
If you're reading this the night before surgery, you're probably thinking less about molars and more about very practical questions. Will the procedure hurt? Will you be groggy? What should you take afterward, and what can you skip?
That anxiety is normal. Wisdom tooth extraction is common, but it still feels personal when it's your mouth, your sleep, your schedule, and your pain tolerance on the line. The best recoveries usually don't happen by accident. They happen when the medication plan is simple, intentional, and matched to the person.
Your Personalized Plan for a Smooth Recovery
A good plan starts before the first numbing shot. One patient may need only local anesthesia and a straightforward non-opioid pain routine. Another may need deeper sedation because of severe dental anxiety, complex impaction, or a history of difficult dental treatment. Someone with reflux, kidney concerns, pregnancy, anticoagulant use, or medication sensitivities may need a modified approach from the start.
That matters because wisdom tooth extraction isn't rare. It's performed about 3.5 million times a year in the United States, and claims-based research found that about 50% of people have had at least one third-molar extraction by age 25 in a large dataset on dental extractions and third molars (Frontiers in Dental Medicine). When a procedure is this common, small medication decisions add up for a lot of people.
For patients who like to prepare, I often suggest reading a practical overview such as Cali Family Dental's recovery guide so the basics feel familiar before surgery day. Planning your food in advance also helps more than commonly expected, especially if chewing will be limited for a few days. A simple wisdom teeth recovery food guide can make the first couple of days much easier.
A calm recovery usually comes from fewer surprises. Know what you'll take, when you'll take it, what you should avoid, and when you should call.
Think of medication for wisdom tooth extraction as part of a full recovery system, not a bag of prescriptions. There are medications used during the procedure to keep you comfortable. There are medications used after the procedure to control inflammation and pain. And there are situations where the safest choice is using less medication, not more.
The modern approach is more selective than older routines. Most healthy patients don't need opioid-heavy pain plans. Many don't need routine antibiotics. What they do need is a strategy that controls pain, protects healing, and avoids unnecessary risk.
Staying Comfortable During the Procedure
Most of the fear around oral surgery comes from not knowing what you'll feel. The first thing to understand is that local anesthesia does the core work. It acts like a roadblock for pain signals. You stay conscious, but the nerves in the area are numbed so you shouldn't feel sharp pain.
Local anesthesia first
Before the deeper work starts, the surgeon typically places a topical numbing gel on the gum and then gives the local anesthetic injection. After that, the area becomes heavy, thick, and numb. Patients often notice pressure, movement, and vibration, but not cutting pain.
That distinction matters. Pressure can feel strange if you aren't expecting it, but it doesn't mean the anesthetic isn't working.
Practical rule: If you feel pain during the procedure, say so right away. Your surgeon can usually add more local anesthetic or adjust the plan.
Sedation works like a volume dial
Sedation isn't one fixed thing. It's more like a comfort dial that can be turned up or down depending on your anxiety level, medical history, and the complexity of the extraction.
- Nitrous oxide often works well for mild anxiety. You breathe it through a mask. Many patients feel calmer, lighter, or less focused on the procedure, and recovery is usually quick.
- Oral sedation is stronger but less precise in timing and effect. You take a prescribed pill before the appointment, and it can make you drowsy and less aware of the details.
- IV sedation is commonly chosen for more difficult extractions or for patients who want minimal memory of the procedure. You still receive local anesthesia, but the IV medication makes the experience feel much more distant.
A helpful comparison of these options appears in this overview of oral surgery anesthesia, especially for patients deciding how much support they want beyond numbing alone.
What recovery from sedation feels like
The sedation choice affects the rest of your day more than the extraction itself. With nitrous oxide, many people feel fairly normal soon after. With oral sedation or IV sedation, you can expect lingering grogginess, slower reaction time, and a definite need for an adult escort.
That's one reason I encourage patients to plan conservatively. Clear your schedule. Have gauze, ice packs, fluids, and soft foods ready. Comfort starts with the medications used in the chair, but it also depends on what happens in the first few hours after you get home.
The Modern Approach to Managing Post-Op Pain
For most patients, the best medication for wisdom tooth extraction after surgery is not an opioid. The strongest current direction is a non-opioid strategy built around ibuprofen plus acetaminophen, because it treats pain without bringing the sedation, nausea, constipation, and dependence concerns that often come with narcotics.
