
If you're reading this before a medical appointment, there's a good chance you've already rehearsed the answer in your head.
“How bad is it on a scale of 1 to 10?”
Individuals often pause at that question. They don't pause because they aren't in pain. They pause because turning a lived experience into a single number can feel strangely hard, especially when the pain moves, changes, or behaves differently from one hour to the next. Jaw pain might be mild at breakfast, spike when you chew, and become a headache by evening. Facial pain might feel sharp one day and like pressure the next. Sleep-related pain problems add another layer because a rough night can make everything feel worse by morning.
That confusion is common, and it matters. The pain scale is useful, but it works best when you understand what the number is supposed to communicate. Research highlighted by the U.S. Pain Foundation notes that effective treatment plans can't be achieved without exploring the circumstances surrounding a person's pain, and that “a 10 on the pain scale means something different to everyone” in When the pain scale falls short.
The good news is that you don't need to guess. You can learn how to use the 1-10 pain scale in a way that gives your clinician a clearer, more complete picture. For complex conditions like TMJ disorders, facial pain, and sleep-related jaw tension, that extra clarity often leads to a better diagnosis and a more targeted plan.
That Moment the Doctor Asks About Your Pain
You might be sitting on an exam table, filling out intake forms, when someone asks for your number. If your pain has been going on for a while, the question can feel too small for what you're experiencing. If your pain is recent, you may worry about saying the wrong thing and not being taken seriously.
Both reactions make sense.
Pain is personal. Two people can have the same condition and use different numbers because they're describing different realities. One person is thinking about intensity. Another is thinking about whether they can still work, eat, or sleep. Someone with chronic TMJ pain may call it a 4 because they've learned to push through it, while another person with the same level of interference may call it a 7 because it dominates their attention.
Why the question still matters
The 1-10 pain scale isn't meant to reduce your experience to a scorecard. It's meant to give you and your clinician a shared starting language. That matters when providers need to compare today's pain with last week's pain, see whether treatment changed anything, or understand how symptoms shift with different activities.
A useful pain rating doesn't just say how much it hurts. It also hints at what the pain is stopping you from doing.
That second part is where many patients get stuck. They assume the right answer is the most dramatic number they can justify, or the most stoic one they can tolerate. Neither approach helps. The goal isn't to impress anyone. The goal is accuracy.
The real communication gap
