
A lot of people arrive at the phrase facial surgery center in the same state of mind. They have jaw pain that won't quit, headaches that keep circling back, a bite that feels off, trouble chewing, or a referral slip that suddenly makes everything sound serious. The word “surgery” can make it feel as if a major decision has already been made for you.
Usually, it hasn't.
A referral to a facial surgery center often means you need a deeper evaluation, not automatic surgery. That distinction matters. Some patients do need an operation for trauma, jaw alignment, airway anatomy, tumors, infection, or reconstruction. Many others need a careful diagnosis first, because facial pain and jaw dysfunction can come from muscle strain, joint inflammation, airway issues, clenching, bite instability, nerve irritation, or a mix of problems that surgery alone won't solve.
Modern care also looks different than many people expect. In the United States, the ambulatory surgery center industry was valued at about $45.6 billion, and these outpatient facilities now host more than 80% of all U.S. surgeries, reflecting a major shift toward lower-cost, high-efficiency care settings that include facial procedures, according to Dialog Health's ASC statistics summary. That means your care may happen in a specialized outpatient environment rather than a large hospital, depending on the procedure and your medical needs.
The more useful question is often not “Where can I get surgery?” It's “What exactly is causing this, and what level of care fits the problem?”
Navigating Your Path to Facial Health and Relief
You may be reading this after a dentist mentioned your TMJ, after an ENT suggested a jaw evaluation, or after weeks of searching symptoms at midnight because your face hurts, your jaw clicks, and your sleep has gotten worse. That uncertainty is common. Patients often worry that seeing a facial specialist means they're already on a one-way path to an operating room.
That's rarely the right mindset.
A good facial care pathway starts with sorting the problem into the right bucket. Is this a pain problem, a joint problem, a bite problem, an airway problem, a trauma problem, or a structural problem that surgery can correct? Those are not interchangeable. The treatment that helps one may do very little for another.
A smart consult should narrow the diagnosis before it narrows the treatment.
For some people, the answer is straightforward. A fracture, severe facial asymmetry with functional impairment, or a jaw position problem affecting chewing and airway function may point toward surgery. For others, the better first step is conservative care: muscle treatment, bite stabilization, airway assessment, habit reversal, breathing retraining, inflammation control, or physical rehabilitation.
What patients often get wrong
The biggest mistake isn't fear. It's assuming all facial symptoms come from one structure.
Jaw pain may be blamed on the joint when the primary driver is muscle overload. Headaches may be treated as a sinus issue when clenching or sleep-disordered breathing is part of the picture. Facial tension may look dental but track with posture, oral habits, or poor nasal breathing. If the diagnosis is broad and vague, the treatment usually becomes broad and disappointing too.
What helps most at the start
Before anyone talks seriously about an operation, you need clarity on three things:
- Where the problem is centered: joint, muscles, teeth, nerves, airway, bone, soft tissue, or a combination.
- What has already been tried: bite guards, medications, therapy, injections, dental work, CPAP, orthodontics, or prior surgery.
- Whether the condition is stable or changing: pain that fluctuates is different from a structural issue that predictably worsens function.
That's the fundamental starting point. Surgery is one tool inside facial care. It isn't the definition of facial care.
Defining the Modern Facial Surgery Center
A modern facial surgery center is best understood as a specialized outpatient setting built around diagnosis, procedures, anesthesia coordination, and recovery for conditions involving the face, jaws, mouth, airway, and related structures. It isn't one specialty in one room. It's closer to a master workshop, where different experts handle different parts of a highly detailed problem.
The three broad domains
While the phrase is often used loosely, facial surgical care usually falls into three broad domains.
Reconstructive care addresses damage or deformity caused by trauma, cancer treatment, congenital differences, or tissue loss. The goal is function first, then form.
Cosmetic care focuses on appearance-based changes such as rhinoplasty, eyelid surgery, facial contouring, and rejuvenation procedures. Some patients who begin with cosmetic questions also explore less invasive options first, including Botox and skincare upgrades, because not every concern requires an operation.