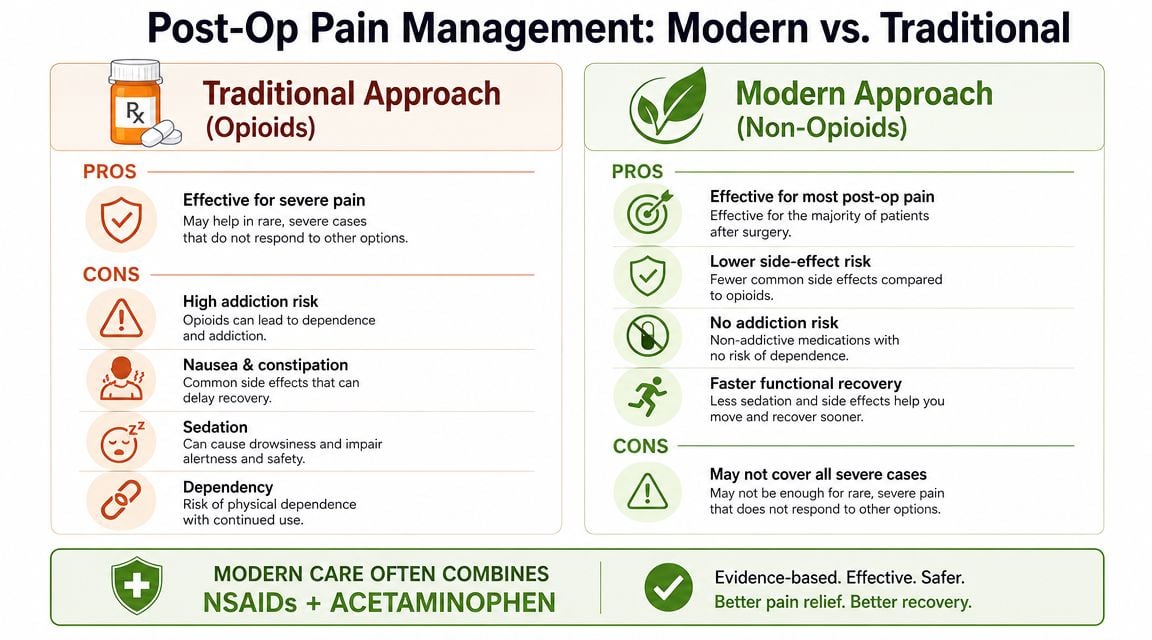
A widely reported 2025 trial found that ibuprofen plus acetaminophen provided better pain relief than hydrocodone plus acetaminophen for the first two days after surgery, along with better sleep and daily function, according to a summary of the trial findings from Powers Health. That's an important shift. The older assumption was that stronger prescription medication must work better. In many wisdom tooth cases, it doesn't.
Why the non-opioid plan often works better
Wisdom tooth pain is driven heavily by inflammation and tissue irritation. Ibuprofen addresses the inflammatory piece. Acetaminophen works differently and can complement it. Together, they often cover the pain pattern more effectively than an opioid combination that mainly blunts sensation while adding side effects.
Here is the practical reasoning many patients find helpful:
| Approach | What it tends to do well | Main limitations |
|---|---|---|
| Ibuprofen plus acetaminophen | Targets common post-op pain patterns, often with clearer thinking and less nausea | Not right for every patient, especially if NSAIDs or acetaminophen aren't safe for them |
| Opioid-containing medication | May help in select cases of severe breakthrough pain | Can cause sedation, constipation, nausea, and misuse risk |
Later in the recovery process, if you're comparing options for pain relief after tooth extraction, it helps to separate "stronger sounding" from "more effective for this type of pain." Those aren't always the same thing.
A simple schedule beats chasing pain
Many problems start when patients wait until the pain is severe. It's usually easier to stay ahead of inflammation than to calm it down once it surges. The exact schedule should come from your surgeon, but the principle is consistent: take the recommended non-opioid medication on time in the first phase of recovery if it's medically appropriate for you.
Use the smallest effective medication plan that keeps you functional, hydrated, and able to rest.
This is also where personalization matters. Some patients should avoid NSAIDs because of ulcers, kidney disease, bleeding risk, pregnancy concerns, or anticoagulants. Some need to limit or avoid acetaminophen because of liver disease or other factors. In those cases, the right plan may involve acetaminophen alone, a modified regimen, or a different strategy entirely. A generic internet checklist isn't enough.
The video below gives a useful patient-friendly overview of safer post-op pain planning.
