
A feeding session shouldn't leave a parent dreading the next one. Yet that's where many families start. The baby clicks and slips off the breast or bottle, feeds take forever, everyone ends up exhausted, and then the questions begin. Is this reflux, colic, milk supply, bottle flow, or something else no one has spotted yet?
Older children can look different but feel just as confusing. A toddler gags on textured foods. A preschooler chews with effort, keeps the mouth open at rest, snores, or sleeps restlessly. A school-age child speaks clearly enough to get by, but seems tense through the jaw, neck, and face. In some of these children, the common thread is a restrictive frenulum.
A pediatric frenectomy is a procedure used to release a tongue-tie or lip-tie when that tissue restriction is limiting function. The key word is function. The question isn't whether a tie is visible. The question is whether it's affecting feeding, swallowing, oral posture, breathing, sleep, or development over time.
The Hidden Reason Behind Your Child's Struggles
Some families arrive after weeks of nursing pain and poor weight gain. Others come in after trying different bottles, positions, burping routines, and reflux strategies with little relief. They're often carrying the same worry. “I know something isn't right, but I can't tell what.”
When feeding looks harder than it should
A restrictive oral frenulum can interfere with the simple mechanics babies rely on. The tongue needs to lift, extend, cup, and seal. The lips need to flange and stabilize. When those movements are limited, feeding can become noisy, inefficient, and tiring for both parent and child.
Common stories sound familiar:
- Breastfeeding feels painful: The latch stays shallow, nipples come out compressed, and feeds don't feel productive.
- Bottle feeding still isn't easy: Even with careful nipple selection, milk transfer seems disorganized or messy. If you're sorting through bottle options, these essential baby bottle tips for parents can help you think through flow, shape, and fit.
- Sleep gets disrupted early: A baby who swallows excess air, feeds constantly, or never seems fully satisfied may also sleep in short, unsettled stretches. Families trying to build calmer bedtime routines later on may also appreciate these ideas for improving kids' bedtime book choices, especially when overtired children are already hard to settle.
None of this means a parent caused the problem. It means the feeding system may be working against them.
A visible tie isn't the diagnosis by itself. The diagnosis comes from matching anatomy to real-life functional problems.
Why more families are hearing about tongue-tie
Awareness has increased sharply. The frequency of frenulum procedures in the United States rose by 866% between 1997 and 2012, a trend largely attributed to greater clinical recognition, especially around infant breastfeeding difficulties, according to the American Academy of Pediatric Dentistry policy document.
That rise creates two opposite problems. Some families feel dismissed because symptoms are attributed to normal newborn fussiness. Others get told a tie is present and assume surgery is automatically the answer. Neither extreme is helpful.
A careful evaluation matters because not every restriction needs release, and not every feeding problem comes from the frenulum. When complications do exist, it helps to understand the broader picture, including the functional issues described in this guide to tongue-tie complications.
Signs Your Child May Have a Tongue or Lip Tie
Parents usually notice patterns before anyone names them. Referring doctors often hear a list of symptoms that seem unrelated until they're viewed through a feeding and airway lens. Looking for signs by age helps.
