
The day a family hears the words “your baby has a cleft palate,” the room often goes quiet. One parent starts making a list of questions. The other is already worried about feeding, speech, anesthesia, and whether their child will be okay in the long run. Most families are not only thinking about surgery. They're thinking about first words, school pictures, breathing at night, and whether meals will ever feel easy.
Those concerns are valid. They also deserve answers that go beyond “we'll close the palate and see how things go.”
Cleft palate reconstruction is not a single event. It's a process of restoring structure, then supporting function as a child grows. The operation matters, but so do the muscles of the soft palate, the way the tongue rests, how a child breathes, how they learn to swallow, and how the face develops over time. Families do best when they understand the whole journey early.
Your Journey Begins Here A Compassionate Introduction
Parents usually arrive at this stage carrying two competing feelings. Fear is one. Relief is the other. Fear comes from not knowing what surgery involves. Relief comes from finally having a name for what's happening and a team to guide the next steps.
A new family may be dealing with a baby who takes a long time to feed, milk that escapes through the nose, or an early referral to a craniofacial team. Another family may have learned about the cleft on prenatal imaging and spent months waiting, wondering what life after birth will look like. Both experiences are common. Both can feel isolating.
The good news is that cleft palate reconstruction is one of the most established areas in craniofacial care. Modern repair is designed to do more than cover an opening. The goal is to rebuild a palate that can support feeding, speech, swallowing, and healthy facial growth.
What helps most early on: Parents don't need to master everything at once. They need a clear plan, a coordinated team, and honest expectations.
That plan usually starts with a few practical priorities:
- Feeding support first: Before surgery, many families need help with bottle selection, pacing, and positioning.
- Timing decisions: The repair is typically planned during infancy, with careful attention to speech development and healing.
- Long-term follow-up: Surgery closes the gap, but follow-up protects function.
- Team-based care: Children often need support from speech, dental, orthodontic, and airway-focused professionals over time.
Families often worry that one decision will determine everything forever. It won't. Good cleft care is not built on one perfect day in the operating room. It's built on thoughtful decisions over many years, with adjustments as a child grows.
Understanding Your Child's Cleft Palate
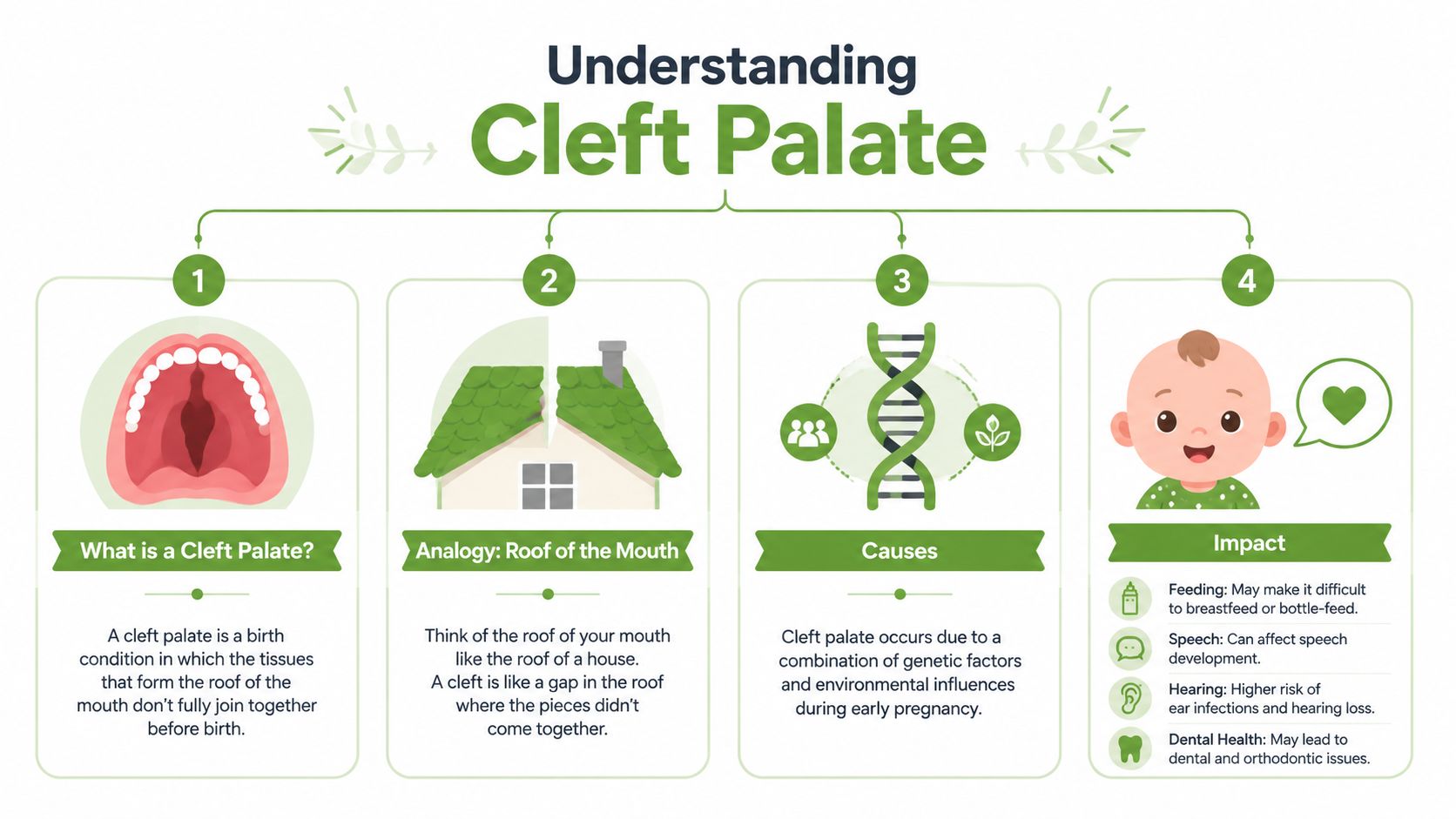
