
You're tired, but the pain won't let you drop into sleep. You shift your jaw, shoulder, neck, lower back, or hip, trying to find the one position that might work. Then the clock becomes part of the problem. The longer you stay awake, the more alert and frustrated you feel. By morning, you haven't just lost sleep. You've lost patience, focus, and some of your ability to cope.
That pattern is so common that many people start to believe their only option is to keep chasing pain relief and hope sleep follows. In practice, that often fails. With chronic pain and insomnia, the more useful question is not “Which one came first?” but “How do we stop them from feeding each other?”
The Nightly Struggle with Chronic Pain and Insomnia
At night, pain gets louder. Not always because the underlying condition suddenly changes, but because the usual daytime distractions fall away. Patients often describe the same sequence. They lie down already bracing for a bad night. They fall asleep late, wake often, or sleep lightly enough that every turn in bed feels like work.
What makes this so frustrating is that it doesn't feel like two separate problems. It feels like one trap.
A major review found that almost 90% of patients with chronic pain report insomnia symptoms, and another review found that in pain-management centres, more than 65% of patients describe themselves as poor sleepers, according to this clinical review on pain and insomnia. That matches what clinicians see every week. Poor sleep is not a side note in chronic pain care. It's part of the condition burden.
What patients often notice first
Some people can't fall asleep because they can't get comfortable. Others fall asleep but wake repeatedly, often with muscle tension, jaw clenching, headaches, or a racing mind. Many wake too early and never return to sleep.
A few patterns show up again and again:
- Bedtime dread because nighttime has become predictable and unpleasant
- Light, broken sleep that never feels restorative
- Pain amplification overnight when stillness leads to more awareness of symptoms
- Morning exhaustion even after spending enough hours in bed
Chronic pain and insomnia often behave like one clinical loop, not two unrelated diagnoses.
That's why basic advice like “just get more sleep” rarely helps. If pain is fragmenting sleep, and poor sleep is making the nervous system more reactive by the next day, the cycle keeps running. Breaking it usually requires treating sleep as more than an afterthought.
Understanding the Vicious Cycle of Pain and Poor Sleep
Pain disrupts sleep in obvious ways. It can make it harder to get comfortable, harder to stay asleep, and harder to return to sleep after waking. But the other half of the cycle matters just as much. Poor sleep changes how the brain and body process discomfort the next day.