A quick visual can help organize what you're seeing:
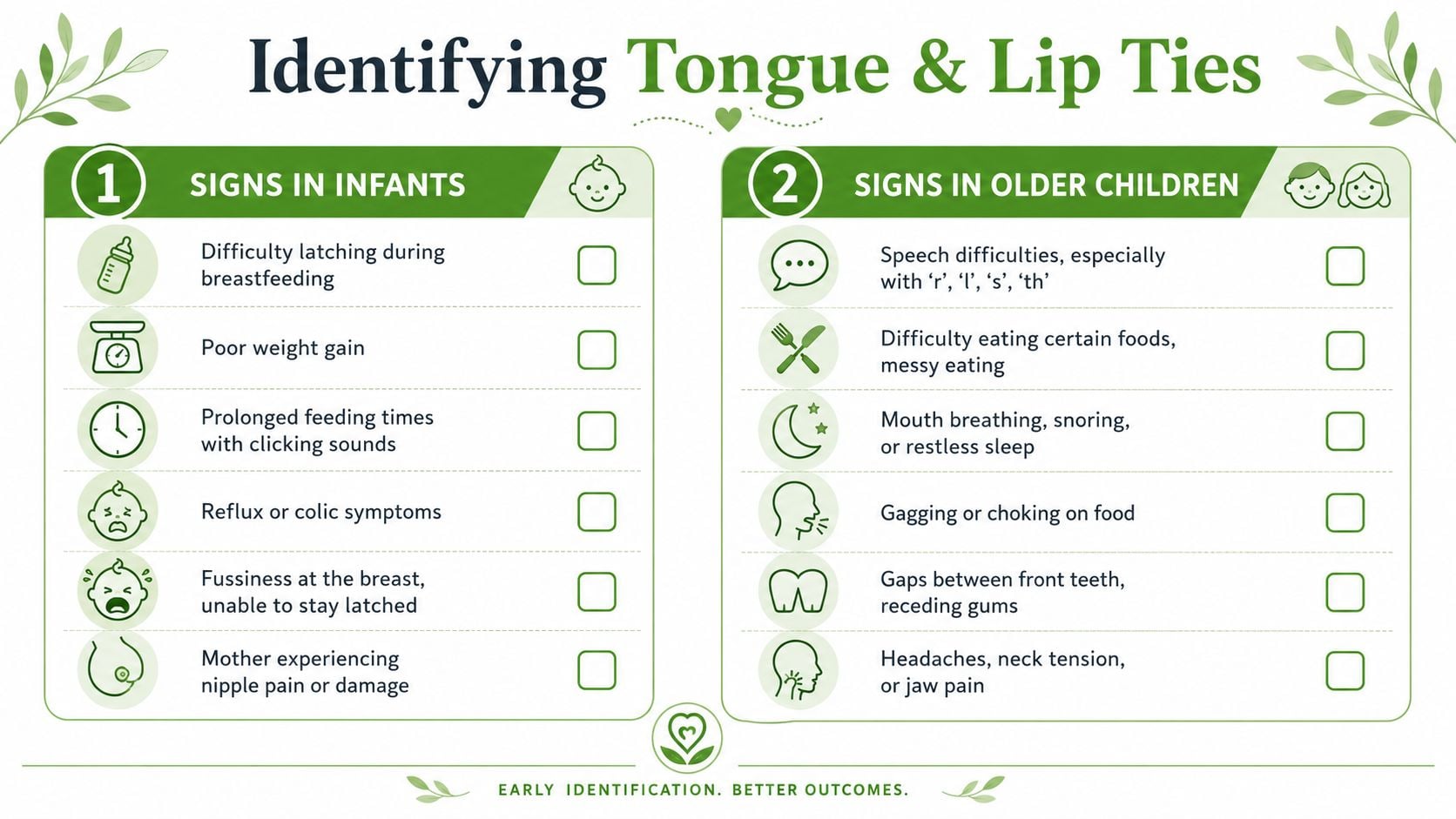
Signs in infants
In infants, the strongest reason to evaluate early is function during feeding. Research found that the rise in frenotomy referrals and procedures was driven primarily by feeding concerns in infants (P < 0.0001), while procedures for speech-related issues did not show a similar increase (P = 0.13) in the cited study on pediatric frenectomy trends in International Journal of Pediatric Otorhinolaryngology.
What families often notice first:
- Shallow latch or repeated loss of latch: The baby grabs, slips, re-latches, and never settles into a smooth rhythm.
- Clicking during feeds: That sound usually signals loss of seal.
- Long feeds with poor transfer: The baby works hard but doesn't seem satisfied.
- Excess gas, reflux-like behavior, or colic symptoms: Air intake often increases when the seal is unstable.
- Nipple pain or damage for the breastfeeding parent: Friction replaces efficient tongue movement.
- Poor weight gain or fatigue during feeds: The baby spends energy without efficient intake.
If you're trying to sort out whether these signs point toward a restriction, this overview on how to tell if baby has tongue-tie can help frame what deserves a closer look.
This video offers a useful visual overview for parents who want to understand what these restrictions can look like in real life.
Signs in toddlers and older children
The presentation changes with age. By then, the concern may no longer be latch. It may be compensation.
Watch for patterns like these:
- Difficulty with solids: Gagging, pocketing food, chewing with effort, or avoiding certain textures.
- Messy eating: Food spills because the lips and tongue can't coordinate well.
- Speech concerns: Not every articulation issue comes from a tie, but limited tongue range can contribute in selected cases.