The palate is the roof of the mouth. It separates the mouth from the nose and gives the tongue a firm surface for feeding and speech. The front part is the hard palate, made of bone. The back part is the soft palate, made of muscle and soft tissue.
A cleft palate means that this roof didn't fully come together during development. Instead of one continuous surface, there is a gap. That gap changes how air, liquid, and food move through the mouth and nose. It can affect feeding early, then later influence speech, ear health, and dental development.
Why the muscles matter so much
The most important structure to understand is the levator veli palatini muscle. In a typical palate, this muscle helps lift the soft palate upward and backward so the mouth and nose can separate during speech and swallowing. In a cleft palate, that muscle is not arranged the way it should be. Instead of forming a useful sling, it is abnormally attached and runs front to back.
That's why cleft palate reconstruction is not merely a matter of stitching tissue together. A central goal is to reorient the levator veli palatini so it can work more normally for velopharyngeal closure, speech, and swallowing, as described in this review of cleft palate repair anatomy and surgical principles.
How a cleft affects everyday function
Parents usually notice function before they understand anatomy. The signs often show up in daily routines:
- Feeding challenges: Babies may have trouble creating suction, take longer to feed, or have milk come through the nose.
- Speech concerns later on: As language develops, the palate has to separate oral and nasal airflow for clear sounds.
- Swallowing mechanics: The soft palate plays a role in directing food and liquid appropriately.
- Breathing patterns: If oral posture and tongue posture adapt poorly over time, some children develop mouth-breathing habits that deserve attention.
A repaired palate should support a child's life, not just their operative note.
Why timing and evaluation matter
Surgical timing is based on function, growth, and the child's overall health. If you're trying to understand how teams think about that decision, this guide on the age for cleft palate surgery gives a useful parent-focused overview.
Families sometimes ask what caused the cleft. In most cases, it is understood as a mix of genetic and environmental influences rather than one simple explanation. What matters most after diagnosis is identifying the exact anatomy, supporting feeding, and planning reconstruction around the child's future function.
The Cleft Palate Reconstruction Surgery Explained
At some point, many parents sit across from me and ask the same question: “What exactly will you do in surgery?” They are not only asking about the day in the operating room. They are asking whether their child will be able to feed more easily, form clear speech, breathe well through the nose, and grow into a balanced pattern of oral function.
Those are the right questions.
