedatives can reduce respiratory drive and slow the rate.
- Pain and stress responses: These often raise the rate, sometimes before other signs become obvious.
- Neurologic pattern changes: Cheyne-Stokes and Biot respirations can point to heart failure, brain injury, or drug effects.
Anxiety adds another layer. Some patients do not only breathe faster. They breathe from the upper chest, overuse the neck and shoulder muscles, and keep the mouth open more often. That pattern can lower carbon dioxide too quickly, which may trigger lightheadedness, tingling, chest discomfort, and a sense of not getting a satisfying breath.
Over time, the pattern can become familiar enough that the patient stops noticing it. Clinicians in airway, sleep, and TMJ care see this often. The respiratory rate may sit near a normal range while the mechanics stay inefficient.
Mechanical and sleep-related causes
In this context, chronic cases are missed.
A narrowed airway changes how the whole system behaves. If airflow is limited during sleep, or if the nose, palate, tongue, jaw, or neck posture makes breathing harder during the day, the body may increase rate or effort to make up the difference. It is similar to sipping through a pinched straw. You may still get air, but the work rises and the pattern changes.
That matters well beyond snoring. Sleep-disordered breathing can disturb nervous system balance, fragment sleep, and train the body into shallow, effortful breathing. In some patients, the result shows up as morning headaches, fatigue, poor concentration, jaw clenching, facial pain, or stubborn muscle tension long before anyone labels it a breathing problem.
For readers who suspect airflow limitation without classic apnea symptoms, this explanation of upper airway resistance syndrome can help connect disrupted breathing with sleep fragmentation and daytime symptoms.
Jaw tension and breathing mechanics often reinforce each other. A person with forward head posture, limited nasal breathing, poor tongue posture, or chronic mouth breathing may recruit the neck and jaw to help move air. That extra muscle work can feed TMJ symptoms, while poor sleep lowers pain tolerance and recovery. The respiratory rate may be only mildly abnormal, yet the pattern still points to a treatable root cause.
That is the part many standard explanations leave out. Abnormal respiratory rate is not only an emergency sign. It can also be a quiet marker of chronic airway strain, dysfunctional breathing, and sleep-related overload that responds to targeted, non-surgical care.
How to Measure and Track Your Breathing Rate
You don’t need a hospital monitor to learn a lot from your breathing. A watch, a timer, and a little consistency are often enough to spot patterns.

The simple manual method
The most accurate home measurement is often the simplest one. Sit still or lie down. Rest for a few minutes. Then count how many breaths occur in a full minute.
A few details make a difference:
- Don’t announce you’re measuring. If someone knows they’re being watched, they often change how they breathe.
- Count complete breath cycles. One inhale and one exhale count as one breath.
- Use a full minute when possible. Shorter counts can miss irregular patterns.
- Measure at consistent times. Morning, bedtime, and calm seated rest are useful checkpoints.
- Track context. Note whether you were anxious, congested, in pain, or just woke up.
If you’re measuring another person, watch the chest or abdomen rather than asking them to “take normal breaths.” Once attention shifts to the act of breathing, the pattern often changes.
Clinical observation and home tech
Clinicians may count breaths by observation or while listening with a stethoscope. In sleep and airway care, the pattern matters as much as the number. Is the chest lifting more than the abdomen? Is there nasal breathing or mouth breathing? Are there pauses, sighs, gasps, or visible effort?
For some people, overnight trends matter more than a single daytime count. That’s why consumer devices have become useful screening tools. Apple Watch, Oura Ring, Whoop, and ECG-based systems don’t all calculate respiratory rate the same way, but many estimate it through beat-to-beat oscillations or related physiologic signals.
The SSCOR review on abnormal respiratory patterns notes that wearable and ECG-derived monitoring can passively detect respiratory rate and highlights a 2025 study in which extreme values, below 8 or above 30 breaths per minute, were associated with double mortality risk in ambulatory settings.
That kind of data doesn’t replace clinical judgment. It does make trends harder to ignore.
What to watch for over time
A single reading can be misleading. Trend lines are more useful.
Look for patterns such as:
- A steadily increased resting rate
- Higher rates during sleep or immediately upon waking
- Large changes during illness, pain flare-ups, or stress
- Breathing that looks shallow, noisy, or effortful even when the number seems “normal”
- Wearable data that lines up with snoring, fatigue, or frequent awakenings
If you’re unsure whether your sleep is affecting daytime breathing, this guide on how to diagnose sleep apnea at home gives a practical overview of what home evaluation can and can’t tell you.
A short visual walk-through can also help if you’ve never measured breathing rate before.
Practical rule: Don’t obsess over one isolated number. Pay attention to repeat patterns, symptoms, and whether your breathing looks easy or effortful.