- Open-mouth posture: Lips apart at rest can signal poor oral posture or airway strain.
- Mouth breathing, snoring, or restless sleep: These signs deserve attention because tongue posture and breathing are linked.
- Jaw, neck, or facial tension: Some children recruit other muscles to compensate for limited tongue mobility.
Parents often say, “I thought my child was just a picky eater.” Sometimes that's true. Sometimes the child is avoiding foods that are physically hard to manage.
What matters most
A tie becomes clinically meaningful when it changes what a child can do. That means a good assessment doesn't stop at appearance. It asks whether the tongue can lift, whether the lips can seal, whether swallowing is coordinated, and whether the child can breathe comfortably with the mouth closed.
Our Comprehensive Evaluation Process
A proper tongue-tie evaluation shouldn't feel rushed. A quick glance under the tongue can identify tissue, but it can miss the larger question. Is this structure restricting function in a way that explains the child's symptoms?
That's why a thorough assessment blends anatomy with observation.
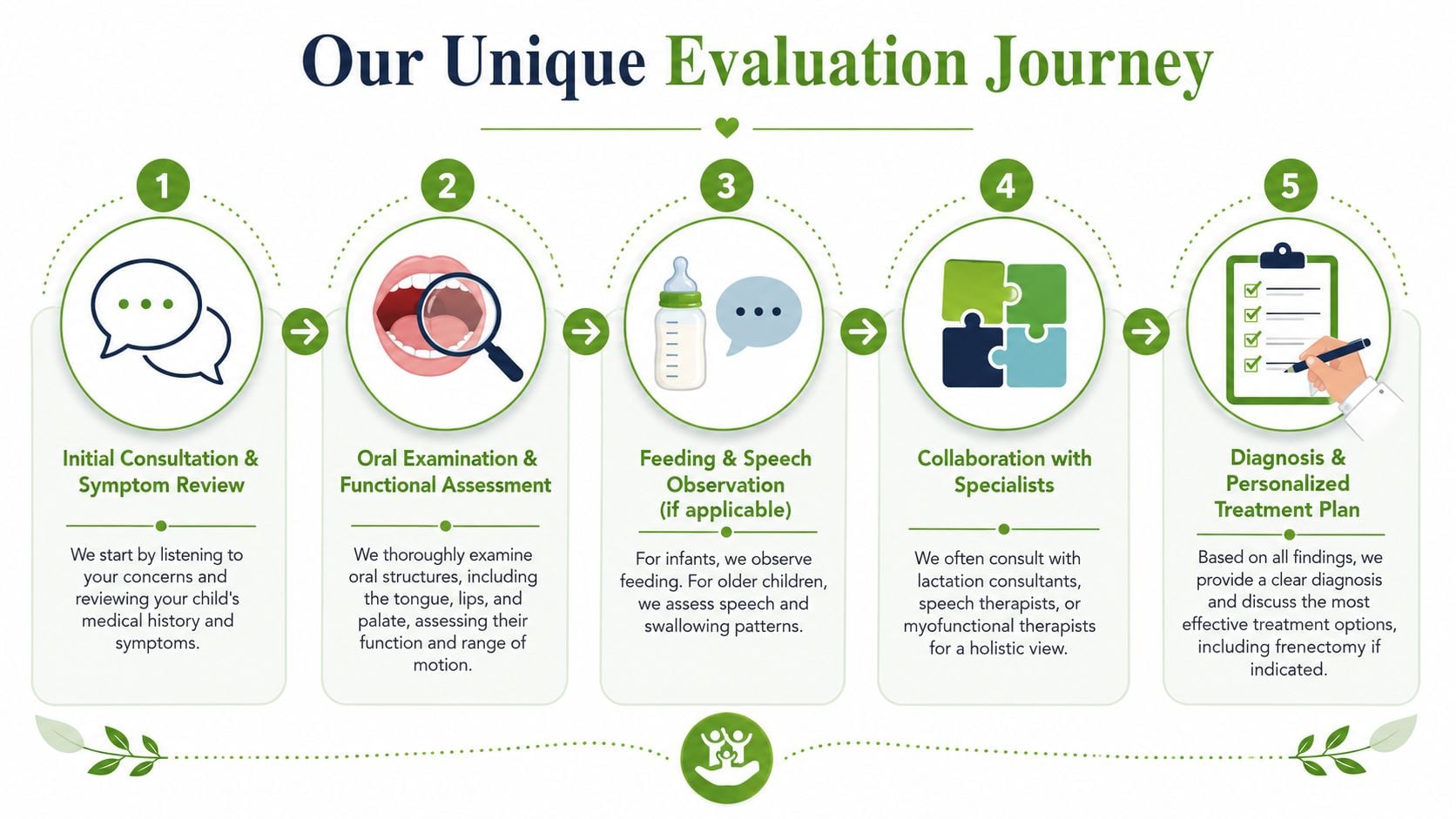
What a meaningful exam includes
A complete workup usually starts with history. Feeding history matters. Pregnancy and birth history may matter. Sleep symptoms, oral habits, reflux concerns, speech history, congestion, posture, and previous therapies all add context.