The procedure aims to close the opening in the palate, rebuild the muscle sling of the soft palate, and create enough length and mobility for the palate to separate the mouth from the nose during speech and swallowing. Good cleft repair is functional reconstruction. The long-term goal is a palate that works with the tongue, jaw, airway, and facial growth, not a palate that is closed in isolation.

When repair is usually done
Many cleft teams plan palate repair during late infancy. Timing is a balance. Earlier repair may support speech development, while waiting slightly longer can give the surgeon more tissue to work with and may reduce some growth-related trade-offs. A parent-friendly discussion of that timing window appears in this review of palatoplasty outcomes and protocols, which also summarizes how outcomes vary by technique and cleft type.
This is also why cleft care fits within the broader field of reconstruction. Families who want a plain-language explanation of how reconstructive surgery restores bodily function often find it helpful, because the purpose of surgery is to restore use, not only appearance.
Two common approaches families may hear about
Surgeons choose techniques based on cleft width, palate shape, tissue quality, and the pattern of muscle disruption. The two names families hear most often are von Langenbeck palatoplasty and Furlow double-opposing Z-palatoplasty.
| Technique | Core idea | Main functional focus |
|---|---|---|
| von Langenbeck | Tissue is mobilized to close the palate | Tension-aware closure |
| Furlow double-opposing Z-palatoplasty | Tissue is rearranged in opposing Z patterns | Soft palate length and better muscle orientation |
The difference matters because long-term function depends heavily on how well the soft palate can move. In children who develop persistent mouth-open posture, low tongue posture, or nasal airflow problems later, the issue is not always the palate alone. But the initial repair sets the foundation for how the palate, tongue, and airway will work together during growth.
What outcome numbers can and cannot answer
The same review linked above reported favorable outcomes for Furlow repair in selected Veau 1 and 2 clefts and noted that velopharyngeal insufficiency after primary palatoplasty remains a real concern across techniques and centers. That is useful context, but families should hear the harder truth too. No percentage can tell you whether one operation is automatically best for your child's anatomy.
Technique choice is only part of the result. Width of the cleft, how the muscles are identified and repaired, scar behavior, healing, hearing history, and later speech follow-up all affect function. I tell families to listen closely when a surgeon explains not just how they close the palate, but how they restore movement.
Ask this directly: What functional problem is this operation designed to solve in my child, and how will you judge whether the palate is working well over time?
Questions to ask before surgery
A focused conversation before surgery often reduces anxiety and improves decision-making. These questions usually get to the heart of the plan:
- Which technique are you recommending for this specific cleft, and why?
- How will you repair and reposition the soft palate muscles?
- What speech or nasal air escape problems would make you watch for velopharyngeal insufficiency later?
- How do you think about airway, breathing pattern, and oral posture as my child grows?
- How will anesthesia and pain control be handled?
If anesthesia is one of your biggest concerns, this overview of oral surgery anesthesia can help you prepare for that discussion with your surgical team.
Assembling Your Child's Cleft Care Team
The best cleft outcomes come from coordination. No single specialist can manage feeding, speech, dental development, facial growth, airway concerns, and family support alone.
Parents often start by focusing on the surgeon. That makes sense. But long-term function depends on a broader team that sees the child from different angles.
Who is usually involved
A strong cleft team often includes these core roles:
- Plastic or craniofacial surgeon: Plans and performs the repair, then monitors healing, scarring, and later structural needs.
- Pediatrician: Tracks growth, feeding tolerance, ear infections, and overall development.
- Speech-language pathologist: Monitors resonance, articulation, and whether speech issues reflect structure, habit, or both.
- Orthodontist and pediatric dental team: Watches tooth eruption, arch form, bite development, and oral hygiene as the child grows.
- ENT specialist: Helps evaluate ear health and related concerns that commonly travel with cleft palate.
Some families also benefit from reading parent-friendly pediatric dental resources while learning how oral development affects the bigger picture. A community-oriented example is this article from Clayton Dental Studio, which explains why early dental guidance matters for children with developing mouths and jaws.
The often-missed members of the team
Two professionals are often underemphasized in standard surgical discussions.
