
Your child goes to bed on time, sleeps what looks like a full night, and still wakes up exhausted. School gets harder. Mornings get combative. Mood swings show up out of nowhere. Some children snore. Others don't. Some look hyperactive instead of sleepy. Others grind their teeth, breathe through their mouths, or toss all night.
That's where pediatric sleep medicine becomes important. It isn't just about “sleep problems” in the casual sense. It's the clinical work of finding out why a child isn't getting restorative sleep, then matching treatment to the actual cause.
For parents, that often brings relief. For referring doctors, it creates a clearer path forward when symptoms don't fit neatly into one box.
What Is Pediatric Sleep Medicine
A child can sleep nine or ten hours and still wake up unrested. In clinic, that pattern often leads families down the wrong path first. They may focus on bedtime alone, when the bigger issue is how the child is breathing, regulating sleep, or maintaining an open airway through the night.
Pediatric sleep medicine evaluates those patterns in the context of a child's whole development. It sits at the intersection of breathing, neurology, behavior, growth, and daily function. Children rarely present the way adults do. Instead of looking sleepy, they may look wired, distracted, irritable, or hard to settle.
The central question is straightforward: what is interfering with restorative sleep, normal sleep timing, or safe breathing during sleep?
That question matters because many children with meaningful sleep problems are never identified early. In practice, I see referrals for snoring, teeth grinding, mouth breathing, night waking, insomnia, delayed sleep schedules, and daytime behavior concerns. Sometimes one symptom points clearly to the problem. Often it does not.
It covers more than bedtime routines and more than tonsils
Parents and referring clinicians often start with the most visible complaint. Snoring. Bedtime resistance. Night sweats. Restless sleep. Those details matter, but pediatric sleep medicine goes further by asking what is driving them.
A child may have obstructive sleep apnea or another form of sleep-disordered breathing. Another may have circadian disruption, behavioral insomnia, parasomnias, restless sleep, or more than one condition at the same time. Some children also have contributing factors outside the sleep lab, including chronic nasal obstruction, low tongue posture, mouth breathing, poor oral rest posture, or narrow jaw development that affects airway size and stability. If you are sorting through child sleep apnea symptoms, those structural and functional clues are often part of the picture.
This is why treatment should not stop at naming the disorder. A tonsil and adenoid evaluation may be appropriate. So may orthodontic assessment, myofunctional therapy, allergy care, behavioral sleep support, or a closer look at craniofacial growth and oral function. Families exploring dental contributions to airway treatment sometimes review resources such as 3D Dental sleep apnea options.
The primary goal
The primary goal of pediatric sleep medicine is to restore healthy function, not to assign a label.
That means looking at how sleep affects:
- Attention, learning, and school performance
- Mood, behavior, and emotional regulation
- Breathing quality during sleep and wakefulness
- Growth of the face, jaws, and oral function
- Family stress when nights are fragmented or unpredictable
Good care starts with root cause analysis. Then it builds a treatment plan around the child in front of us. That multidisciplinary approach is a major part of modern pediatric sleep medicine, especially for children whose symptoms involve both airway and function, not just sleep duration alone.
Common Pediatric Sleep Disorders Explained
A child can snore, fight bedtime, wake screaming, and still have more than one problem contributing to the same rough night. That is why pediatric sleep medicine separates disorders by mechanism. The label matters because the next step depends on what is disrupting sleep.