Then comes the functional exam. That usually includes:
- Tongue mobility: Can the tongue lift, extend, lateralize, and maintain suction when needed?
- Lip mobility and seal: Does the upper lip flange and rest well, or is compensation obvious?
- Palate and oral structure: A narrow palate, poor tongue rest posture, or chronic open-mouth posture can change how symptoms show up.
- Swallowing pattern: Some children push forward, thrust, or recruit the lips and jaw excessively.
- Breathing pattern: Nasal breathing versus mouth breathing is never a trivial detail in this setting.
Why observation changes the diagnosis
For infants, watching a feed can reveal more than a static exam. You can see seal loss, jaw fatigue, noisy swallowing, poor rhythm, or compensatory body tension. For older children, speech, chewing, and swallowing tasks often tell the story more clearly than the tissue band alone.
A narrow approach asks, “Is there a tie?”
A better approach asks:
| Question | Why it matters |
|---|---|
| What function is limited | Treatment should solve a real problem, not a cosmetic finding |
| What compensations are present | Children often adapt in ways that hide the restriction |
| What else is contributing | Airway issues, muscle tension, and habit patterns can coexist |
| Will release alone help | Some children need therapy before and after the procedure |
The best pediatric frenectomy decisions come from matching symptoms, exam findings, and functional goals. Tissue alone isn't enough.
Why this matters for parents and referring doctors
This kind of evaluation protects children in both directions. It prevents unnecessary procedures when the frenulum isn't the true driver. It also prevents under-treatment when the tie is part of a bigger pattern involving feeding, oral posture, breathing, and sleep.
For referring providers, that root-cause lens matters. It creates a clearer handoff, a more targeted procedure when one is indicated, and a better recovery plan because everyone understands what improvement should look like.
The Laser Frenectomy Procedure Explained
Once a child is identified as a good candidate, the next concern is usually simple. What happens during the procedure, and how is it different from older methods?