One simple way to understand it is to picture a volume knob. Pain is the signal. Sleep helps regulate the system that turns the volume down. When sleep becomes shallow, fragmented, or inconsistent, that volume control stops working well. The result is not imaginary pain. It is pain that feels sharper, more intrusive, and harder to manage.
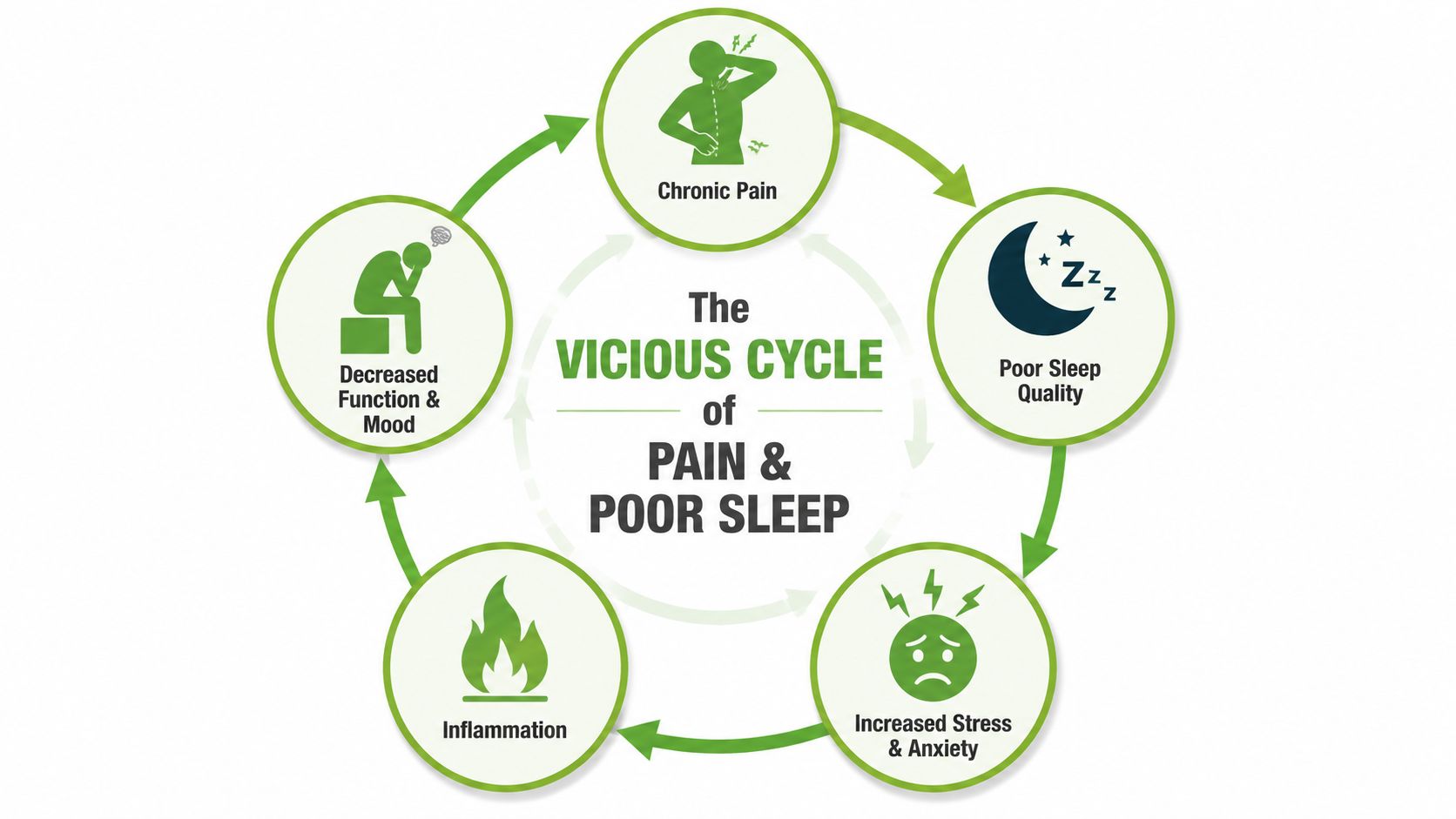
How the loop reinforces itself
The cycle usually includes several layers at once:
- Pain fragments sleep with longer time to fall asleep, more awakenings, and less efficient sleep
- Poor sleep raises pain sensitivity and reduces resilience the next day
- Stress and anxiety increase because another bad night starts to feel likely
- Mood and function drop so normal tasks feel heavier and recovery gets harder
This bidirectional relationship is well supported in the literature. A review on sleep and pain describes chronic pain as being associated with longer sleep-onset latency, more awakenings after sleep onset, shorter total sleep time, and poorer sleep efficiency, while insomnia is also a risk factor for developing or maintaining pain symptoms, as summarized in this review on chronic pain and sleep.
Why this matters clinically
When chronic pain and insomnia travel together, the issue isn't just comfort. A large population-based study found that people with chronic multisite pain plus insomnia had a 21% higher risk of all-cause mortality than those with neither condition, as noted in the evidence summarized by the earlier review on pain and insomnia.
That doesn't mean every poor sleeper should panic. It means this pattern deserves treatment.
Practical rule: If your pain is worse after a bad night, and your sleep is worse after a painful day, assume you're dealing with a cycle until proven otherwise.
A lot of treatment plans stall because they target only one side. If the plan focuses only on pain procedures, only on pain medication, or only on generic sleep hygiene, the loop often survives. Durable improvement usually comes when clinicians address pain and insomnia together, while recognizing that insomnia may need its own direct treatment path.
Recognizing the Clinical Signs and Symptoms
Many people say, “I know I'm not sleeping well.” That's true, but it's often too broad to be useful. Specialists listen for a more specific pattern, because chronic pain and insomnia show up in different ways at night and during the day.
Nighttime signs
Some symptoms point to sleep-onset insomnia. You get into bed tired, but pain, tension, or mental arousal keeps you awake. This is common in people who brace physically at night, clench the jaw, or become hyperaware of every uncomfortable sensation.