Where opioids still fit
Opioids haven't disappeared from oral surgery, but their role should be narrow. I think of them as rescue medication, not routine prevention. They may be reasonable for brief use if pain is unusually intense, if surgery was especially difficult, or if standard non-opioid options aren't appropriate.
That caution isn't theoretical. A major U.S. study published in JAMA found that among opioid-naive patients who filled a perioperative opioid prescription after wisdom tooth extraction, persistent opioid use occurred at an adjusted rate of 13 per 1,000 patients, compared with 5 per 1,000 among those who did not fill such a prescription (JAMA). The same evidence was summarized as a more than two-fold increase in the rate of persistent opioid use in the reporting noted earlier.
For adolescents and young adults, that's enough reason to treat opioids with real respect. If they are prescribed, use them only as directed, for the shortest necessary period, and stop them as soon as the non-opioid plan is enough.
The Question of Antibiotics After Surgery
Many patients assume antibiotics are a standard part of wisdom tooth extraction. They aren't, or at least they shouldn't be.

A Cochrane review found that antibiotics after wisdom tooth surgery can reduce infection and dry socket, but the evidence was low certainty, and it does not support routine preventive use for every patient, especially given the downsides of side effects and antibiotic resistance (Cochrane review on third molar surgery antibiotics).
When antibiotics may make sense
There are situations where antibiotics are reasonable and sometimes important. These often include:
- Existing infection before surgery. If the tooth or surrounding tissue is already infected, the situation is different from a clean, routine extraction.
- Higher-risk surgery involving significant tissue manipulation, deeper impaction, or a more complicated healing environment.
- Medical vulnerability in patients whose healing or immune response may be affected by other health conditions.
- Clinical signs that infection is developing after the procedure, rather than using antibiotics "just in case" from the start.
Why selective use is safer care
Antibiotics aren't painkillers, and they don't speed healing just because they're prescribed. If there isn't a clear reason to use them, they can add stomach upset, rashes, yeast-related problems, medication interactions, and false reassurance. They also contribute to a larger public health problem when used casually.
Antibiotics should solve a defined problem. They shouldn't be handed out to make a routine procedure feel more serious or more complete.
Patients sometimes worry that "no antibiotic" means corners were cut. In many healthy cases, the opposite is true. It means the surgeon is matching treatment to the actual risk instead of following an outdated routine.
Medication Safety and Important Interactions
A smooth recovery can get off track fast if the medication plan is unclear. The preventable problems I see most often are not rare allergic emergencies. They are dosing mistakes, duplicate ingredients, and avoidable interactions that start with an incomplete medication list.
Before surgery, your oral surgeon needs an accurate picture of what you take, what you have reacted to in the past, and what medical conditions could change the safest plan. That is especially important if the goal is a lean, evidence-based recovery with the fewest medications necessary.
What to tell your surgeon before the procedure
Bring a written list or a photo of every medication bottle. Memory is unreliable, especially if you take several prescriptions, use supplements, or only take certain products occasionally.
Include:
- Prescription medications such as blood thinners, blood pressure medicines, antidepressants, stimulants, seizure medications, diabetes drugs, and anything used for chronic pain
- Over-the-counter products including ibuprofen, acetaminophen, aspirin, sleep aids, allergy medicines, and cold or flu remedies
- Supplements and herbals such as fish oil, garlic, ginkgo, turmeric, St. John's wort, and anything marketed for sleep, stress, or inflammation
- Allergies and past reactions to antibiotics, pain medicines, latex, local anesthetics, or sedation medications
- Health conditions such as kidney disease, liver disease, ulcers, reflux, bleeding disorders, pregnancy, sleep apnea, and any history of difficult anesthesia or severe nausea after surgery
Details matter here. For example, ibuprofen may be appropriate for one patient and a poor choice for another with kidney disease, stomach ulcers, or certain bleeding risks. Sedating medication also deserves extra caution in patients with sleep apnea or those already taking other drugs that cause drowsiness.
Common mistakes after surgery
The biggest hazards usually come from ordinary decisions made when a patient is tired, numb, or trying to stay ahead of pain.
- Mixing products without checking the label. Many combination medicines already contain acetaminophen or another pain reliever.
- Adding alcohol or recreational drugs. Sedation, opioids, anti-anxiety medicines, and alcohol can combine in dangerous ways.
- Using leftover medication from a prior procedure or from another person. The right drug for someone else may be the wrong drug for you.
- Taking extra because the first dose did not work fast enough. Many medicines need time to reach effect, and stacking doses can create more risk than benefit.