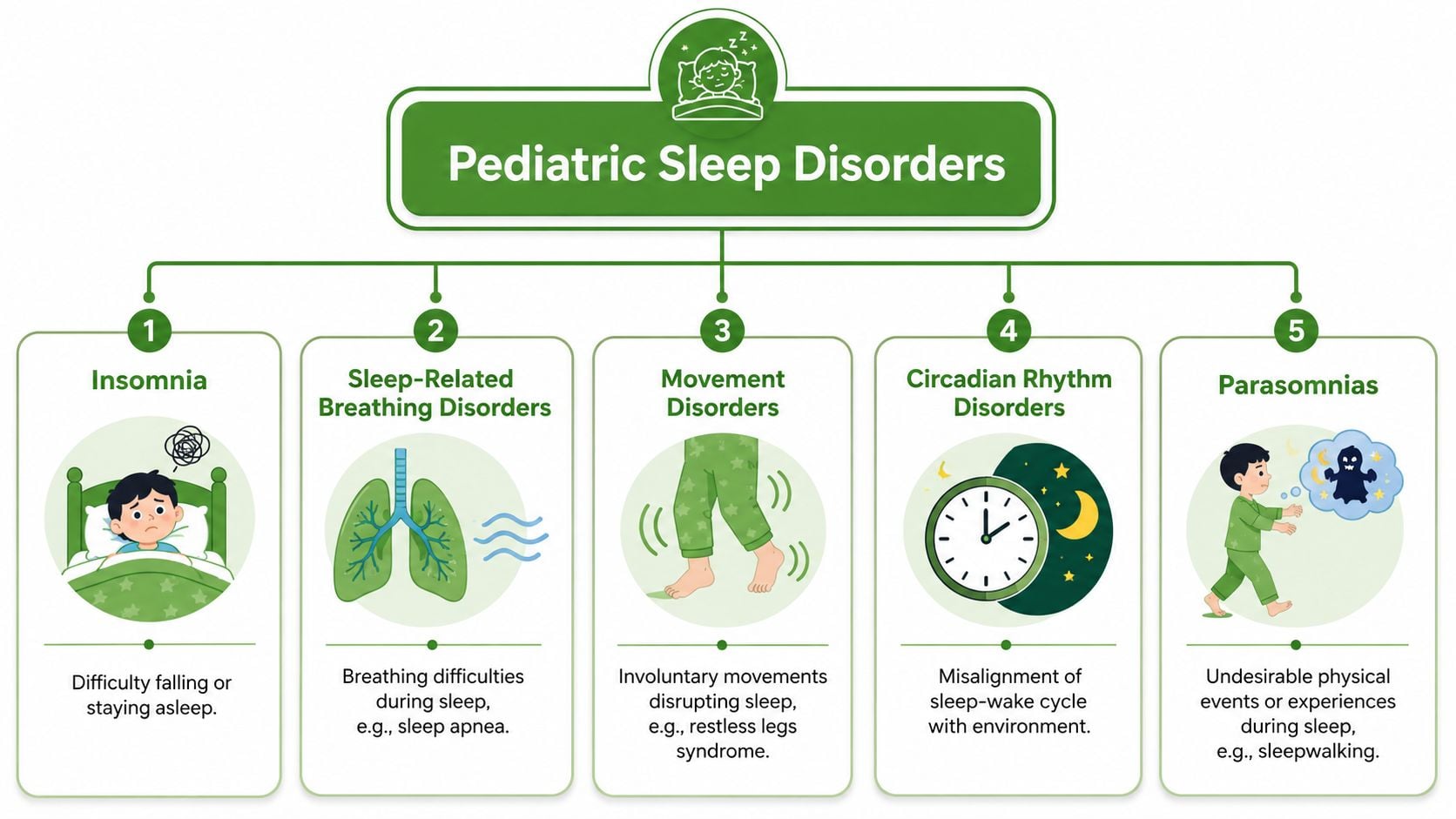
Some sleep disorders primarily affect breathing. Others affect arousal, circadian timing, or learned sleep patterns. In practice, children often have overlap. A child with airway obstruction may also develop bedtime resistance because sleep feels uncomfortable. A child with chronic sleep loss may have more parasomnias. Good evaluation starts by sorting out which problem is primary and which problems developed around it.
Obstructive sleep apnea
Obstructive sleep apnea, or OSA, happens when the upper airway narrows or closes during sleep. Breathing effort continues, but airflow becomes limited.
Enlarged tonsils and adenoids are common contributors. They are not the whole story. Nasal blockage, chronic mouth breathing, low tongue posture, narrow jaw development, and poor oral function can all reduce airway stability. This is one reason I do not treat every snoring child as a simple surgical referral. Some children need ENT care. Some need orthodontic or dental airway evaluation, myofunctional therapy, allergy treatment, weight assessment, or a combination of these.
Typical features include:
- Habitual snoring
- Pauses in breathing, gasping, or increased work of breathing
- Restless sleep or unusual sleep positions
- Morning headaches, irritability, or attention problems
Families who want to better understand airway-related symptom patterns can review these child sleep apnea symptoms. For those exploring how oral anatomy may fit into treatment planning, 3D Dental sleep apnea options offers a useful overview.