The biggest challenge isn't that the scale exists. It's that people often use it without context. A single number can't show whether your jaw locks when you yawn, whether chewing steak causes a flare, or whether poor sleep makes your face ache the next day. Those details are often the key to understanding facial pain patterns.
When you treat the number as one piece of the story, it becomes much more helpful. It stops being a test and starts being a tool.
Decoding the 1-10 Numeric Pain Rating Scale
The formal name for the 1-10 pain scale is the Numeric Pain Rating Scale. In everyday practice, it gives patients a quick way to choose a number that reflects pain intensity. Clinicians use that number to track patterns, compare visits, and communicate clearly across a care team.
A simple way to think about it is a volume knob. Zero means the volume is off. Higher numbers mean the signal is louder and harder to ignore. But in medicine, the volume isn't judged only by sensation. It's also judged by what the pain does to your ability to function.
What the ranges usually mean
The most widely accepted functional grouping is described by the Shirley Ryan AbilityLab resource on the Numeric Pain Rating Scale. It classifies the scale like this:
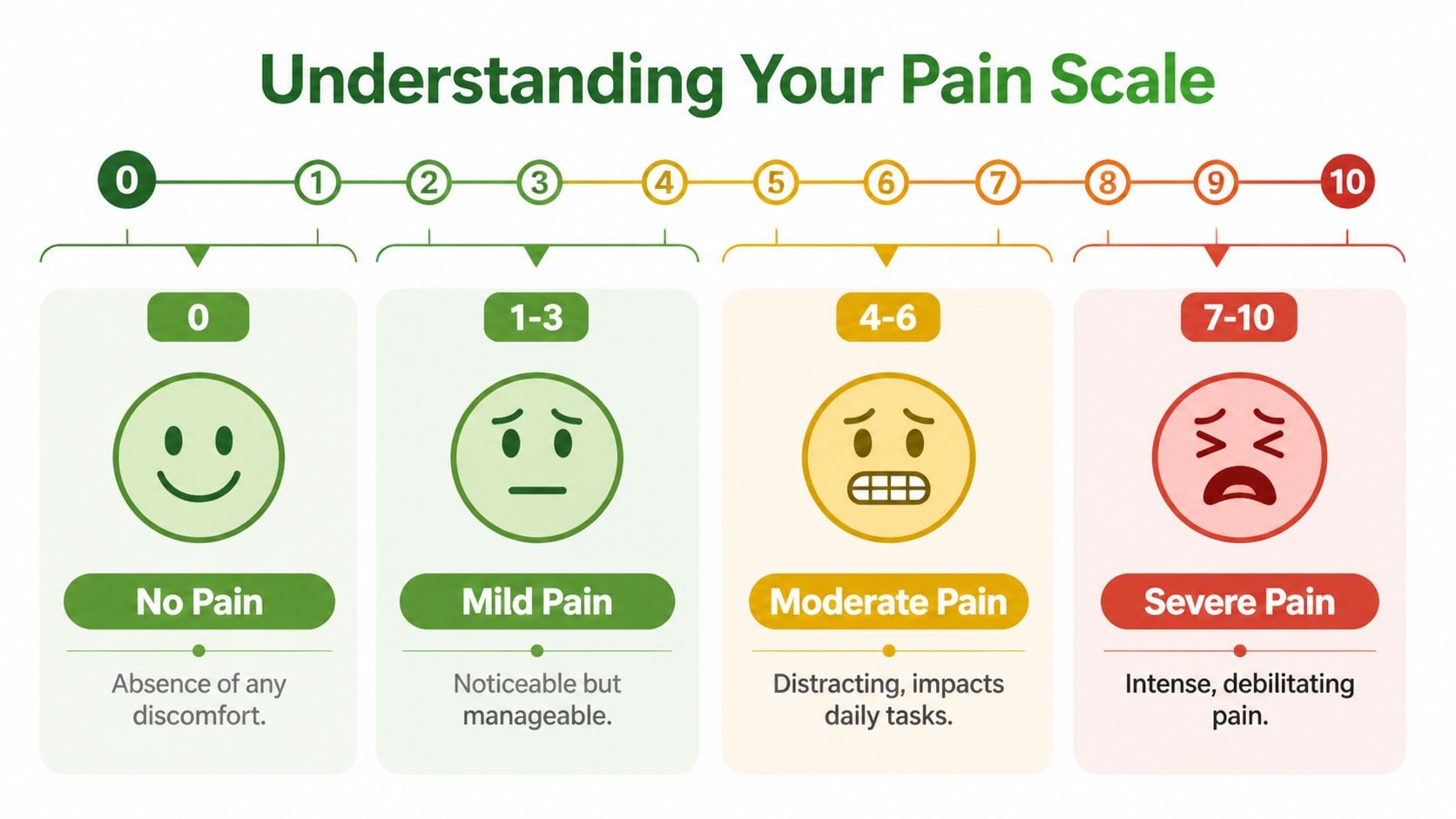
- 0 means no pain
- 1 to 3 means mild pain, which is minimally interfering with activities of daily living
- 4 to 6 means moderate pain, which interferes significantly with activities of daily living
- 7 to 10 means severe pain, which can be disabling and may make normal daily activities difficult or impossible
That functional framing is important. It gives the numbers practical meaning.
Think about function, not just feeling
If you're unsure whether your pain is a 3 or a 5, ask a different question. What is this pain doing to my day?
Consider these examples:
- Mild pain might be noticeable but not dominant. You can work, talk, cook, and focus, even if you wish the pain weren't there.
- Moderate pain starts taking up mental space. You may avoid harder foods, need breaks while speaking, or struggle to focus because the pain keeps pulling your attention back.
- Severe pain changes what you're able to do. You may stop eating certain foods altogether, cancel plans, lose sleep, or find it hard to get through routine tasks.
Why this helps with TMJ and facial pain
Jaw and facial pain often confuse people because the pain isn't always constant. It may be low at rest and jump with chewing, clenching, talking, or waking after a bad night of sleep. Using the 1-10 pain scale as a function-based tool makes it easier to answer accurately.
Practical rule: If the number feels hard to choose, start with how much the pain interferes with eating, speaking, concentrating, and sleeping.
That approach often gives a truer answer than trying to measure pain in a vacuum.
A Detailed Guide to Each Pain Level with Examples
Numbers become easier when you connect them to everyday life. For most patients, the best way to use the 1-10 pain scale is to match the number to both sensation and disruption. That's especially helpful for TMJ symptoms, facial muscle tension, tooth-adjacent pain, and pain that changes with sleep quality.