A laser pediatric frenectomy releases restrictive tissue with controlled precision. The aim isn't to create a larger wound. The aim is to free movement while minimizing collateral trauma.
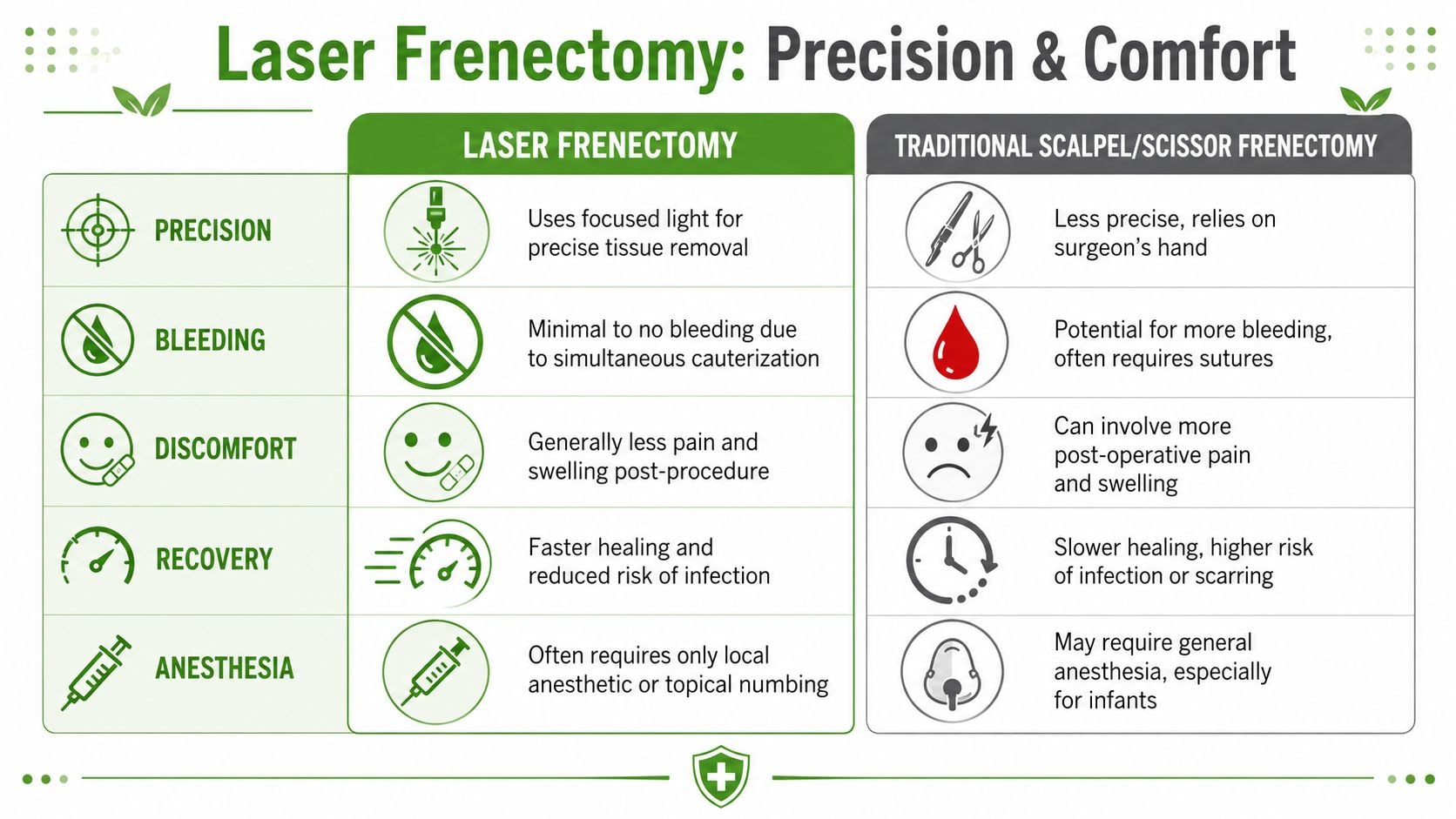
How laser treatment differs from scissors or a scalpel
Traditional scissors or scalpel release can still be effective in the right hands. But the experience for the child and family often differs in important ways.
A diode laser allows the clinician to release dense fibrous tissue while simultaneously coagulating small vessels. In the pediatric case series cited in the verified data, diode laser-assisted lingual frenectomy showed minimal bleeding, often less than 0.5 mL, no need for sutures, and significantly reduced postoperative pain, with rapid healing and immediate improvement in tongue mobility according to the PubMed Central article on diode laser frenectomy.
Here's the practical comparison:
| Feature | Laser frenectomy | Traditional scissors or scalpel |
|---|---|---|
| Tissue handling | Precise, targeted release | More mechanical cutting |
| Bleeding | Minimal because tissue is cauterized | Usually more bleeding |
| Sutures | Commonly not needed | More likely to be needed |
| Post-op comfort | Typically easier for children | Often more swelling or soreness |
| Healing environment | Clean wound bed with less disruption | More raw tissue surface |
What parents can expect
The procedure itself is short. The child is positioned securely, the area is numbed appropriately, and the restrictive tissue is released in a controlled way. In infants, the goal is often improved mobility for feeding. In older children, the goal may include oral function, tongue posture, swallowing mechanics, and breathing patterns.
Parents are often surprised by what doesn't happen:
- There usually isn't heavy bleeding
- There usually aren't stitches
- There usually isn't the degree of post-op distress parents feared
That doesn't make it casual. It still requires skill, planning, and follow-up. But it is often gentler than families imagine.
What laser can and cannot do
Laser technology solves several technical problems well. It improves visibility, reduces bleeding, and can make recovery more manageable. It does not replace proper diagnosis, careful wound management, or therapy when the child has developed compensatory patterns.