Central sleep apnea
Central sleep apnea has a different mechanism. The problem is not airway collapse. The brain's signaling to breathe becomes inconsistent during sleep, so breathing pauses occur without the obstructive pattern seen in OSA.
That difference changes the workup. Central events may call for closer review of age, prematurity history, neurologic factors, medications, cardiac or pulmonary issues, and the child's sleep study pattern. In infants, brief central pauses can be normal. In older children, repeated central events deserve a more specific explanation.
Parasomnias
Parasomnias include sleepwalking, confusional arousals, night terrors, and related behaviors that arise out of sleep. These episodes can look alarming, especially when a child seems awake but is confused, inconsolable, or hard to redirect.
Many parasomnias are benign. They also become more frequent when sleep is fragmented. I often see them intensified by sleep deprivation, obstructive breathing, fever, stress, or an irregular sleep schedule. When the episodes are frequent, prolonged, or atypical, the goal is to identify the trigger rather than assume the behavior itself is the whole diagnosis.
Behavioral insomnia
Behavioral insomnia describes persistent difficulty falling asleep or returning to sleep because of learned sleep associations, bedtime resistance, or inconsistent routines. This is common in pediatrics, but it should not be dismissed.
Some children need structured behavior change and parent coaching. Others have an underlying reason they cannot settle, such as nasal obstruction, reflux, eczema, anxiety, sensory dysregulation, or discomfort with lying flat and breathing through a restricted airway. If a child cannot sleep without a parent, I want to know whether that is purely behavioral or whether sleep has become associated with distress.
Restless sleep and movement-related disorders
Some children are not snoring, but they still sleep poorly because their sleep is physically unsettled. Restless legs symptoms, periodic limb movements, and frequent tossing or kicking can fragment sleep and leave a child tired, moody, or unable to focus during the day.
This category deserves attention because it is easy to miss. Parents may describe the child as a wild sleeper, but the underlying issue may involve sensory discomfort, iron deficiency, medication effects, or another sleep disorder disrupting sleep continuity.
Why the distinction matters
Children do better when the diagnosis reflects the underlying cause. Snoring does not automatically mean surgery. Bedtime struggles do not automatically mean stricter routines. Dramatic nighttime behaviors do not automatically point to a neurologic disorder.