What each range often feels like
Below is a practical reference you can use before an appointment.
| Pain Level | Descriptor | Impact on Daily Life | TMJ/Facial Pain Example |
|---|---|---|---|
| 0 | No pain | You aren't aware of discomfort. Normal activity feels normal. | Your jaw moves comfortably, and you can chew, talk, and yawn without thinking about it. |
| 1 to 3 | Mild pain | You notice it, but it doesn't control your day. You can still do routine tasks. | A light ache in the jaw joint or cheek muscles that shows up when you first wake up or after a long conversation, but you can still eat and work. |
| 4 to 6 | Moderate pain | The pain becomes distracting. You may modify what you eat, how long you talk, or how well you concentrate. | Chewing a sandwich makes one side of your jaw hurt enough that you switch sides, take breaks, or avoid certain foods. A headache may start from clenching and affect focus. |
| 7 to 10 | Severe pain | The pain is intense and function drops sharply. Normal activities become difficult or feel impossible. | Jaw pain makes it hard to finish meals, speak comfortably, or sleep through the night. Opening your mouth widely feels overwhelming, or a flare leaves you unable to function normally. |
Real-life examples patients recognize
A 2 often sounds like this: “I can feel it, but I can ignore it when I'm busy.”
A 5 often sounds like this: “I can get through the day, but I'm changing what I do because of it.”
A 7 often sounds like this: “This is running the day. I'm not functioning the way I normally do.”
Those descriptions are more helpful than trying to compare your pain with childbirth, kidney stones, or a broken bone. You don't need a dramatic reference point. You need a number that reflects your own experience accurately.
For facial pain, the trigger matters
Two people may both report a 4, but one has a dull temple ache all day, while the other gets a sharp jolt only when chewing. Same number, different pattern. That's why clinicians caring for jaw and facial pain usually want more than the number itself.
Helpful add-ons include:
- When it happens. Morning, during meals, late in the day, after clenching, after poor sleep.
- What brings it on. Chewing, yawning, stress, talking, posture, exercise.
- How it feels. Aching, pressure, burning, throbbing, stabbing, tightness.
- What it limits. Eating, speaking, concentrating, sleeping, exercise, social time.
If your number changes depending on what you're doing, that's valuable information. It doesn't make your answer less accurate. It makes it more complete.
A common mistake to avoid
Many patients underrate chronic pain because they've adapted to it. They think, “I can still work, so it must be low.” But if you're cutting food into tiny pieces, avoiding chewy meals, rubbing your jaw all afternoon, and sleeping poorly, the pain is affecting function even if you've become used to it.
The right number isn't the bravest number. It's the one that best matches how much the pain is interfering with your life.
How to Report Your Pain More Accurately
The biggest upgrade you can make is simple. Don't report your pain as one frozen number if your symptoms change throughout the day.

For fluctuating conditions like TMJ and facial pain, a single score is only a snapshot. Physio-Pedia's overview of the Numeric Pain Rating Scale describes a better method: report your current, best, and worst pain over the past 24 hours, then use the average of those three ratings to reflect your overall pain level.
Use the three-number method
This works well because facial pain often follows patterns. Your pain might be:
- Current when you're sitting in the office
- Best after rest, heat, stretching, or a relaxed morning
- Worst during chewing, clenching, stress, or after a bad night of sleep
That gives your clinician a fuller view than one number alone.
For example, “Right now I'm a 3. My best was a 2 this morning. My worst was a 7 during dinner when chewing.” That's much more informative than saying only, “It's about a 5.”
Questions to ask yourself before the visit
A short pain log can help. You don't need anything fancy. A notes app or a piece of paper works well.
Ask yourself:
- What was I doing when the pain peaked
- What does the pain feel like at its worst
- What brings it down, even a little
- Does it affect chewing, talking, yawning, or sleep
- Is the pain worse in the morning, later in the day, or after certain activities
If you'd like a patient-friendly primer that reinforces this kind of thinking, Lake City Physical Therapy's pain guide offers a helpful plain-language overview.
A brief video can also make the process easier to picture:
A better sentence to bring into the room
Try this format:
“My pain is a 4 right now, but it rises to a 6 when I chew or talk for a long time. It feels like pressure near the jaw joint and a tight ache in my cheeks. It also disrupts sleep.”
That kind of answer gives your clinician intensity, pattern, quality, triggers, and impact. It's still concise, but it's far more useful.
The Limitations of Relying on Just a Number
Many patients feel frustrated by the 1-10 pain scale, and that frustration is reasonable. Pain isn't only intensity. It's also meaning, context, timing, fear, fatigue, and function.
One of the clearest examples of this gap appears in the NHSJS article On a scale of 1-10, how bad is your pain. It reported that approximately 75 percent of patients who rated their pain between 4 and 7 also described that pain as tolerable, even though that number range often signals a need for treatment. That disconnect shows why the number alone can miss the full picture.
What the number leaves out
A pain score doesn't automatically tell your clinician:
- The quality of pain. Sharp, dull, burning, throbbing, electric, pressure-like, tight.
- The pattern. Constant, intermittent, morning-only, meal-related, stress-related.
- The body area. Joint, muscle, teeth, temple, ear region, neck, tongue, throat.
- The effect on daily life. Trouble chewing, speaking, concentrating, exercising, or sleeping.