Oral and maxillofacial care covers teeth, jaws, bite relationships, facial bones, oral pathology, wisdom teeth, implants, jaw surgery, trauma, and some airway-related issues. For patients dealing with skeletal bite problems or functional jaw mismatch, a resource on surgery for jaw realignment can help clarify where orthognathic surgery fits.
Why you may see different specialists
Facial surgery is multidisciplinary. A national survey of top trauma centers found facial trauma coverage was provided by plastic surgeons in 39.6% of centers, oral and maxillofacial surgeons in 36.6%, and otolaryngologists in 23.3%, according to the PubMed record of the trauma-center survey. That distribution reflects how the field works. Different anatomy, different training, different problems.
Here's a practical way to understand it:
| Specialist | Often handles | Common reason for referral |
|---|---|---|
| Plastic surgeon | Soft tissue reconstruction, cosmetic facial work, some trauma | Aesthetic goals or reconstructive needs |
| Oral and maxillofacial surgeon | Jaws, teeth, facial bones, bite, oral surgery | TMJ-related structure questions, jaw surgery, extractions, trauma |
| ENT or head and neck surgeon | Nose, sinuses, airway, ears, throat, related facial structures | Breathing, sinus, airway, or head and neck concerns |
The right specialist depends less on the symptom location than on the structure causing it.
A true facial surgery center should help sort that out rather than forcing every patient toward the same answer.
How to Evaluate a Facial Surgery Center
You sit down for a consultation because your face hurts, your bite feels off, or breathing has become harder than it should be. Ten minutes later, someone is already talking about a procedure date. That is the moment to slow down.
A facial surgery center should help confirm what is wrong before it recommends how to fix it. Some centers do that well. Others are organized around procedures first. Patients feel that difference quickly in the quality of the exam, the clarity of the explanation, and whether non-surgical causes are taken seriously.
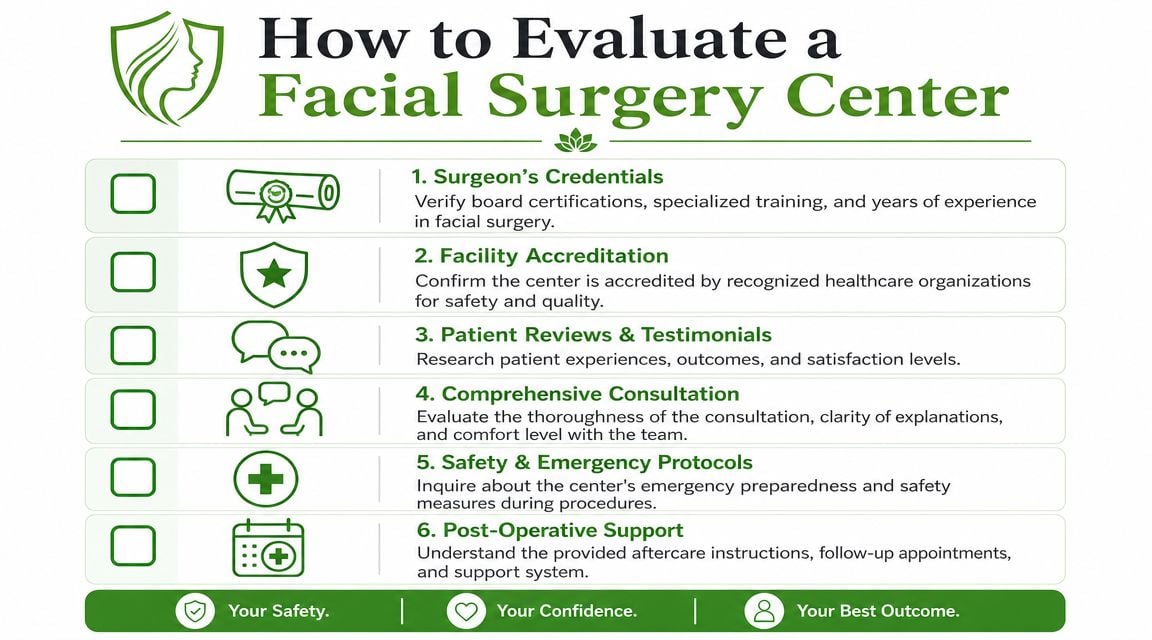
Start with a visual checklist.