The most useful question is simple: what is keeping this child from getting stable, restorative sleep, and which systems are involved? In many cases, the answer includes more than one specialty.
Signs Parents and Providers Should Not Ignore
Children rarely announce that their sleep quality is poor. They show it through patterns. Some of those patterns appear at night. Others show up in the classroom, at the dinner table, or during the morning rush.
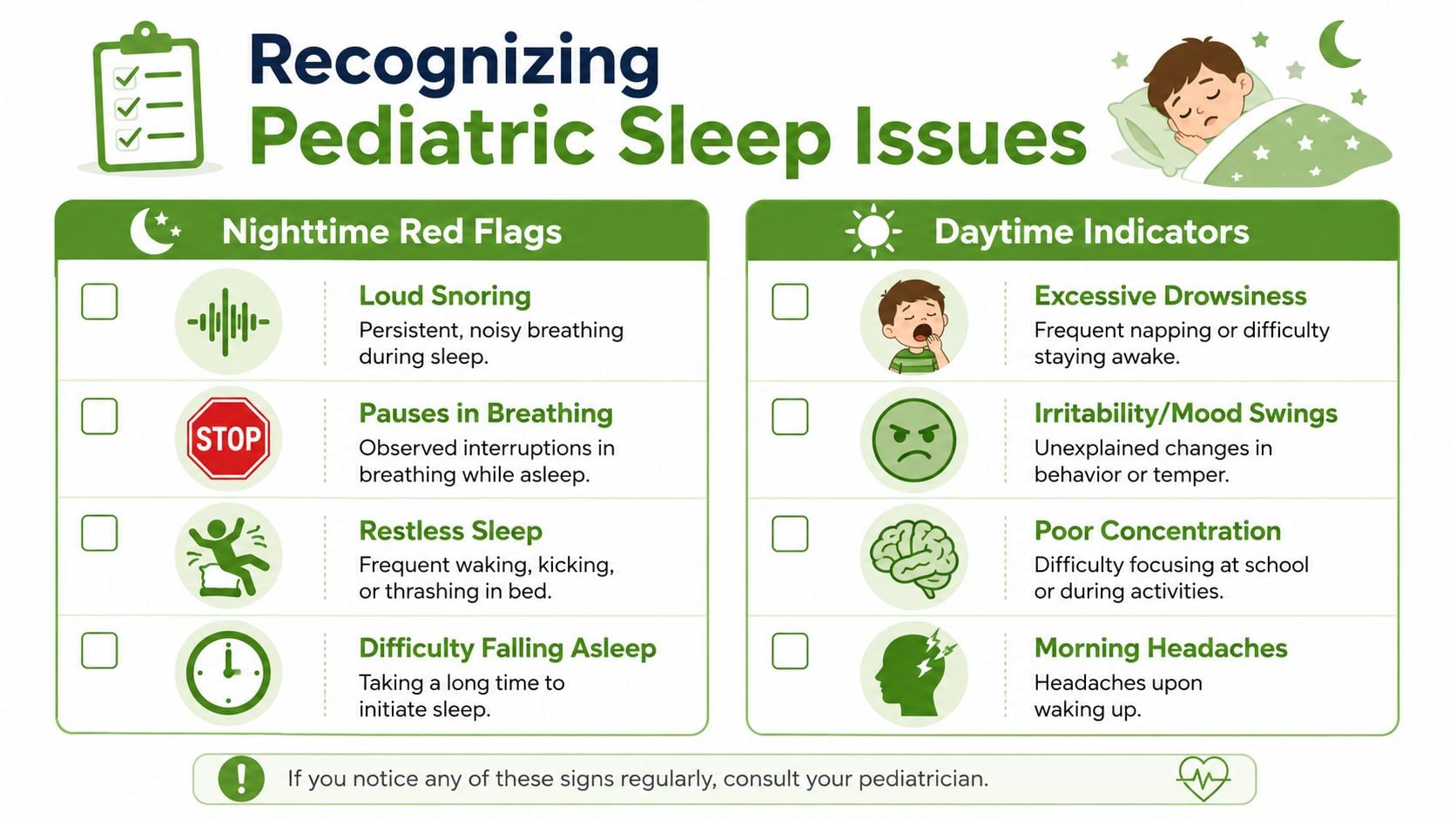
Nighttime red flags
These are the signs that often prompt an evaluation first:
- Loud snoring that happens regularly rather than only with a cold
- Pauses in breathing, gasping, or choking sounds
- Restless sleep with kicking, thrashing, unusual positions, or frequent waking
- Trouble falling asleep that becomes a repeated pattern
- Sweaty sleep or a child who seems to work hard to breathe
- Bedwetting when other sleep-disordered breathing clues are present
Some children also sleep with their mouths open all night or seem unable to maintain quiet nasal breathing.
Daytime clues that are easy to miss
Poor sleep in children often hides behind behavior. Instead of obvious drowsiness, many children look “wired.”
Watch for:
- Hyperactivity or impulsivity that worsens when sleep is poor
- Irritability and emotional swings
- Poor concentration or inconsistent school performance
- Morning headaches
- Fatigue that shows up as low frustration tolerance
- Chronic mouth breathing during the day
- Bruxism, or teeth grinding, especially when paired with other airway concerns
A broader pediatric sleep evaluation should include symptoms such as fragmented sleep, behavior changes, bruxism, and mouth breathing because untreated sleep disruption is linked to depression, anxiety, diabetes, and hypertension, as described in this UNM Health overview of pediatric sleep evaluation.
A short visual explanation can help families recognize patterns they've normalized over time:
Why these signs matter together
One symptom by itself may be nonspecific. A child who grinds teeth could be stressed. A child who mouth breathes could have nasal congestion. A child who's irritable could be overtired.
The clinical picture changes when those clues cluster. Snoring plus bruxism plus morning moodiness points in a different direction than bedtime resistance alone. That's why both parents and providers should think in patterns rather than isolated complaints.
The Diagnostic Journey to Uncover Root Causes
A useful sleep evaluation feels less like a single test and more like a structured investigation. The aim isn't to confirm a suspicion as quickly as possible. It's to understand what is driving the child's symptoms.