- Doubling a missed dose. Follow the written instructions or call the office if the schedule gets off track.
One practical rule helps. Use one written schedule, one measuring device for liquids, and one person to track each dose if more than one adult is helping at home.
Storage and disposal matter
Any sedating medication should be stored securely, especially opioids if they were prescribed at all. A bathroom counter, kitchen table, or backpack is not a safe place for them. Leftover tablets should not stay in a drawer for future dental pain, because the next episode may need a different diagnosis and a different treatment plan.
If your care also involves facial pain, jaw dysfunction, or sleep-related contributors to pain sensitivity, Pain and Sleep Therapy Center offers TMJ, facial pain, and regenerative services through a root-cause model rather than relying on long-term medication alone. For wisdom tooth recovery, the immediate priority is simpler. Take only the medications your surgeon recommended, in the dose and timing provided, and ask before adding anything else.
Ask questions before surgery day if any part of the medication plan is unclear. It is much easier to prevent a mistake than to fix one after you are home and reading labels through swelling and fatigue.
Beyond Pills Non-Drug Pain Control Strategies
Medication helps, but it isn't the whole recovery. The body heals better when swelling is controlled, the surgical site is protected, and the nervous system isn't constantly being irritated.

Use cold, rest, and food strategically
During the early phase, cold packs on the outside of the cheek can reduce swelling and make the area less reactive. Rest matters just as much. Patients who try to power through errands, workouts, or late nights often feel worse than patients who let the first day be quiet.
Food choice matters more than many people expect. Soft, non-irritating meals reduce mechanical stress on the surgical area and make it easier to stay nourished. Yogurt, smoothies eaten without a straw, mashed foods, soups that aren't too hot, eggs, and soft rice dishes are usually easier than crunchy or chewy foods.
Protect the clot and support healing
The early blood clot is part of healing, not something incidental. Rough rinsing, forceful spitting, smoking, aggressive brushing near the site, and straw suction can disturb it. Once your surgeon says it's appropriate, gentle saltwater rinses can help keep the area cleaner without the harshness of strong mouthwashes.
A practical home plan often looks like this:
- Cold outside the mouth to calm swelling.
- Soft foods and good hydration so you don't fall behind nutritionally.
- Head elevation during rest to limit throbbing and puffiness.
- Gentle oral hygiene that respects the surgical site.
- Low-stimulation recovery with reading, music, or simple distraction instead of constant talking and activity.
Biology-first options
In some practices, recovery support may also include regenerative approaches such as platelet-rich fibrin, or PRF, which uses the patient's own biology to support healing. That's not standard in every wisdom tooth case, but it reflects an important principle I agree with: help the tissue heal well, and you often reduce the need for more medication later.
Non-drug care isn't an optional extra. It's one of the main reasons many patients can stay comfortable with a lighter medication plan.
When to Call Your Surgeon A Clear Checklist
Most recoveries are uneventful. Some soreness, swelling, limited jaw opening, and mild oozing are expected. The key is knowing when the pattern stops looking normal.
Call your surgeon if you notice any of the following:
- Pain that isn't controlled by the prescribed plan or pain that sharply worsens after an initial period of improvement. That can signal a complication such as dry socket or another issue that needs direct evaluation.
- Bleeding that doesn't settle with pressure or bleeding that feels heavy rather than like minor oozing. Persistent bleeding deserves a call.
- Fever, pus, foul-tasting drainage, or a worsening bad smell from the extraction area. Those can point to infection.
- Swelling that keeps increasing instead of leveling off, especially if it becomes hard, hot, or associated with difficulty swallowing.
- Trouble breathing, severe rash, or concerning medication reactions. Those need urgent medical attention.
- Vomiting, inability to keep fluids down, or extreme dizziness after surgery or medication use. Dehydration can make recovery spiral quickly.
If you're unsure whether a symptom is urgent, it's better to ask than to guess. Patients sometimes find it useful to read broader after-hours warning signs in resources such as Skotzko Dental's emergency extraction guide, but your own surgeon's instructions always come first. If you need immediate local help, a 24-hour emergency dentist resource can help you find the right next step.
Normal healing should trend in the right direction. If you're moving backward instead of forward, call.
If you're preparing for wisdom tooth removal and want a careful, root-cause-minded approach to oral and facial pain, Pain and Sleep Therapy Center offers evaluation and treatment for TMJ disorders, facial pain, and related recovery concerns. When medication plans need to be adapted to the whole patient, not just the extraction site, that kind of individualized care matters.



