
You may be sitting with a treatment plan in your hand after hearing that jaw surgery is the answer to your bite, airway, or TMJ problems. That recommendation can bring relief. It can also bring pressure, because surgery sounds definitive, and when you’ve been in pain or struggling to function, a definitive answer is appealing.
Jaw surgery can help the right patient. It can improve facial balance, chewing, speech, and airway mechanics. But patients deserve the full picture before they commit to an irreversible procedure, especially when the jaw joints, nerves, muscles, and airway all have to adapt long after the incisions heal.
The phrase jaw surgery long term side effects matters because the true outcome of surgery isn’t measured only by the first few months. It’s measured by how your face feels, how your jaw functions, whether your bite stays stable, whether numbness resolves, and whether TMJ symptoms settle down or return years later.
Deciding on Jaw Surgery What You Need to Know First
A lot of people reach the surgical consult after a long stretch of frustration. They’ve tried splints, braces, physical therapy, soft foods, anti-inflammatory medication, maybe even CPAP or airway care. By the time surgery enters the conversation, they’re often tired and ready for a finish line.
That’s exactly why the decision has to be made carefully. Surgery can reposition bone, but it doesn’t automatically normalize muscle tone, joint loading, breathing patterns, oral posture, swallowing mechanics, or pain processing. If those drivers remain, the new jaw position still has to live inside the same body that created the problem in the first place.
For some patients, surgery is appropriate. For others, a second opinion focused on joint health, airway, muscle function, and conservative treatment changes the plan entirely. If you’re sorting through whether the procedure fits your case, this overview of surgery for jaw realignment can help frame the discussion in practical terms.
Ask what problem surgery is solving
Before saying yes, pin down the main target.
- Bite correction: Is the issue primarily skeletal, or is there a muscular habit that keeps pulling the jaw off track?
- Pain relief: Has anyone shown that your pain is coming from jaw position itself, rather than inflamed joints, overloaded muscles, or poor oral posture?
- Airway improvement: Is your airway problem structural only, or are tongue posture, nasal resistance, and breathing habits part of the picture?
- Appearance concerns: Are you prepared for the emotional adjustment that can come with facial change, even when the surgery is technically successful?
Practical rule: If the diagnosis is vague, the surgery discussion is premature.
Think beyond the operation
Patients often prepare for the operation date. They should also prepare for the adaptation phase that follows. Bone can be moved in one day. Functional recovery takes much longer, and it often depends on active rehab rather than passive waiting.
That’s where many people get surprised. They expect correction. What they experience is a long process of sensory change, muscle retraining, bite adaptation, and monitoring for relapse or joint strain.
Understanding the Spectrum of Long-Term Side Effects
Six months after jaw surgery, a patient may hear that the bones healed well and the scans look good, yet still struggle to feel a sip of water on the lower lip, tire through a normal meal, or notice that speech and bite contact still feel unfamiliar. That gap between surgical healing and functional recovery is where many long-term side effects show up.
These effects are not limited to one problem type. They can involve sensation, joint comfort, muscle endurance, bite stability, airway function, and the day-to-day coordination of chewing and speech. Surgery can deliver meaningful improvement, but it also changes mechanics that the joints, nerves, muscles, tongue, and brain then have to adapt to.
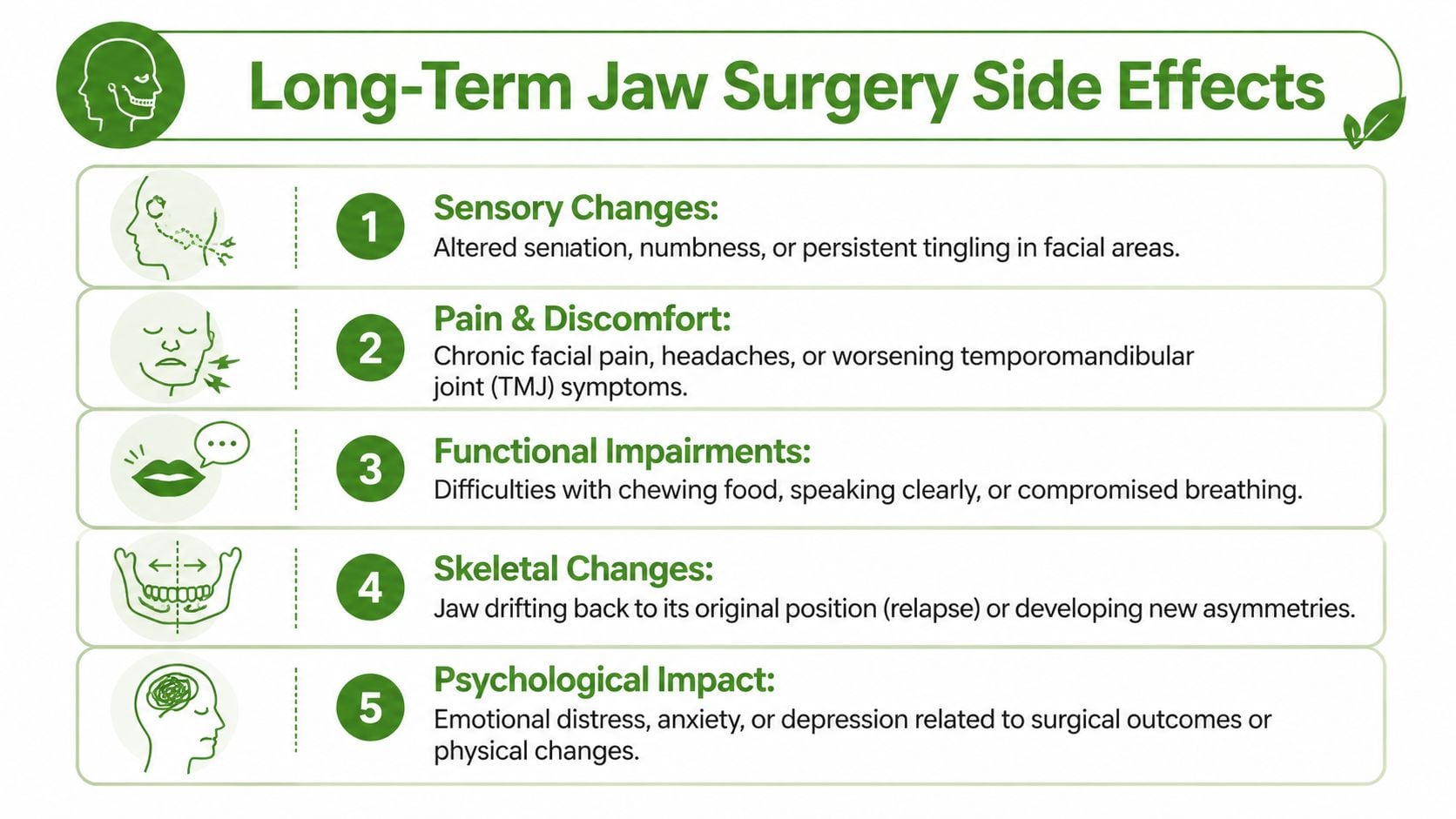
Common long-term side effects of jaw surgery at a glance
| Side Effect | Incidence Rate | Typical Timeline | Key Symptoms |