What a sleep study can tell you
For suspected obstructive sleep apnea and other complex sleep disorders, overnight polysomnography, or PSG, is the gold-standard test. It records brain waves through EEG, cardiac rhythm through EKG, muscle tone through EMG, and respiratory signals during sleep, which is why it can sort out problems that symptoms alone can't define, as explained in this Yale Medicine overview of pediatric sleep studies.
That matters because children don't always fit adult screening assumptions. Parents may report “restless sleep,” but PSG can show whether that restlessness is coming from obstructive events, central events, limb movements, parasomnias, or something else entirely.
Why the physical exam still matters
A PSG answers important questions, but it doesn't replace a careful clinical exam.
In root-cause pediatric sleep medicine, clinicians often assess:
- Nasal breathing and whether airflow is consistently restricted
- Oral posture at rest, including open-mouth posture
- Tongue mobility and function, especially when restriction affects swallow or palate development
- Jaw and facial development, which can influence airway space
- Sleep behaviors and routines, because not every problem is anatomical
A normal-looking bedtime routine doesn't rule out a breathing problem. A positive sleep study doesn't tell you why the airway is unstable.
The stepwise workup
A thorough process often includes a blend of history, observation, and targeted testing.
| Step | What clinicians look for | Why it matters |
|---|---|---|
| History | Snoring, night waking, daytime behavior, school concerns, mouth breathing | Symptoms help define the pattern |
| Exam | Airway, tonsils, nasal obstruction, oral posture, tongue function, craniofacial features | Structure and function both affect sleep |
| Objective testing | PSG when symptoms are complex or severity is unclear | Confirms event type and severity |
| Functional review | Breathing habits, swallowing, muscle use, sleep schedule | Guides treatment beyond diagnosis |
When symptoms point toward a broader breathing and function issue, families may benefit from a more thorough sleep quality assessment rather than assuming the answer is only behavioral or only surgical.
The diagnosis should do more than name a disorder. It should explain the mechanism. That's what makes treatment precise.
A Team Approach to Pediatric Sleep Treatment
Children do best when treatment follows the cause. That sounds obvious, but pediatric sleep care often gets reduced to a narrow menu: remove tonsils, try CPAP, or wait and see. Those options matter, but they don't cover the full range of root-cause care.