The Critical Link Between Breathing, Sleep Apnea, and TMJ
Most articles about abnormal respiratory rate stop at emergencies. They discuss sepsis, overdose, pneumonia, or diabetic ketoacidosis, then end. That’s useful, but it leaves out a large group of people whose breathing is chronically inefficient rather than acutely catastrophic.
Those patients often show up with snoring, jaw pain, clenching, facial tension, poor sleep, headaches, and daytime fatigue.
The overlooked daytime pattern
The verified data behind this outpatient gap matters. The NCBI summary on breathing dysfunction and related patterns notes that while standard medicine focuses on acute tachypnea above 20 breaths per minute, many people with TMJ disorders and sleep-disordered breathing have a chronic dysfunctional pattern. Poor nasal breathing and jaw dysfunction can drive compensatory over-breathing in the range of 15 to 20 breaths per minute at rest, which can worsen headaches and fatigue.
That range may not trigger alarm in a rushed office visit. But it can still represent a system that never really settles.
Imagine driving with your foot slightly on the gas and slightly on the brake all day. The car still moves. But it burns more fuel, creates more wear, and never feels smooth.
How the jaw and airway affect the breath
TMJ disorders don’t exist in isolation. The jaw, tongue, palate, facial muscles, neck posture, and airway all influence one another.
When the jaw is tense or poorly positioned, several things can happen:
- Mouth breathing becomes more common. Nasal breathing drops off, especially during sleep.
- Neck and accessory breathing muscles work harder. The person starts lifting the chest and shoulders rather than expanding through the lower ribcage.
- Forward head posture narrows the airway. The body adapts by increasing effort and often increasing rate.
- Sleep becomes fragmented. The brain keeps reacting to airflow resistance, even if the person doesn’t remember waking.
This is why a patient may say, “My jaw hurts, but I also feel tired and wired all the time.” The breathing pattern may be helping maintain that state.

Why sleep changes the whole picture
During sleep, the body loses some of the muscular support that helps keep the airway open. If the tongue posture is poor, the jaw position is unstable, or the airway is already narrow, breathing can become noisy, restricted, or repeatedly interrupted.
That’s why sleep position sometimes makes a noticeable difference. For readers trying to reduce nighttime airway collapse or snoring, this guide on the best position to sleep to avoid snoring offers practical context on positional effects.
But position is only part of the story. If a person has underlying airway vulnerability, they may still wake unrefreshed, mouth-breathe overnight, or show signs of daytime over-breathing even when they try to sleep “the right way.”
The symptoms people often separate, but shouldn’t
Patients often split their symptoms into unrelated boxes:
- jaw pain
- headaches
- clenching
- snoring
- dry mouth
- fatigue
- anxiety
- lightheadedness
- neck tension
Clinically, these can belong to the same network. If breathing is inefficient, the nervous system stays more activated. If sleep is fragmented, pain sensitivity often rises. If the jaw and tongue posture are off, the airway may become less stable.
For a broader overview of how these patterns fit together, this page on sleep apnea causes and symptoms is a useful starting point.
A person doesn’t need to be gasping dramatically to have meaningful breathing dysfunction. Chronic strain is still strain.
Why root-cause care matters
When the issue is chronic, symptom-only treatment usually falls short. Mouth taping without evaluation, pain medication without airway assessment, or a generic night guard without attention to breathing mechanics may help temporarily or may miss the root cause altogether.
That’s why therapies aimed at restoring nasal breathing, oral posture, tongue function, and coordination of the jaw, diaphragm, and ribcage can be so meaningful. In the right patient, that’s where approaches such as orofacial myofunctional therapy and breathing retraining fit.
Seeking Help From Red Flags to Root-Cause Solutions
A patient can sit in front of you talking in full sentences and still be showing a breathing pattern that deserves attention. Another patient may look obviously distressed, with fast, deep, effortful breaths that signal immediate danger. Respiratory rate works like a warning light on a dashboard. Sometimes it points to a crisis that needs emergency care now. Sometimes it points to a slower problem involving sleep, airway stability, jaw function, or chronic over-breathing.
When an abnormal respiratory rate is an emergency
Some breathing changes belong in the emergency category because they can reflect serious problems with the airway, brain, heart, lungs, or acid-base balance.
Get emergency help right away if a breathing change comes with any of these signs:
- Blue or gray lips or skin
- Severe difficulty breathing
- Confusion or reduced responsiveness
- Chest retractions or visible struggle to pull air in
- Sudden slowing of breathing after opioid or sedative use
- Repeated pauses in breathing with failure to wake appropriately
- Very fast breathing with signs of serious illness
A good clinical rule is simple. If the person looks unstable, increasingly sleepy, hard to arouse, or is working hard to breathe, do not wait for a home tracking plan or a routine office visit. Deep, labored, unusually rapid breathing can happen when the body is trying to correct a dangerous internal imbalance. That pattern is an emergency signal.