That's particularly important in jaw and facial conditions because many symptoms overlap. Muscle pain, joint irritation, nerve-related pain, headaches, airway-related strain, and sleep-related clenching can all be experienced differently even when patients choose the same number.
Why chronic pain often gets underrated
People who live with ongoing pain often adjust their lives around it. They eat softer foods, avoid gum, stop opening wide, sleep in certain positions, and build workarounds into the day. Then they report a modest number because the pain feels familiar.
Familiar doesn't mean minor.
If you're dealing with symptoms in the jaw, face, temples, or surrounding muscles, a more complete description of orofacial pain symptoms and causes can help you recognize patterns worth mentioning at your visit.
The most helpful pain report combines a number with a description of what the pain feels like, what triggers it, and what it stops you from doing.
What to say instead of only a number
You don't need medical jargon. Plain language works well.
Try phrases like:
- “It's a 5, but only when I chew.”
- “It's a 3 at rest and a 7 by the end of the day.”
- “The number isn't huge, but it's affecting sleep and eating.”
- “It's more tight and aching than sharp.”
That kind of detail often tells a clinician more than moving from a 5 to a 6 ever could.
Beyond the 1-10 Scale Other Ways to Describe Pain
The basic 1-10 pain scale is common because it's fast. But it isn't the only tool clinicians can use. Some situations call for a broader, more descriptive approach.

Two alternatives worth knowing
The FACES scale can help children, older adults, or anyone who has trouble translating pain into numbers. Instead of choosing a numeral, the patient chooses a face that best matches how they feel. That can lower confusion and make communication easier.
The Defense and Veterans Pain Rating Scale, often called DVPRS, takes a more multidimensional approach. According to the U.S. Department of Defense explanation of the Defense and Veterans Pain Rating Scale, the tool was created to address the limits of the standard 0-10 scale and includes functional descriptors so that successful pain management is associated with improved function rather than chasing zero intensity.
That idea matters in chronic facial pain. For many patients, progress doesn't mean a perfect zero every hour of the day. It means chewing more comfortably, sleeping better, speaking without strain, and having fewer disruptive flares.
Why a broader view can help
A richer pain assessment often looks at more than intensity alone:
- Function. What are you able to do now that pain had limited before?
- Pattern. Are flares shorter, less frequent, or easier to calm?
- Recovery. Does the pain settle faster after meals or stress?
- Quality of life. Are you sleeping more soundly or waking with less jaw tension?
People who are building a calmer recovery environment at home sometimes also look for gentle lifestyle supports, such as a low-chemical home collection that fits a rest-focused routine.
For persistent pain conditions, a multidisciplinary approach to pain management is often useful because pain can involve muscles, joints, nerves, breathing patterns, sleep, and stress responses all at once.
When Your Pain Score Means You Need to See a Specialist
A pain score matters, but the bigger question is this. Is the pain interfering with your life, and is there a pattern that deserves a closer look?
You should consider seeing a specialist if your pain is consistently in the moderate to severe range, if it keeps returning, or if the number doesn't seem dramatic but the impact is. A jaw pain score that seems “manageable” can still deserve attention if you're avoiding foods, limiting conversation, waking with headaches, or feeling worn down from broken sleep.
Signs that deserve more than watchful waiting
Seek further evaluation if any of these sound familiar:
- Your pain is changing how you eat. You avoid chewy foods, switch sides to chew, or feel sore after meals.
- Sleep is being disrupted. Pain wakes you, morning jaw tension is becoming routine, or poor sleep makes the next day worse.
- Your function is shrinking. Talking, yawning, exercising, or concentrating is harder than it should be.
- The pattern is persistent. Symptoms keep cycling back instead of settling.
- The pain spreads or overlaps. Jaw discomfort comes with temple pain, ear-area pain, headaches, or facial tightness.
Think beyond the number
A low number with a high daily cost is still important. So is a fluctuating number that points to a deeper mechanical or sleep-related issue. Posture and whole-body strain can also influence how pain behaves, which is why some patients find educational resources like PosturaZen on scoliosis pain helpful for understanding how musculoskeletal patterns can affect daily comfort more broadly.
If your symptoms center in the jaw, face, temples, or related muscles, finding a facial pain specialist near you can help move the conversation beyond “What number is it?” and toward “What's driving this, and how do we improve function?”
The best time to seek help is before the pain becomes your normal.
If jaw pain, facial pain, headaches, or sleep-related tension are affecting your daily life, Pain and Sleep Therapy Center can help you move beyond a simple number and toward a clear diagnosis and personalized treatment plan. Their team focuses on root causes, functional improvement, and practical care for TMJ disorders, orofacial pain, and sleep-related breathing issues.



