
Those who begin researching full arch dental implants are often already tired.
They're tired of planning meals around what dentures can handle. Tired of teeth that are loose, broken, infected, or failing one at a time. Tired of smiling with their lips closed in photos, or speaking carefully because they don't trust what will happen when they laugh, cough, or bite into something firmer than soft bread.
That fatigue matters. Full arch treatment isn't just about replacing teeth. It's about restoring a stable bite, dependable function, and the kind of confidence that disappears slowly when oral health has been a daily problem for too long.
A Lasting Solution for a Lost Smile
A patient in this situation often isn't choosing between “good” and “better.” They're choosing between continued compromise and a meaningful reset.
Sometimes the problem is an upper denture that moves at the wrong moment. Sometimes it's a lower denture that never really felt secure. In other cases, the patient still has teeth, but they're heavily restored, repeatedly infected, or so worn down that each new repair feels temporary. The common thread is loss of trust. Eating becomes cautious. Social situations feel calculated. Oral health starts controlling the day.
What changes with a fixed foundation
Full arch dental implants shift the conversation from replacing individual teeth to rebuilding the entire support system. Instead of relying on gum pressure or adhesive, the restoration is anchored to implants placed in the jaw. That changes how the teeth feel, how they function, and how the patient experiences daily life.
For the right candidate, the difference is practical:
- Chewing becomes more predictable because the prosthesis doesn't slide the way a conventional denture can.
- Speech often feels more natural once the tongue and lips adapt to a stable restoration.
- Self-conscious habits ease up because patients aren't constantly checking whether their teeth are moving.
- Repeated patchwork dentistry can stop when the treatment plan addresses the full problem rather than one failing tooth at a time.
Full arch treatment works best when the goal isn't simply to “put teeth back,” but to rebuild a bite that a patient can rely on every day.
Why this option feels different
What patients usually notice first is stability. What clinicians value most is control. A fixed implant-supported arch lets the team design function, tooth position, smile support, and hygiene access more intentionally than a removable appliance usually allows.
That doesn't make it simple, effortless, or right for everyone. It does make it one of the most important advances in restorative dentistry for people missing an entire upper or lower arch, or those approaching that point.
Understanding Full Arch Dental Implants
A full arch prosthesis works less like paving a path with separate stones and more like building a bridge on engineered supports. The visible teeth are the bridge. The implants are the piers that carry the load into the bone.
Historically, complete-arch fixed prostheses often used about 5 to 10 implants, but modern concepts such as All-on-4 can support an entire arch with four implants, often by angling the posterior implants to bypass anatomic limits, shorten cantilevers, and help avoid grafting in selected cases, as described in this clinical review of complete-arch fixed prostheses.

Why four to six implants can support a full arch
Patients often ask why they don't need one implant for every missing tooth. The answer is biomechanics.
A full arch prosthesis is splinted together. That means the restoration shares forces across the whole framework rather than asking each implant to act alone. When implants are placed in strong positions and connected by a rigid prosthesis, they work as a system.
Most full arch designs are built around 4 to 6 implants per arch. The exact number depends on anatomy, bite forces, restorative goals, and how much margin for safety the case requires.
Why angled posterior implants matter
The back implants are where modern planning changed the field. In many patients, the posterior jaw presents limitations such as the maxillary sinus in the upper arch or reduced bone volume in the back of the jaws. Tilting posterior implants can let the surgeon engage available bone more effectively.
That has real consequences for the patient:
- Less need for grafting in selected cases because the implants use existing bone more efficiently.
- Better support for the prosthesis by extending the implant spread farther back.
- Shorter cantilevers so the bridge doesn't project unsupported as far beyond the terminal implants.
- A simpler surgical process in cases where traditional posterior placement would have required additional procedures first.
Practical rule: The best full arch design uses the bone you have wisely, rather than assuming more surgery is always the answer.
What the implants actually do
The implants don't replace teeth one-for-one. They create anchor points. Onto those anchors, the restorative team attaches a fixed bridge that replaces the visible teeth and, when needed, some missing gum and tissue volume as well.
That's why full arch dentistry is more than implant placement. It's prosthetic engineering, surgical planning, and bite design working together. When those parts line up, the treatment feels efficient. When they don't, patients often end up with a smile that looks acceptable in photos but is harder to clean, harder to chew with, or harder to maintain long term.
Comparing Your Full Arch Treatment Options
Most patients are choosing between two broad paths. One is a fixed hybrid bridge, commonly associated with All-on-4 or All-on-6 treatment. The other is a removable implant-supported overdenture, which snaps onto implants but comes out for cleaning.