When it is not an emergency, but still deserves evaluation
A large group of patients fall between “fine” and “ER.” They are functioning, but compensating.
This is the group that often gets missed in routine care. Their respiratory rate may run high at rest, drift upward during sleep, or become irregular during stress, pain, or exertion that should feel easy. They may not describe “breathing trouble” at all. They talk about jaw pain, clenching, headaches, poor sleep, dry mouth, fatigue, brain fog, or anxiety.
A focused evaluation makes sense when you notice patterns such as:
- Chronic snoring
- Observed breathing pauses during sleep
- Waking with headaches or a dry mouth
- Persistent daytime fatigue
- Jaw pain, clenching, or facial tension
- Restless sleep or frequent awakenings
- A consistently increased resting breathing rate
- A wearable that repeatedly flags unusual breathing trends
- A child with noisy sleep, mouth breathing, or concerns about oral development
These symptoms often get separated into different specialties, even when they may share the same driver. An unstable airway can disturb sleep. Poor sleep can raise pain sensitivity. Mouth breathing and low tongue posture can change how the jaw, neck, and ribcage work together. Over time, the body adapts, but the adaptation has a cost.
What root-cause solutions can look like
Root-cause care asks a different question. Instead of only asking how to suppress the symptom, it asks why the breathing pattern became inefficient in the first place.
That evaluation may lead to:
- Orofacial myofunctional therapy: Exercises and retraining for tongue posture, lip seal, swallowing pattern, and the muscle habits that help support a more stable airway.
- Breathing retraining, including Buteyko-based methods: Work aimed at reducing habitual over-breathing, improving nasal breathing, and decreasing unnecessary upper chest effort.
- Sleep-focused evaluation: Assessment of snoring, upper airway resistance, positional issues, and obstructive sleep apnea instead of assuming poor sleep is only stress-related.
- TMJ-focused care: Evaluation of whether clenching, joint strain, pain, or altered jaw position are affecting airway mechanics and breathing coordination.
- Pediatric airway assessment: Especially for children with mouth breathing, restless sleep, feeding difficulty, or oral posture concerns.
These approaches matter because breathing is not just a lung event. It is a whole-system behavior. The nose, tongue, palate, jaw, diaphragm, ribcage, and nervous system all have to coordinate, much like musicians in the same ensemble. If one section is out of rhythm, the whole performance becomes strained.
Why treating the root often changes more than breathing
As breathing mechanics improve, patients often report changes that seem unrelated at first. Morning jaw tension may ease. Headaches may become less frequent. Neck and chest tightness may settle. Sleep can feel deeper and less broken up. Daytime energy often improves when the body no longer spends so much effort compensating.
That is why respiratory rate is such a useful clue in chronic care. It is not the whole diagnosis. It is a signpost. In the right clinical context, it can point toward sleep-disordered breathing, dysfunctional breathing, TMJ-related compensation, or a mix of all three.
The number matters. The pattern matters more. Fast, slow, shallow, irregular, mouth-based, noisy, or effortful breathing can each show where the body is struggling to compensate.
Conclusion Reclaiming Your Health One Breath at a Time
Breathing rate looks simple because it’s easy to count. It’s not simple in what it reflects. Every breath is shaped by brain rhythm, metabolic chemistry, airway anatomy, posture, sleep quality, pain, and habit. When the rate becomes abnormal, the body is telling you something important.
Sometimes that message is urgent. Sometimes it’s chronic and easy to miss. That’s especially true for people with TMJ symptoms, snoring, sleep apnea, mouth breathing, facial pain, and fatigue. They may not look acutely ill, but their breathing may still be working harder than it should.
The key takeaway is this: an abnormal respiratory rate isn’t only an emergency-room concept. It can also be a quiet marker of dysfunctional breathing, upper airway resistance, poor oral posture, sleep fragmentation, or compensation driven by jaw and airway problems. When you understand that link, symptoms that once seemed unrelated start to make sense together.
Better breathing often requires more than telling someone to “relax” or handing them a one-size-fits-all appliance. It may call for careful assessment, sleep-focused investigation, breathing retraining, myofunctional therapy, or treatment that addresses TMJ strain and airway mechanics together.
If you’re a patient, trust your pattern when it keeps repeating. If you’re a referring clinician, consider respiratory rate and breathing mechanics as part of the bigger picture in chronic pain, fatigue, and sleep cases. A resting breath pattern can reveal what many standard visits miss.
If you’re dealing with snoring, sleep apnea, jaw pain, chronic headaches, mouth breathing, or fatigue that no one has fully connected, Pain and Sleep Therapy Center offers thorough evaluation focused on root causes. Their team works across TMJ care, airway assessment, myofunctional therapy, breathing retraining, and non-surgical sleep solutions to help patients and referring providers find answers that fit the whole person.