Practical rule: A precise release helps, but a release alone won't retrain a child who has learned to swallow, breathe, or rest the tongue the wrong way for months or years.
That distinction matters. The procedure removes the restriction. The rest of care teaches the child how to use the new freedom.
Why Post-Procedure Care Is Not Optional
The procedure is the mechanical release. Recovery is the functional treatment.
Many otherwise promising outcomes can be compromised. Families are relieved the tie has been released, but the mouth heals quickly, and healing tissue tends to contract. If wound care and retraining are skipped, the old restriction can return in the form of scar tissue or the child can keep using the same compensations as before.
The biology behind reattachment
A wound in the mouth doesn't stay open on its own. It contracts as it heals. That's why post-op exercises matter so much.
The verified data notes that a frenectomy carries a 15-20% higher risk of scar tissue re-attachment if it is not immediately followed by rigorous, specific stretching exercises and myofunctional therapy, compared with a less extensive frenotomy. That's the difference between a technically successful procedure and a lasting functional result.
Parents who want a clearer idea of the day-to-day healing process often benefit from reviewing this guide on tongue-tie surgery recovery.
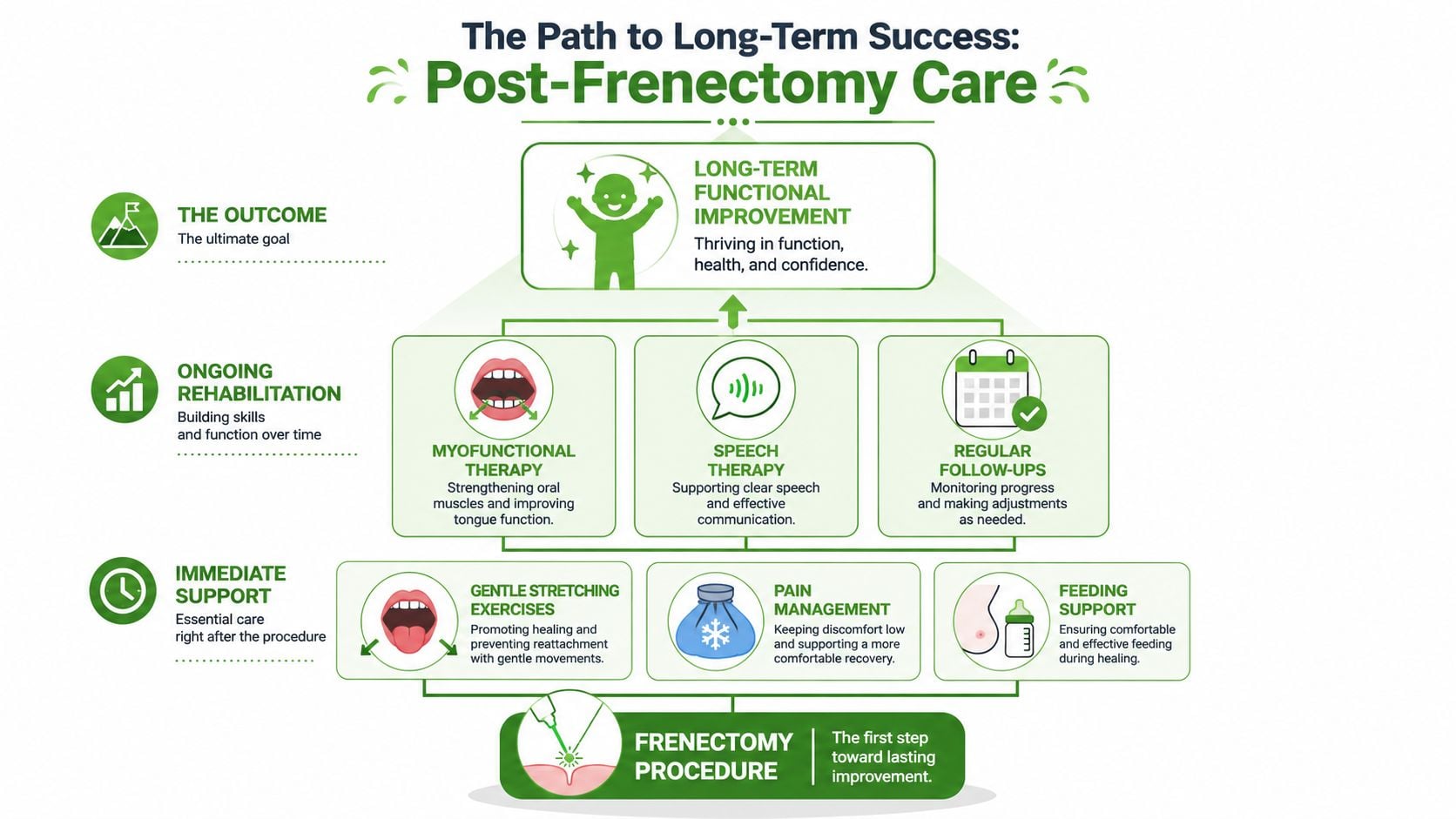
The two pieces that protect the result
The first piece is active wound management. These are the stretches or lifts recommended right after the procedure. They are specific, time-sensitive, and often uncomfortable to think about as a parent. But they serve a clear purpose. They keep healing tissue from knitting back together in a restrictive way.