Look past the marketing language
Strong centers explain the decision-making process in plain English. You should know who will perform the procedure, who will manage anesthesia, what imaging or other workup is needed, and what happens if the diagnosis changes after a closer exam. If those answers stay vague, the center may be better at promotion than patient selection.
That matters because many facial complaints are not surgical problems at first presentation. Muscle-driven jaw pain, clenching, airway-related strain, dental wear, sinus disease, and nerve pain can mimic structural surgical issues. A careful center sorts those out instead of forcing every patient into the same pipeline.
It can also help to compare how different clinics present their philosophy of care. For a non-surgical example of how a clinic communicates patient experience and scope, Skinsation Aesthetics Inc.'s London clinic gives a useful reference point for the kind of professionalism and communication many patients look for.
Examine the facility, not just the consultation room
The procedure space tells you a lot about how seriously a center treats safety. Guidance summarized in Plastic Surgery Key's discussion of office-based surgery center design notes that operating room floors should be continuous and made of cleanable materials, and ceilings should also be continuous rather than standard drop ceilings that can collect dirt and bacteria. The same discussion explains that operating room lighting must support accurate tissue and blood-color assessment, which directly affects precision during facial procedures.
Those details are easy to miss if you are focused on symptoms, cost, or scheduling. They still matter. Facial surgery is done in tight spaces, often close to the airway, major nerves, and structures that affect appearance and function at the same time.
Ask practical questions:
- Where is the procedure performed? A true operating room is different from a treatment room adapted for minor procedures.
- Who is responsible for airway management and monitoring? Facial procedures and sedation can complicate access to the airway.
- What monitoring is standard during the case? Clear, specific answers are better than reassurance alone.
- What type of anesthesia is offered for my procedure, and why? A center should be able to explain the reasoning. This overview of oral surgery anesthesia options can help you know what to listen for.
A short overview can help you understand what to listen for during a consult:
Compliance needs to be visible in the process
Regulatory compliance is not paperwork for its own sake. It shows up in infection-control protocols, medication handling, staff credentialing, emergency drills, and the center's transfer plan if a patient needs hospital-level care.
For this section, I would focus less on whether a center says it is compliant and more on whether staff can describe what that means in daily practice. Ask how instruments are processed, how emergencies are handled, and how surgeon and anesthesia credentials are verified. Centers that run well usually answer these questions without defensiveness or confusion.
Practical rule: If a center cannot clearly explain infection control, emergency readiness, and hospital transfer procedures, keep looking.
What a strong consultation feels like
A good consultation leaves you with a diagnosis, a differential, or a clear plan to get one. It does not leave you with pressure.
The best centers review trade-offs transparently. Surgery may improve structure but not muscle-driven pain. It may help breathing while adding recovery time, cost, and swelling. In other cases, physical therapy, bite stabilization, nasal treatment, sleep evaluation, or habit control should come first. That is the kind of judgment patients should look for.
Questions to Ask Before Committing to Surgery
The most productive consultation is not the one where you nod politely and leave with a brochure. It's the one where you ask precise questions and get specific answers. That doesn't make you difficult. It makes you safe.
Ask diagnosis questions first
Before discussing technique, ask whether the diagnosis is firm or provisional. Facial pain, jaw locking, chewing difficulty, and facial tension can overlap across joint, muscle, dental, airway, and neurologic causes.
Use questions like these:
- What exactly are you treating: Is the main problem the joint, muscles, bite, bone position, airway, soft tissue, or something else?
- What findings support that diagnosis: Imaging, physical exam, airway screening, bite analysis, motion limits, or symptom pattern?
- What else is still on the differential: If surgery doesn't address those possibilities, you need to know that now.