The first is the orofacial myofunctional therapist. This clinician looks at tongue posture, lip seal, chewing pattern, swallowing mechanics, and whether a child is relying on compensatory habits after repair. Surgery can rebuild anatomy. It doesn't automatically train efficient function.
The second is an airway-focused specialist. Some children develop chronic mouth breathing, low tongue posture, restless sleep, or noisy breathing patterns that deserve attention. These are not side issues. They affect craniofacial growth, sleep quality, and muscle balance across the face and jaw.
Children don't use their mouths in isolated ways. Speech, swallowing, nasal breathing, and jaw mechanics influence one another.
Access and coordination matter
For some families, access is part of the challenge. Insurance limits, travel distance, and specialist shortages can make care fragmented. If you're trying to identify coverage-friendly options for surgical support, this resource on oral surgeons in Charlotte NC that accept Medicaid may help as a starting point.
A coordinated team doesn't mean more appointments for the sake of more appointments. It means fewer missed problems. That's what protects long-term function.
Navigating Recovery and Early Milestones
The first day after surgery is often harder on the parents than on the child. Families are watching every swallow, every nap, every cry. Most babies and toddlers look puffy, tired, and uncomfortable at first. That is expected.
In the hospital, the team usually focuses on pain control, hydration, and safe feeding. Your child may be fussy. Sleep may be irregular. Feeding may look different from what you're used to, and that change can feel unsettling even when healing is on track.
What the first stretch often looks like
Most families notice the same early themes:
- Mouth discomfort: Children may resist anything touching the palate.
- Changed feeding routine: Depending on the surgeon's instructions, you may use a cup, spoon, syringe, or another modified method.
- Protective measures: Some children go home with arm restraints, often called “no-nos,” to reduce the chance of hands or objects entering the mouth.
- Messier sleep and breathing sounds: Congestion and noisy breathing can happen during early swelling.
The care team will give precise instructions about what your child can drink, how to clean the mouth, and what activities to avoid. Follow those instructions exactly, even if your child seems to bounce back quickly.
The milestone parents remember most
It's often not the day of surgery. It's the first feed at home that goes more smoothly than expected. Or the first morning your child seems more like themselves. Or the moment you realize healing has moved from crisis mode into routine.
Some of the most important recovery signs are ordinary ones. Taking fluids. Settling to sleep. Fewer tears with feeding.
Families also benefit from seeing practical demonstrations from clinicians and parents. This video offers a useful look at the recovery period and what support can look like in real life.
When to call the surgical team
Call sooner rather than later if you notice concerns such as:
- Poor fluid intake: Fewer wet diapers or signs of dehydration
- Persistent bleeding: More than minor spotting
- Fever or unusual lethargy: Especially when paired with poor intake
- A sudden change in the mouth: Bad odor, wound opening, or increasing distress with feeds
Parents often worry they're overreacting. They usually aren't. Early questions are part of good recovery.
Long-Term Health Airway Speech and Facial Growth
A child can heal well from surgery and still need ongoing support. That's the part many families don't hear enough about at the beginning. Cleft palate reconstruction creates the foundation. Growth, speech learning, scar maturation, oral habits, and airway development shape what happens on top of that foundation.

Secondary surgery is part of the long view
Families often assume that more surgery automatically means something went wrong. That's not always true. Growth changes the face. Scar tissue matures. Speech needs become clearer with age. Some children eventually need additional procedures, but rates differ dramatically between centers.
A study highlighted by the American Society of Plastic Surgeons found secondary lip surgery rates ranging from 5% to 60% over ten years and secondary rhinoplasty rates from 47% to 79% by age 20, with no significant improvement in final appearance despite those interventions in the group studied. The same report described a 12-fold variation in secondary lip surgery risk across centers, underscoring how much protocols differ. The details are summarized in this ASPS press release on variation in secondary cleft surgery rates.
The practical lesson is not “avoid follow-up.” It's the opposite. Follow-up should be functional, not automatic.
Where airway and myofunctional development fit in
Long-term care takes on greater interest and importance. The palate does not work alone. It works with the tongue, lips, cheeks, jaw, nasal airway, and swallowing pattern.