Other symptoms fit sleep-maintenance insomnia. You fall asleep, then wake over and over. Sometimes the trigger is obvious, such as facial pain, neck pain, headaches, or shifting position. Sometimes the first awakening comes from pain, and the later ones come from frustration and alertness.
A third pattern is non-restorative sleep. You may technically sleep for hours but wake feeling unrefreshed, stiff, foggy, and depleted.
Daytime signs
What happens the next day is part of the diagnosis. People often report:
- Fatigue that feels heavy, not just sleepy
- Brain fog with poor concentration or slower recall
- Lower pain tolerance for routine tasks
- Irritability or tearfulness after another bad night
- Reduced activity because everything feels harder than it should
If you wake feeling as if you “never really slept,” that's clinically meaningful, even if you were in bed all night.
Clues that the problem is bigger than sleep hygiene
Many patients have already tried the usual advice. They've darkened the room, cut back caffeine, used white noise, bought a pillow, or started a bedtime tea. Those steps can help at the margins, but they don't usually fix a self-reinforcing pain-sleep cycle on their own.
The pattern becomes more concerning when you notice that sleep trouble is tied to pain flares, mood changes, jaw tension, headaches, or a growing fear of bedtime itself. At that point, the issue is less about “bad habits” and more about a conditioned cycle involving the nervous system, behavior, and the body's pain response.
How Specialists Diagnose the Root Cause
A good evaluation starts by refusing to oversimplify the problem. If a patient says, “My pain keeps me awake,” that may be true. It also may be incomplete. In chronic pain populations, insomnia is common enough that a screening-first approach is justified. One study found that 72.8% of patients with chronic non-cancer pain met diagnostic criteria for insomnia, according to this study on insomnia in chronic pain patients.
That's why specialists don't stop at a quick sleep question. They look for the full pattern.
What a thorough evaluation usually includes
A careful assessment often covers:
- Pain timing and type such as whether symptoms peak at bedtime, during the night, or on waking
- Sleep pattern details including time to fall asleep, number of awakenings, early morning waking, and perceived sleep quality
- Behavior around sleep such as spending extra time in bed, irregular schedules, or trying too hard to force sleep
- Mood and stress load because anxiety and depression commonly intensify the cycle
- Breathing and airway clues including snoring, dry mouth, witnessed pauses, or waking with headaches
A structured sleep quality assessment can help organize these details before a formal visit and make the conversation more productive.
When testing matters
Not every patient needs a sleep study, but some do. If the history suggests sleep-disordered breathing, repeated choking or gasping, heavy snoring, or unexplained daytime sleepiness, clinicians may recommend further evaluation. The goal is not to pile on tests. It's to avoid missing a second problem that can sabotage treatment.
A pain diary and sleep diary are often more useful than patients expect. When tracked together, they can reveal patterns that memory alone misses.
| What to track | Why it helps |
|---|---|
| Bedtime and wake time | Shows schedule variability |
| Night awakenings | Clarifies sleep-maintenance issues |
| Pain intensity and location | Identifies symptom timing |
| Medications and timing | Spots treatment-related patterns |
| Caffeine, alcohol, naps, activity | Reveals contributors and confounders |
The most useful diagnosis is rarely “you have pain” or “you have insomnia.” It's identifying what keeps the cycle active in your specific case.
That distinction matters. Jaw pain, TMJ-related muscle tension, headaches, airway issues, anxious arousal, and conditioned wakefulness in bed can all look similar from a distance. Treatment gets better when diagnosis gets more precise.
Evidence-Based Treatments That Break the Cycle
If you only treat pain, sleep may stay broken. If you only chase sleep with sedating shortcuts, the next day's pain and dysfunction may still be there. The most effective plans usually work on both sides of the loop, while recognizing that insomnia often needs direct treatment of its own.
A recent review highlights that the pain-sleep relationship is bidirectional and that insomnia can independently worsen next-day pain and disability. That supports treating insomnia as its own target, including with CBT-I, rather than assuming sleep will normalize once pain is better, as described in this review on insomnia as a distinct treatment target.
Why CBT-I matters in chronic pain
Cognitive Behavioral Therapy for Insomnia, or CBT-I, is not just a list of bedtime rules. Done well, it helps patients change the thoughts, behaviors, and conditioned patterns that keep insomnia going.
That matters in pain care because many people have developed a difficult relationship with bedtime itself. Bed becomes a place for bracing, clock-watching, worry, jaw clenching, symptom monitoring, and frustration. CBT-I works to reverse that pattern carefully and systematically.