Ask about the procedure and anesthesia
The next layer is procedural clarity. Don't settle for general phrases like “we'll fix the issue” or “you'll be more comfortable afterward.”
Ask:
- What is the operation called, and what does it change anatomically?
- What improvement should I realistically expect in pain, function, breathing, appearance, or chewing?
- What are the important risks in my case, not just the standard form risks?
- What type of sedation or anesthesia will be used? If you need background on that part of care, this guide to oral surgery anesthesia is a helpful companion.
- What would make you decide not to proceed on the day of surgery?
Ask the questions that reveal whether surgery is premature
These are often the most important ones.
- What non-surgical options should be tried first, if any?
- What is the risk of waiting and monitoring instead of operating now?
- If my pain improves but the anatomy doesn't change, would surgery still be necessary?
- What kind of patient tends to do poorly with this surgery?
- How will we know afterward whether the surgery solved the original problem?
A trustworthy surgeon won't be irritated by conservative questions. They'll usually welcome them.
If the answers are evasive, overly certain, or disconnected from your actual symptoms, pause before moving forward.
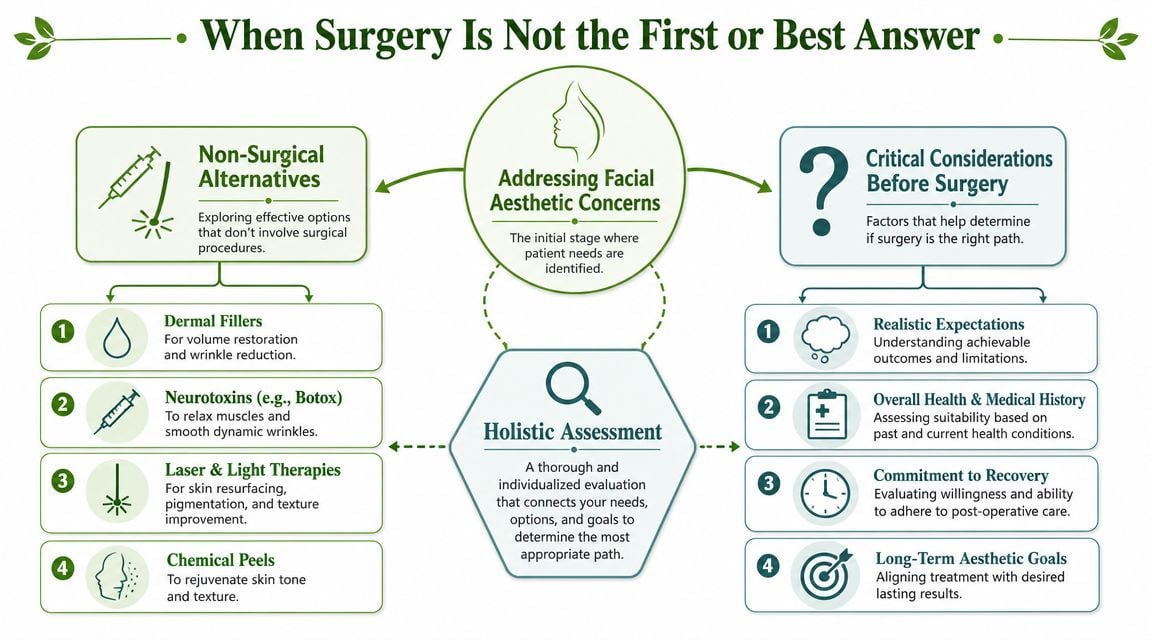
When Surgery Is Not the First or Best Answer
Many people searching for a facial surgery center are not looking for surgery as much as they're looking for relief. They want the jaw to stop hurting, the headaches to stop building, the clicking to make sense, or the fatigue and snoring to stop disrupting life. That's where many facial-care websites fall short. They list procedures, but they don't help patients decide whether a procedure belongs in the plan at all.
The more accurate approach is diagnose first, operate only when the diagnosis supports it.