Both use implants. They are not the same experience.
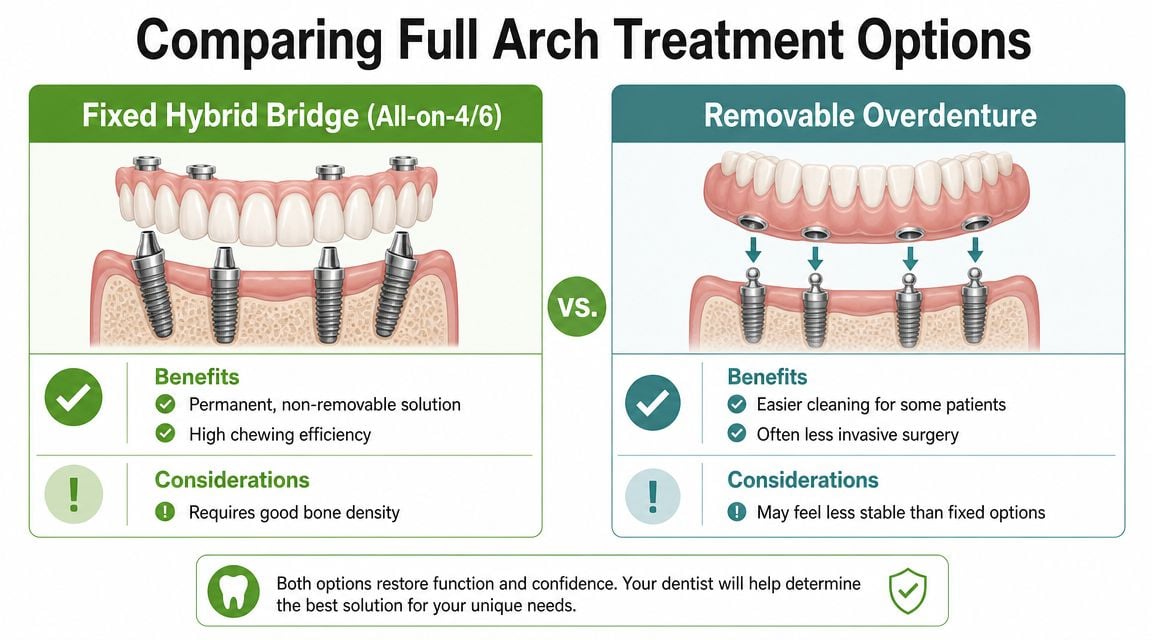
Fixed and removable are different lifestyles
A fixed hybrid bridge is designed to stay in place. The patient brushes and cleans around it while it remains attached, and the dental team removes it at maintenance visits when needed. This option usually appeals to people who want the most tooth-like experience and don't want to take their teeth out.
A removable overdenture still gains retention from implants, which is a major step up from a loose conventional denture. But it remains a removable appliance. For some patients, especially those who want easier direct cleaning or a less involved surgical plan, that's a reasonable trade-off.
For a plain-language overview of how practices explain fixed full-arch care to patients, Dr. Schneider's implant services are a useful reference.
Full Arch Options at a Glance
| Feature | Fixed Hybrid Bridge (All-on-4/6) | Removable Implant Overdenture |
|---|---|---|
| Feel in daily life | Closest to fixed teeth | More secure than a traditional denture, but still removable |
| How it stays in place | Attached to implants by the dental team | Snaps onto implants and is removed by the patient |
| Chewing experience | Usually stronger and more stable | Improved over a conventional denture, but less fixed in feel |
| Cleaning style | Clean under and around the bridge in the mouth | Remove daily for direct cleaning |
| Surgical demands | Often more prosthetically exacting | May be a simpler path for selected patients |
| Best fit for | Patients who prioritize a fixed solution | Patients who value removability or easier direct access for hygiene |
| Cost discussion | Typically a larger initial investment | Often a more conservative entry point |
Later in the decision process, some patients with severe upper jaw bone loss ask whether advanced alternatives are needed. In those cases, it can help to understand options like zygomatic bone implants, which are considered in more anatomically challenging situations.
Here's a visual walkthrough of the fixed approach many patients ask about:
What long-term durability tells us
Long-term outcome data matter most when a patient is deciding whether a fixed full-arch option is established care or still a niche concept. One review reports 10-year prosthetic survival of 98.8% in the lower jaw and 95% to 97% in the upper jaw for All-on-4, with individual implant survival at 94.8% after 10 years. The same source notes that All-on-6 can reach 98% to 99% success rates, and cites a 2022 study reporting 99.0% implant survival for All-on-6 versus 89.7% for All-on-4 in the same population, according to this summary of full-arch implant outcomes.