A stronger model is multidisciplinary. Pediatric programs commonly involve pulmonary medicine, neurology, otolaryngology, and psychology because sleep-disordered breathing may reflect upper-airway or craniofacial factors rather than one isolated issue, as noted in this MedStar overview of multidisciplinary pediatric sleep care.
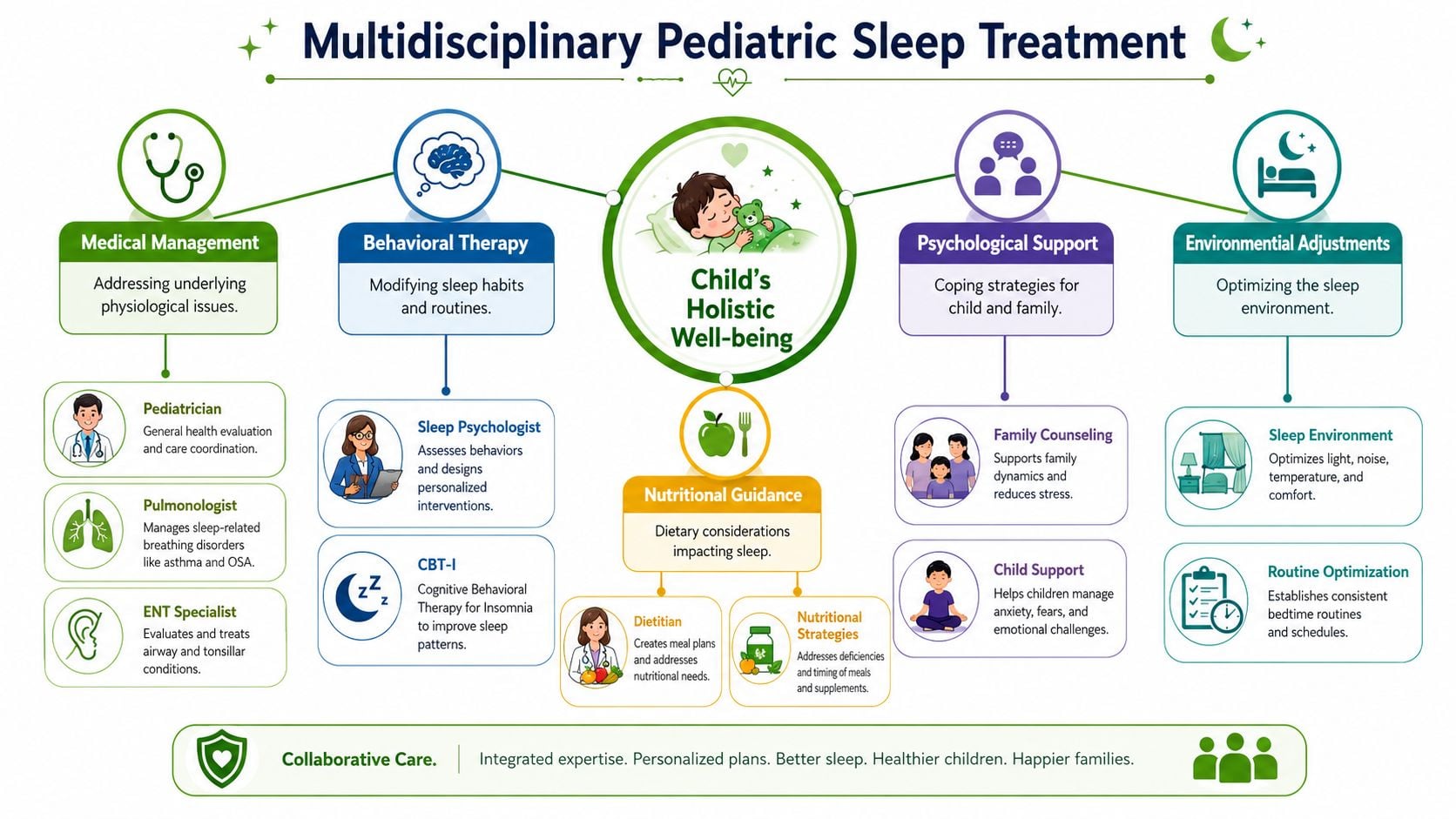
What different specialists contribute
An airway-related sleep problem may need several lenses at once.
- ENT evaluation can identify adenotonsillar enlargement, nasal obstruction, and structural airway contributors.
- Sleep medicine and pulmonary input help interpret breathing patterns, sleep study findings, and the need for therapies such as PAP support.
- Neurology becomes important when events are atypical, central breathing concerns are present, or seizures need to be distinguished from sleep phenomena.
- Psychology or behavioral sleep support helps when insomnia, sleep anxiety, or habit-based waking patterns are part of the picture.
- Dental and oral function assessment can add value when jaw development, oral posture, tongue restriction, or bruxism appear connected to airway stability.
What works and what doesn't
Some treatments are highly effective when the indication is right. They're disappointing when used as catch-all solutions.
Tonsils and adenoids can be central, but not always sufficient
If enlarged tonsils or adenoids are the main source of obstruction, surgery may be appropriate. But surgery doesn't retrain nasal breathing, correct low tongue posture, or resolve every craniofacial contributor. Children with persistent mouth breathing or poor oral function after surgery often need further evaluation.
CPAP can stabilize breathing, but adherence matters
PAP therapy can be very helpful, especially when obstruction persists or surgery isn't the right answer. The problem isn't the machine. The problem is expecting a child to tolerate it without adequate support, mask fitting, coaching, and follow-up.
Behavioral work is essential when sleep habits are part of the problem
If a child has insomnia, prolonged sleep-onset struggles, or repeated parent-dependent wakings, behavior-based treatment matters. But behavioral strategies won't fix a physically unstable airway. Sleep training is a poor substitute for airway evaluation when clear breathing signs are present.
Root-cause therapies that are often overlooked
In this context, pediatric sleep medicine becomes more individualized.
A child with chronic mouth breathing may need work on nasal breathing habits and oral rest posture. A child with a restricted tongue may need careful evaluation of function, not just anatomy. A child with narrow arches or poor tongue-palate contact may need collaboration between dental, orthodontic, and myofunctional providers.