According to the University of Washington Oral and Maxillofacial Surgery overview, oral and maxillofacial specialty care includes diagnosis and conservative management, not just surgery. That's an important consideration for TMJ disorders, facial pain, and some airway-related complaints, because the first-line answer may be non-surgical even when the symptoms feel severe.
Problems that often need broader evaluation
Surgery is usually a poor first move when the main complaint is pain without clear structural pathology. It's also worth slowing down when symptoms fluctuate with stress, sleep quality, posture, clenching, chewing load, or airway congestion.
Common examples include:
- TMJ pain with muscle dominance: The joint gets blamed, but the muscles are doing most of the suffering.
- Chronic headaches with jaw tension: The trigger may be parafunction, neck mechanics, or sleep-disordered breathing rather than a surgical lesion.
- Facial pain with normal imaging: If scans don't match the intensity of symptoms, the answer may lie in nerve sensitivity, muscle guarding, or functional overload.
- Airway complaints with daytime fatigue: A structural issue may exist, but evaluation often needs to include sleep and breathing patterns, not just anatomy.
What conservative care can look like
Non-surgical treatment isn't passive. Good conservative care is targeted and active.
That may include bite stabilization, physical therapy, airway assessment, myofunctional therapy, breathing retraining, guided exercises, sleep-focused treatment, habit reversal, anti-inflammatory strategies, and regenerative approaches such as Prolotherapy or PRF injections when a clinician determines they fit the case. In some patients, these methods reduce the need for surgery. In others, they clarify whether surgery is still necessary.
Aesthetic patients face a similar decision process. Someone bothered by laxity, volume loss, or skin texture may explore no-knife facial lifting options before considering a formal operation. The lesson applies more broadly: treatment should match the problem's depth and cause.
Surgery works best when it solves a structural problem. It works poorly when it's asked to solve an unconfirmed pain syndrome.
Signs you may need diagnosis before any procedure
A pause is wise if any of these sound familiar:
| Situation | Why caution helps |
|---|---|
| Your pain moves around | Migrating symptoms often suggest functional or muscular drivers |
| The worst symptoms occur at night or on waking | Sleep, clenching, or airway issues may be involved |
| Prior dental or medical treatment didn't change the pattern | The original diagnosis may have been incomplete |
| Your imaging looks “not that bad” but your pain is intense | Pain amplification or non-structural factors may need attention |
When surgery becomes the right answer
None of this means surgery is wrong. It means surgery should be used for the right reasons. Clear facial fractures, destructive pathology, major bite discrepancies, severe structural obstruction, unstable deformity, or anatomy-driven dysfunction may absolutely justify it.
The key is sequencing. The best outcomes usually come when the team identifies what is structural, what is inflammatory, what is muscular, and what is behavioral or airway-related. Once those layers are separated, the treatment plan gets sharper and more effective.
What to Expect During Recovery and Aftercare
Recovery starts before the procedure. A patient who arranges meals, sleeping support, medications, rides, and time away from work usually has a smoother first week than the patient who focuses only on the surgical date. I tell patients to treat aftercare as part of the operation, because the quality of healing often depends on the first several days at home.

The early recovery window
Expect swelling, soreness, stiffness, bruising, and fatigue. The pattern depends on the procedure. Jaw surgery often affects chewing and speech for a period. Nasal or airway procedures can temporarily change breathing comfort, sleep quality, and moisture in the nose and throat. Reconstruction after injury may add numbness, asymmetry, or a longer timeline for soft tissue settling.
Healing rarely follows a perfectly straight line. Mornings may feel tighter. Swelling can shift. One side may look ahead of the other for a while.
A few habits make a real difference:
- Protect the surgical area: Follow cleaning, wound care, mouth rinses, and cold-therapy instructions exactly as prescribed.
- Follow diet limits: Advancing food texture too quickly can increase pain, irritate tissue, and set healing back.
- Sleep with support: Head elevation and stable positioning often reduce swelling and make rest easier.
- Show up for follow-up: Small concerns are easier to address early, before they become larger problems.