Those figures don't mean more implants are always better. They do support a more careful point. Cases with greater force demands, more complex anatomy, or a desire for added restorative flexibility may justify a different design than the minimum implant count.
A full arch plan should fit the patient's anatomy, bite, and maintenance capacity. It shouldn't be reduced to a slogan.
The Advanced Diagnostic and Planning Workflow
A patient may arrive focused on one question: “Can I leave with fixed teeth?” My first concern is different. I need to know whether the anatomy, bite, smile line, and long-term maintenance demands all support a result that is safe to deliver and realistic to keep healthy.

The records that matter
A strong full arch workup usually includes CBCT, intraoral scanning, facial analysis, and a diagnostic wax-up or mock-up. Each record answers a different question, and the value is practical, not cosmetic.
- CBCT shows the three-dimensional anatomy, including available bone, sinus position, nerve location, implant angulation limits, and the restorative space that may or may not exist.
- Intraoral scans capture teeth and soft tissue surfaces with enough detail to plan fit, contour, and prosthetic transitions.
- Facial analysis connects the teeth to the face, which affects lip support, smile display, phonetics, and whether the final prosthesis will look natural in motion, not just in a still photo.
- A wax-up or mock-up sets the restorative end point before surgery, so implant placement supports the planned teeth instead of forcing compromises later.
That sequence is the basis of prosthetically driven planning. The implants are positioned to support the restoration the patient will wear every day, clean every day, and function on for years. A detailed clinical review of that approach appears in this review of precision planning in full-arch implant rehabilitation.
Why digital planning changes the surgical risk profile
Technology matters because it changes decisions before the first incision. CBCT can reveal that an implant trajectory is too close to the sinus or inferior alveolar nerve. A facial scan can show that the planned tooth position needs more lip support than the existing ridge allows. A diagnostic setup can expose limited restorative space that would otherwise create bulky teeth, poor speech, or hygiene trouble after surgery.
Guided planning can improve precision, but only when the records are accurate and the plan respects biology. A surgical guide does not fix poor bone quality, unstable bites, parafunctional habits, or unrealistic esthetic goals. It helps the team place implants where they were intended to go.
Patients who are anxious about the planning appointment or the procedure itself often benefit from reviewing their oral surgery anesthesia options early, because comfort planning affects the whole treatment experience, not just the surgical day.
A good patient education resource can also help clarify how a fixed implant restoration differs from a removable option in day-to-day life. St. Pete Family & Cosmetic Dentistry offers that kind of overview.
In full arch treatment, the best plan starts with the final teeth, the bite, and the hygiene design. Implant placement follows those requirements.
Small design decisions shape long-term maintenance
Patients rarely see the decisions that protect a case over time. Clinicians do. Abutment height, tissue contour, prosthetic access channels, smile line, and cleansability all influence whether the restoration remains healthy and serviceable.
One example is abutment selection. The planning literature has associated very short abutments with greater marginal bone loss in some situations. That does not create a universal rule, but it does show why full arch treatment is restorative dentistry, surgery, and maintenance planning at the same time.
This is also where newer biologic tools fit the larger picture. Digital diagnostics help the surgeon place implants more safely and design the prosthesis more intelligently. Healing tools such as PRF, discussed in the treatment timeline, matter because better tissue response supports the plan you worked so carefully to build.
Your Full Arch Treatment Timeline Explained
The treatment day gets the most attention, but patients usually do better when they understand the full sequence. Full arch rehabilitation is a process with distinct phases. Each phase has a different goal.