If you want a plain-language overview of the method, this CBT guide for Vancouver residents gives a helpful introduction to how cognitive and behavioral strategies are used in practice.
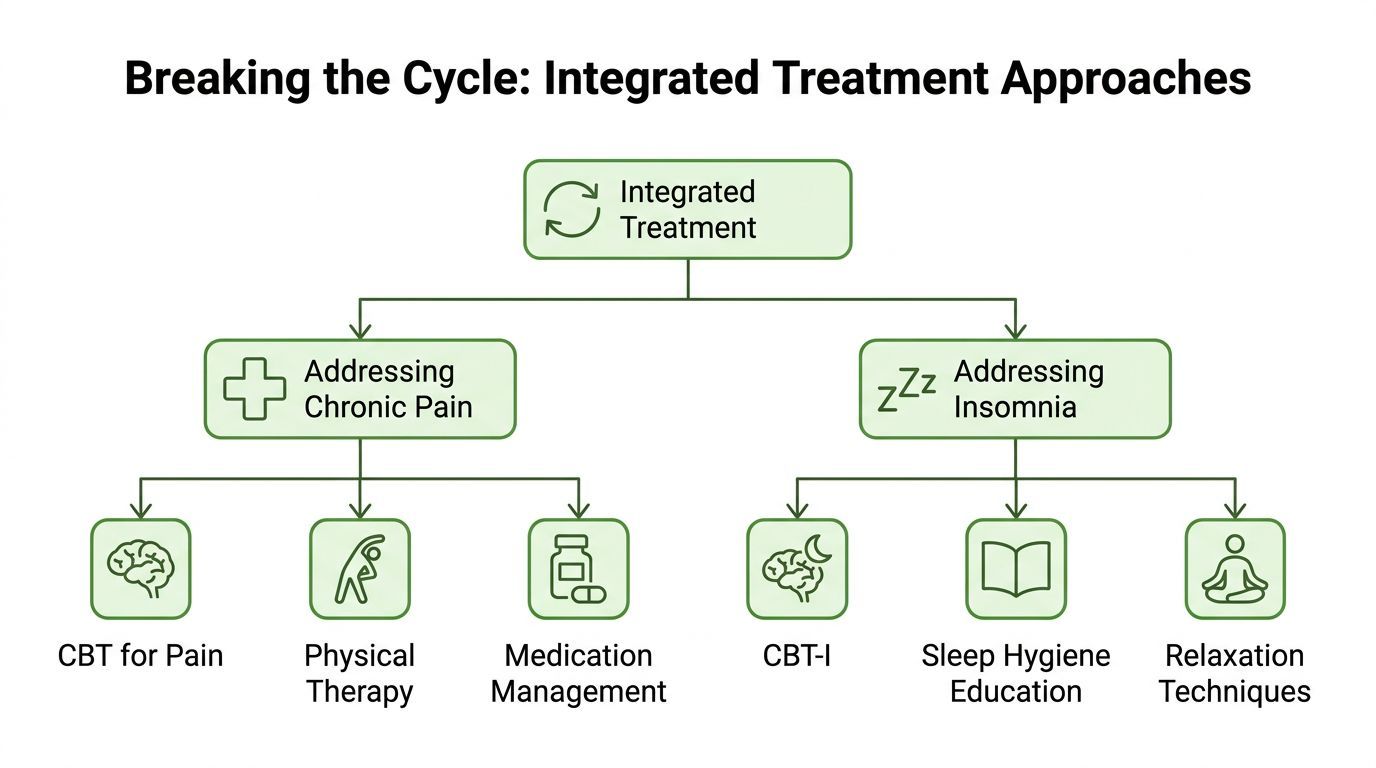
What integrated treatment can look like
An effective plan often includes more than one lane at once:
- Direct insomnia treatment with CBT-I or a modified version when pain limits mobility or tolerance for standard protocols
- Pain-focused rehabilitation such as physical therapy, targeted exercise progression, and behavioral pain coping strategies
- Targeted medical care for contributors such as TMJ dysfunction, headaches, facial pain, or sleep-disordered breathing
- Medication review to assess whether current treatment is helping, neutral, or disrupting sleep patterns
For patients dealing with overlapping symptoms, a multidisciplinary approach to pain management is often more realistic than expecting a single intervention to fix everything.