If a child adapts by mouth breathing, holding the tongue low, thrusting during swallowing, or overusing facial muscles to compensate, those habits can influence:
- Speech clarity
- Nasal breathing
- Resting oral posture
- Chewing efficiency
- Jaw muscle tension and TMJ mechanics later
Scar tissue can also change how tissue glides and stretches. Even a technically successful repair may leave a child needing help with movement quality and coordination.
A functional palate is not just closed tissue. It is tissue that can move, coordinate, and support healthy habits.
Why therapy still matters after the palate is closed
Speech therapy is often the most visible part of long-term support, and families should take it seriously. For a broader parent-facing overview, these pediatric speech therapy insights explain why children often need guided practice even after structural issues have been addressed.
Beyond speech therapy, some children benefit from targeted work on oral rest posture, nasal breathing, and swallowing mechanics. That is where orofacial myofunctional therapy may help. It doesn't replace surgery, and it doesn't replace speech therapy. It addresses different questions. Is the tongue resting where it should? Can the child maintain lip seal? Are they breathing through the nose comfortably? Are there compensations that may create strain through the jaw and face?
Facial growth needs patience
One of the hardest parts for families is accepting that facial growth cannot be judged too early. A child's profile, bite, and airway pattern change over years. Some concerns settle. Others emerge gradually.
The healthiest mindset is long-term observation with purposeful intervention. Watch speech. Watch breathing. Watch oral posture. Watch sleep. The families who do best are rarely the ones who panic at every stage. They're the ones who stay engaged.
Frequently Asked Questions from Families
Will my child's speech sound normal?
Many children go on to have strong, understandable speech, but that outcome depends on more than closure alone. The palate has to move well, the muscles have to work in coordination, and the child may need speech therapy to build efficient sound patterns. If speech remains unusually nasal or hard to understand, the team should assess whether the issue is structural, learned, or both.
How do we choose the right cleft team?
Look for a team that talks about function as much as closure. Ask how they evaluate speech, feeding, dental development, facial growth, and airway concerns over time. A good team welcomes questions and explains not only what they plan to do, but why.
A few useful questions include:
- How do you assess soft palate function after repair?
- Who follows speech development?
- How do dental and orthodontic specialists fit into care?
- Do you evaluate breathing, oral posture, and swallowing habits as the child grows?
Will my child need more than one surgery?
Possibly. Some children do, and some do not. The need for later procedures depends on anatomy, growth, scar behavior, speech function, and center-specific practice patterns. It's better to think in terms of ongoing assessment than fixed predictions.
What if feeding is still difficult after repair?
That doesn't automatically mean something is wrong. Feeding often takes time to normalize because children are healing and adjusting to a different palate. Persistent problems deserve follow-up. Feeding struggles can reflect discomfort, oral aversion, coordination issues, or a need for more guided therapy.
Is access to care the same everywhere?
No. Access to timely cleft palate reconstruction varies widely across the world. In high-income countries, repair is typically done within the 9 to 18 month window, while low-resource settings may depend on short-term missions, leading to delays that raise the risk of speech issues and complications, as described in this report on barriers to reconstructive surgery in low- and middle-income countries.
That matters even if your family is receiving local care. It highlights why organized, multidisciplinary follow-up is so valuable.
How can we support our child emotionally?
Children take cues from their parents. Calm, confident routines help. So does speaking about treatment in matter-of-fact language. Let your child know they are safe, capable, and not defined by surgery. Connecting with other cleft families can also make the process feel far less lonely.
What should we keep watching as our child grows?
Keep an eye on the things that reveal function in daily life:
- Speech: clarity, effort, and nasal quality
- Breathing: nasal versus mouth breathing, especially during sleep
- Eating: chewing efficiency and messy or effortful swallowing
- Sleep: restlessness, snoring, or persistent fatigue
- Jaw comfort: clenching, facial tension, or pain as the child gets older
Families often expect the journey to end after the repair. In reality, that operation begins a new stage. With the right follow-up, that stage can be very positive.
If your child has a history of cleft palate repair and you're concerned about long-term breathing patterns, oral posture, swallowing mechanics, facial muscle tension, or sleep quality, Pain and Sleep Therapy Center offers airway-focused, root-cause care for children and adults. Their team evaluates how the mouth, jaw, and airway function together so families can address problems early and support healthier development over time.