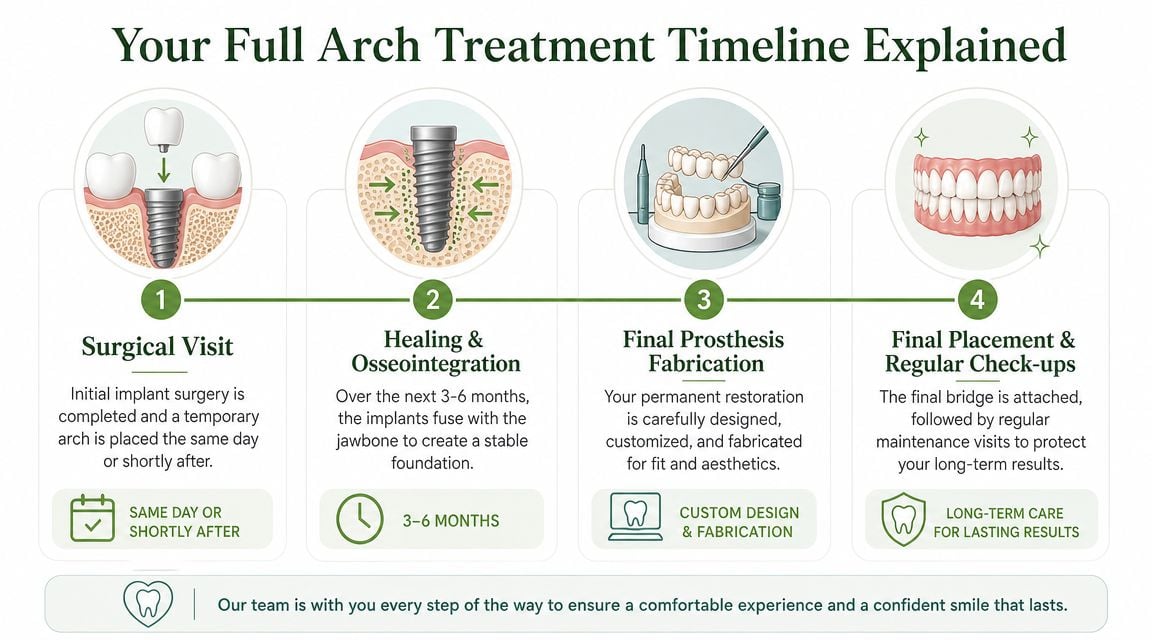
Phase one includes surgery and temporary teeth
On the surgical visit, the team may remove failing teeth, prepare the sites, place the implants, and attach a temporary full-arch prosthesis when primary stability allows. This is the part many patients know as “teeth in a day.”
The phrase is useful, but it can also mislead. What patients receive that day is typically a provisional prosthesis, not the final restoration. It's meant to look good, function acceptably, and protect the implants during healing.
For patients who feel anxious about the surgical experience itself, discussions around sedation and comfort matter just as much as the restorative plan. A page like this overview of oral surgery anesthesia can help patients understand those options before the procedure.
PRF and healing support
Some practices also use Platelet-Rich Fibrin, or PRF, as part of the surgical protocol. PRF is prepared from the patient's own blood and used as a biologic aid at surgical sites. In practical terms, it functions like a natural healing membrane or “bandage” that can support soft-tissue healing and help the early recovery period feel more manageable.
Patients don't need PRF to understand one key point. Healing quality is shaped by surgical technique, tissue handling, prosthetic fit, and the patient's health habits in the days that follow.
A straightforward patient guide to sequencing and expectations can also be found through Dental Professionals of Fair Lawn, which outlines the broader implant timeline in accessible terms.
Healing comes before the final bridge
After surgery, the implants need time to integrate with bone. During this healing phase, patients usually follow a modified diet and specific hygiene instructions while the tissues mature and the implants stabilize.
Then the final restorative phase begins. The temporary prosthesis has already taught the team a lot: where speech needs adjustment, whether lip support is ideal, how the bite feels, and what contours are easiest to clean. Those lessons are carried into the definitive prosthesis, often fabricated in more durable materials such as zirconia or other reinforced designs depending on the case.
The provisional phase is not a placeholder to rush through. It is one of the most informative parts of full arch treatment.
The final delivery is not the finish line
When the final bridge is delivered, patients usually feel the emotional payoff of the process. The teeth look more refined. The bite feels more settled. Function improves.
However, the true long-term work begins there. The patient now has an advanced prosthesis that needs regular review, occasional adjustment, and disciplined home care if it's going to perform the way it was designed to.
Benefits, Risks, and Candidacy Factors
The best reason to consider full arch dental implants is simple. They can restore a level of confidence and function that removable dentures often can't match.
A stable implant-supported arch can let patients eat with less caution, speak with more confidence, and stop relying on adhesives or the constant mental rehearsal that comes with loose teeth. For someone who has spent years managing dental problems meal by meal, that improvement can feel enormous.
The benefits patients usually care about most
The functional gains are often more meaningful than the cosmetic ones, even though both matter.
- Food choice opens up because the teeth are anchored rather than resting loosely on the gums.
- Speech often becomes less guarded once the prosthesis is stable and the contours are refined.