The next resource may help you visualize how integrated care works in practice.
What usually doesn't work well enough
Some common approaches help temporarily but don't solve the root problem:
- Waiting for pain to disappear first before addressing sleep
- Relying on generic sleep hygiene alone when insomnia has become conditioned and persistent
- Using bedtime as recovery time for hours of wakeful rest, which can strengthen the brain's association between bed and being awake
- Overdoing activity after a better night, then triggering a flare that ruins the next one
Sleep improvement is often not the reward you get after pain is fixed. It's one of the tools that helps pain become more manageable.
That shift in strategy is often the turning point.
Self-Management Strategies for Daily Relief
Home strategies won't replace skilled care when the cycle is established, but they can lower friction and help treatment work better. The key is choosing tools that respect pain, rather than pretending pain isn't there.

Build a calmer evening on purpose
The hour before bed shouldn't be a struggle to “knock yourself out.” It should be a transition. For many pain patients, that means lowering stimulation before they ever lie down.
A simple wind-down routine might include gentle stretching, heat or cold if prescribed, light breathing work, dimmer lighting, and less screen exposure. If scent helps you settle, a practical overview like Aroma Warehouse's sleep oil guide can be a reasonable starting point for non-medication comfort measures.
Protect tomorrow from tonight
One of the biggest traps in chronic pain care is the boom-and-bust pattern. You finally sleep a bit better, feel more human, and then do too much. By evening, pain is back up and sleep falls apart again.
Try these daily rules instead:
- Pace the good days so improved energy doesn't turn into overexertion
- Keep wake time steady even after a rough night, unless your clinician advises otherwise
- Track patterns briefly in a notebook or app, but don't turn monitoring into a second job
- Use movement strategically with short bouts of mobility work rather than long all-or-nothing efforts
Keep self-care specific
Generic advice is often too broad to help. More specific habits tend to work better:
| Self-management tool | Best use |
|---|---|
| Gentle evening mobility | Reduces stiffness without revving you up |
| Breathwork | Helps reduce arousal and jaw or chest tension |
| Heat, ice, or topical support | Offers symptom-specific comfort when recommended |
| Brief journaling | Gets worries out of your head before bed |
| Consistent morning light exposure | Supports a stronger sleep-wake rhythm |
For readers looking for more conservative strategies, this guide on how to improve sleep quality naturally offers ideas that can fit alongside professional treatment.
Self-management works best when it supports a larger plan. It struggles when it becomes a substitute for diagnosis.
If you've been trying hard and still feel stuck, that doesn't mean you're doing it wrong. It often means the cycle is stronger than self-help alone can handle.
Your Path Forward at the Pain and Sleep Therapy Center
The most useful takeaway is simple. Chronic pain and insomnia rarely improve for long when they're treated as separate complaints. Pain can disturb sleep. Sleep loss can increase pain, disability, irritability, and reduced function the next day. Once that loop is established, both sides need attention.
That's especially true when symptoms overlap with jaw tension, TMJ dysfunction, facial pain, headaches, snoring, or suspected airway problems. In those cases, a narrow plan can miss the root driver. A broader clinical view often leads to better decisions.
A center that combines expertise in pain, breathing, jaw function, and sleep can sort out whether the main issue is insomnia, pain-driven sleep disruption, sleep-disordered breathing, TMJ-related strain, or a combination of several. That kind of interdisciplinary model matters because patients rarely arrive with a neat, single-cause problem.
When it's time to get help
Consider a specialist evaluation if any of these sound familiar:
- You've tried basic sleep advice and still wake exhausted
- Pain, jaw tension, or headaches reliably worsen your nights
- Snoring, dry mouth, or breathing concerns are part of the picture
- You're spending more time in bed but sleeping worse
- Your mood, concentration, or daily function are slipping
The goal isn't to chase another temporary fix. It's to identify what's driving your cycle and build a plan that addresses the cause, not just the symptoms.
If you're ready for a more precise approach, Pain and Sleep Therapy Center offers evaluation and treatment for TMJ-related pain, facial tension, sleep-disordered breathing, and other root causes that can keep chronic pain and insomnia locked together. A focused assessment can help you figure out what's driving your nights, and what to do next.