Depending on the child, that plan may include:
- Orofacial myofunctional therapy to improve tongue posture, lip seal, swallow pattern, and airway-supportive muscle function
- Airway-focused orthodontic planning when jaw and palate development contribute to breathing compromise
- Breathing retraining, including Buteyko-informed techniques, when dysfunctional breathing habits reinforce mouth breathing
- Laser frenectomy evaluation in selected cases where tongue restriction clearly affects feeding, oral function, or airway-related development
The best treatment plan is often layered. Structural treatment, functional therapy, and sleep-specific care may all be necessary.
One example of this type of coordinated model is Pain and Sleep Therapy Center, which evaluates sleep-related breathing issues alongside oral posture, tongue function, myofunctional patterns, and airway-focused dental findings as part of a broader referral network. That kind of setup doesn't replace ENT, pulmonary, or neurology care. It complements them when the child's symptoms point to more than one driver.
The practical trade-off
A one-specialist model is simpler. A multidisciplinary model is more work. It asks families to think beyond a single procedure or device.
But when a child's sleep problem is tied to airway anatomy, oral function, behavior, and breathing habits all at once, simple answers often don't hold. Coordinated care usually gets closer to durable improvement because it treats the child, not just the test result.
When to Seek a Pediatric Sleep Specialist
Referral shouldn't wait until a child is in crisis. In many cases, the right time is when the pattern is persistent, the symptoms don't fit neatly into routine care, or treatment attempts haven't explained the full picture.
There's also a practical reason to lower the threshold. In one survey, only 46% of pediatricians felt confident or very confident screening for sleep problems, and just 25.3% felt confident treating them, according to this survey data on pediatric sleep training and practice gaps. Clear referral pathways help children get evaluated before sleep disruption becomes a chronic family problem.
Referral triggers for parents
Consider specialist evaluation if any of these apply:
- Snoring plus daytime issues such as irritability, hyperactivity, poor focus, or fatigue
- Observed breathing pauses or gasping during sleep
- Mouth breathing that persists despite routine allergy or congestion treatment
- Teeth grinding with other sleep concerns like restless sleep or morning headaches
- Bedtime struggles or night waking that don't improve with consistent routines
- Night terrors, sleepwalking, or unusual sleep behaviors that are frequent, intense, or hard to interpret
Referral triggers for pediatricians, ENTs, dentists, and therapists
A specialist workup is especially useful when:
- Symptoms are mixed and it isn't clear whether the main problem is behavioral, neurologic, or airway-related
- Exam findings and symptoms don't match well, such as a child with significant daytime dysfunction but a limited office exam
- Initial treatment hasn't solved the problem, including persistent mouth breathing after common interventions
- Oral function seems relevant, including low tongue posture, restricted tongue mobility, narrow arches, or bruxism
- Objective testing may change management, particularly when surgery, PAP therapy, or multidisciplinary treatment is being considered
For clinicians and families who are trying to determine the right next step, connecting with a sleep disorder specialist near me can help move the case from suspicion to a clear plan.
A sensible threshold
If the child's sleep is affecting behavior, learning, breathing, or family functioning, that's enough reason to ask for expert input. You don't need to wait for a dramatic event or a textbook presentation.
Your Path to Restored Health and Sleep
Most pediatric sleep problems aren't simple, but they are often understandable once the right questions are asked. A child may need airway evaluation, behavior support, oral function treatment, or a combination of all three. The point is to identify the underlying driver and treat that driver directly.
That root-cause mindset changes the conversation. Instead of asking only whether a child snores or resists bedtime, the better question is why sleep is unstable in the first place. When care is thoughtful and coordinated, sleep can improve in a way that supports mood, learning, breathing, and development.
For parents, small daytime changes can also support the bigger treatment plan. Consistent routines, calm evenings, and lower screen exposure often help. If you need practical ideas for winding down without devices, this guide to find screen-free activities for children is a useful place to start.
If you're worried that your child's sleep isn't normal, trust that instinct. If you're a referring provider who sees the pattern but wants a more complete airway and function workup, early collaboration helps.
If you're ready for next steps, Pain and Sleep Therapy Center offers resources for both families and referring providers, including sleep-focused evaluations, airway and oral function assessment, and guidance on whether multidisciplinary care may be appropriate.