- Social confidence improves because smiling and laughing don't carry the same fear of movement or embarrassment.
- Treatment can consolidate a failing situation when keeping compromised teeth would mean repeated repairs with uncertain prognosis.
Patients also like the psychological simplicity. They want to stop living in a cycle of temporary fixes.
The risks deserve a direct conversation
None of that means candidacy is automatic. Full arch implant treatment is surgery, and surgery always requires judgment.
Potential problems include failure of an implant to integrate, infection, mechanical complications, prosthetic fracture or wear, bite problems, hygiene difficulty, and dissatisfaction with esthetics or speech if the planning is poor. Some risks are procedural. Others show up only over time because the prosthesis was difficult to clean or because the patient couldn't maintain the level of home care required.
A broad implant follow-up study of 10,871 implants reported cumulative implant survival of 98.9% at 3 years, 98.5% at 5 years, 96.8% at 10 years, and 94.0% at 15 years, while patient-level survival declined from 97.4% at 3 years to 86% at 15 years. The same study found that smoking and diabetes mellitus were positively correlated with implant failure, and that patients with multiple implants had a 10-year survival rate of 90.2% compared with 98.2% for single-implant patients, according to this large clinical follow-up study on implant survival.
Who tends to be a better candidate
Good candidates are not defined by enthusiasm alone. They're defined by a combination of anatomy, medical history, bite forces, and maintenance capacity.
Key factors include:
- Systemic health. Smoking and uncontrolled diabetes can shift risk in the wrong direction.
- Bone and soft tissue condition. Adequate anatomy improves restorative options, though advanced designs may expand what's possible.
- Expectation level. Patients need to understand the difference between a provisional bridge and a final one, and between a fixed bridge and a natural dentition.
- Commitment to maintenance. This treatment rewards patients who will clean thoroughly and return for follow-up.
For patients weighing treatment plans more broadly, including the financial side of implant care, this overview of the average cost of dental implants can help frame the conversation.
Ensuring Decades of Success with Proper Aftercare
One of the most damaging myths in implant dentistry is that implants don't need much maintenance because they “can't get cavities.” That's the wrong benchmark.
Implants can fail for biologic and mechanical reasons, and many of those problems develop slowly. A fixed full-arch bridge may feel solid for years while plaque accumulates beneath it, inflammation progresses, or access for cleaning becomes more difficult because the patient never learned the right technique.
Daily care has to be realistic
A patient with full arch dental implants needs a cleaning routine built for a prosthesis, not for natural teeth alone. That usually includes brushing, cleaning under the bridge, and using tools such as a water flosser or appropriately sized proxy brushes when recommended.
The goal isn't perfection. The goal is consistency.
- Clean where the bridge meets the tissue because plaque tends to accumulate in the protected spaces patients can't see easily.
- Use the tools the prosthesis requires rather than assuming ordinary brushing is enough.
- Report soreness, bleeding, or odor early because these are often the first signs that hygiene access or inflammation needs attention.
- Keep maintenance visits so the clinical team can remove deposits, assess tissue health, and evaluate the prosthesis itself.
A beautiful bridge that a patient can't clean is not a long-term success. It's a delayed problem.
Peri-implant disease is real
A 2024 study reported peri-implant mucositis in 36.4% and peri-implantitis in 14.9% of implants, with higher risk linked to poor plaque control and smoking, as summarized in this clinical discussion of maintenance challenges in full-arch implantology.
Those terms matter. Peri-implant mucositis is inflammation in the soft tissue around an implant. Peri-implantitis goes further and involves destructive disease around the supporting structures. In everyday language, this is the implant equivalent of saying, “inflammation can become deeper damage if no one intervenes.”
Success is a partnership
The surgical result matters. The prosthesis design matters. But long-term performance depends on the relationship between patient habits and professional follow-up.
Some patients are excellent surgical candidates and poor maintenance candidates. That distinction should change the treatment recommendation. If dexterity is limited, if dry mouth is significant, if plaque control has historically been poor, or if regular recall visits are unlikely, the smartest plan may not be the most aggressive one.
That honesty protects the patient. It also protects the implants.
If you're dealing with jaw pain, facial tension, sleep-disordered breathing, or complex bite concerns alongside missing or failing teeth, Pain and Sleep Therapy Center offers a more root-cause view of care. Their Charlotte team focuses on technology-driven diagnostics, airway and TMJ evaluation, and regenerative therapies such as PRF in the broader context of function, comfort, and long-term health.