Aftercare should be clear before you ever go home
A well-run center does more than perform the procedure. It gives patients written instructions, a way to reach the team after hours, and clear thresholds for when to call urgently. Ask those questions before surgery, not while you are groggy and trying to remember discharge paperwork.
Call promptly for breathing trouble, bleeding that does not slow, swelling that rises quickly, fever, or pain that becomes sharper instead of gradually easing. Those changes deserve direct guidance.
If your operation followed an injury, recovery may involve several goals at once. Bone healing, bite function, facial movement, sensation, and appearance do not always improve on the same schedule. Patients recovering from facial trauma surgery often do better when they understand that function usually takes priority first, with swelling and contour changes settling over time.
Give the result time to declare itself
Early healing can be visually misleading. Tissues may look uneven, feel firm, or seem overcorrected before they soften and settle. That is common. It is also one reason I urge patients to avoid judging the outcome too soon or comparing day-by-day photos without context.
Good recovery also means knowing when surgery did its job and when another issue still needs attention. If pain persists in a pattern that seems out of proportion to the healing exam, the next step may be reassessment for muscle tension, nerve irritation, sleep-related clenching, sinus disease, or another non-surgical driver. The best facial care does not stop at the operating room. It follows the symptoms until the cause is clear.
Frequently Asked Questions About Facial Care
Do I need a facial surgery center if I have TMJ pain
Not necessarily. TMJ pain can come from the joint, but it can also come from muscles, clenching, airway issues, bite strain, or referred pain patterns. If the symptoms are mostly pain, tightness, or headache without a clear structural finding, a diagnostic evaluation is often more useful than jumping straight to surgery.
What's the difference between an oral surgeon and a TMJ specialist
An oral and maxillofacial surgeon treats diseases and conditions involving the mouth, jaws, and facial structures and can perform procedures when surgery is appropriate. A TMJ-focused clinician may concentrate more heavily on joint function, muscle pain, bite issues, behavioral factors, and conservative treatment. Some patients need one. Some need both.
When should a primary care doctor, dentist, or ENT refer to a facial surgeon
Referral makes sense when there is trauma, suspected structural pathology, progressive functional limitation, significant bite change, persistent trismus, infection, or imaging findings that may need procedural management. When the picture is dominated by chronic pain, headaches, clenching, poor sleep, or variable symptoms, referral to a non-surgical facial pain or airway-focused provider may be the better first step.
If imaging shows something abnormal, does that mean I need surgery
No. Imaging has to match symptoms, exam findings, and functional impairment. Many patients have visible abnormalities that don't explain their pain well. Surgery should treat the actual pain generator or functional deficit, not just a scan finding.
Can children ever need facial or oral procedures in this care category
Yes. Pediatric oral and facial care can include tongue-tie evaluation, laser frenectomy, airway-related concerns, facial growth questions, trauma, and developmental issues. The right setting depends on the child's age, health, procedure type, and whether the concern is functional, surgical, or both.
What if I've already tried several treatments and still don't feel better
That's often a sign the diagnosis needs a fresh review, instead of a stronger version of the same treatment. Refractory facial pain can involve overlapping drivers. A clinician should reconsider the joint, muscles, nerves, airway, sleep quality, oral habits, cervical mechanics, and prior dental history together.
Is a hospital always safer than an outpatient facial surgery center
Not always. Safety depends on patient selection, procedure complexity, anesthesia planning, facility systems, and emergency readiness. Hospitals are appropriate for some higher-acuity cases. A well-run outpatient center can be an excellent setting for properly selected facial procedures.
How do I know whether I'm seeking relief or seeking the wrong tool
Ask yourself one question: do I have a confirmed structural problem, or am I mostly trying to stop pain and dysfunction? If the answer is unclear, slow down. The right diagnosis usually points toward the right level of treatment.
If you're dealing with TMJ pain, facial tension, headaches, snoring, sleep-disordered breathing, or jaw dysfunction and you want a diagnosis before jumping into surgery, Pain and Sleep Therapy Center offers root-cause evaluation and non-surgical care focused on function, comfort, and long-term relief.