The second piece is orofacial myofunctional therapy or related functional therapy. That work may include:
- Tongue elevation practice: Helping the tongue learn where it belongs at rest
- Swallow retraining: Reducing lip, chin, and jaw compensation
- Lip seal work: Supporting closed-mouth posture
- Breathing exercises: Encouraging nasal breathing when medically appropriate
- Feeding integration: Helping infants and children use the new range of motion in real feeding tasks
What doesn't work
A few approaches commonly fall short:
- Releasing the tie without aftercare: The tissue may heal back down or function may not improve as expected.
- Doing stretches without addressing habits: The wound stays open, but the child still swallows, breathes, or rests the tongue the same old way.
- Waiting for function to “just improve” on its own: Some children adapt beautifully. Others need guided retraining.
“The release creates access. Therapy creates the pattern.”
That's why post-op care should be discussed before the procedure, not after it. Parents need to know what recovery asks of them. Referring doctors need to know whether the child will have a structured plan for stretches, feeding support, and myofunctional follow-up.
Connecting Today's Care to Lifelong Health
A restrictive frenulum can start as a feeding problem and later show up as an oral posture, chewing, or sleep problem. That doesn't mean every tongue-tie leads to major airway disease. It does mean the tongue plays a larger role in growth and breathing than many families realize.
When the tongue rests well against the palate, it supports normal oral function and helps maintain a healthier breathing pattern. When it can't lift well, children may compensate with low tongue posture, lip separation, mouth breathing, and inefficient swallowing. Over time, those patterns can affect comfort, sleep quality, and facial development.
Why airway and sleep belong in the conversation
This is the part many standard frenectomy discussions leave out. The procedure is often framed around feeding alone, especially in infancy. Feeding matters. But airway matters too.
The verified data identifies a major research gap here. It also notes that 30-40% of children with mild-to-moderate obstructive sleep apnea had previously undiagnosed lingual frenulum restrictions, while emphasizing that extensive long-term data is still needed to quantify how much frenectomy changes future OSA risk. That makes one thing clear. The airway connection deserves attention, even if the literature hasn't answered every long-term question yet.
A thoughtful way to think about prevention
A pediatric frenectomy shouldn't be sold as a guaranteed way to prevent future sleep apnea. That would go beyond the evidence. But it is reasonable to view tongue mobility as one piece of a child's long-term airway picture, especially when paired with oral posture, nasal breathing, swallowing mechanics, and growth guidance.
For families already focused on whole-child development, broader wellness habits matter too. Supportive routines around feeding, sleep, and caregiver health all contribute to a stronger foundation. For example, this article on maternal wellness for infant brain health offers helpful context for the bigger developmental picture.
The right goal isn't just to “clip a tie.” The goal is to help a child feed better, breathe better, sleep better, and grow with fewer compensations.
If you're concerned that a tongue-tie or lip-tie may be affecting your child's feeding, oral development, or sleep, Pain and Sleep Therapy Center offers airway-focused pediatric evaluation and laser frenectomy care designed around root-cause treatment. Their team looks beyond the visible tie to assess function, breathing, posture, and long-term health so families and referring providers can make clear, confident decisions.