|---|---|---|---|
| Sensory nerve changes after orthognathic procedures | As high as 50% according to PMC review data | May improve over months, but some changes persist long term | Numbness, tingling, altered temperature sensation, reduced lip or chin awareness |
| Persistent sensory changes involving the inferior alveolar nerve | 25% with persistent changes beyond several months in the same review | Several months to over a year in some patients | Lip and chin numbness, altered touch, difficulty judging food or saliva |
| Permanent lingual nerve alteration | Less than 1% in the same review | If permanent, long term | Altered tongue sensation |
| Persistent hypoesthesia one year after SSRO in patients under 19 | 4.8% in the same review | One year and beyond | Ongoing reduced sensation |
| Persistent hypoesthesia one year after SSRO in patients age 19 to 30 | 7.9% in the same review | One year and beyond | Ongoing reduced sensation |
| Persistent hypoesthesia one year after SSRO in patients over 31 | 15.2% in the same review | One year and beyond | Ongoing reduced sensation |
| Upper lip numbness after upper jaw surgery | Most resolve in weeks, with less than 1% long term in the same review | Usually weeks, occasionally longer | Numb upper lip, altered lip feel |
Sensory changes affect daily function
Numbness sounds minor until it interferes with eating, speaking, shaving, applying lipstick, sensing saliva, or judging temperature. Patients often describe the area as present but unfamiliar. That distinction matters because altered sensation can be more disruptive than simple pain.
Age also changes the discussion. The same review reports lower rates of persistent hypoesthesia at one year in younger patients and higher rates in older adults. In practice, that means recovery expectations should be individualized, not handed out as a standard script.
This is also where early supportive care matters. Sensory re-education, myofunctional work, soft-tissue treatment, and careful monitoring of compensatory habits can improve function while the nerve recovers, and they help identify patients whose symptoms are no longer following a routine timeline.
Functional problems often become clearer later
Once swelling settles, some patients notice that the harder part is not healing from the incision. It is using the jaw normally again.
Chewing efficiency may drop before it improves. Speech can feel less automatic. Jaw muscles may fatigue faster. A bite may look acceptable on paper but still feel uneven in motion. Those problems are easy to dismiss if the focus stays only on bone position, yet they are often what determine whether a patient feels restored or still limited months later.
Patients with pre-existing pain, clenching, poor tongue posture, mouth breathing, or TMJ irritation deserve special attention here. Surgery can reposition the jaws, but it does not automatically correct the muscle patterns and airway habits that may have contributed to the problem in the first place. That is one reason non-surgical rehabilitation is so valuable, both before surgery and after it.
For readers also dealing with neck pain, nerve irritation, or overlapping pain conditions, this overview of spine and nerve disorders treated is useful because jaw symptoms rarely exist in isolation. The jaw, cervical spine, and surrounding nerves often influence one another.
Structural success and patient success are not always the same
A patient can have a technically sound result and still feel disappointed if the bite shifts, the joints become sore, the face feels tight, or the new position is difficult to maintain comfortably. I often tell patients to judge outcome in three categories at once.
- Comfort: numbness, headaches, muscle fatigue, joint irritation
- Function: chewing, speech, nasal breathing, sleep quality, endurance
- Stability: bite consistency, symmetry, and how well the result holds over time
That broader view matters because some long-term side effects are manageable if they are recognized early. Physical medicine, TMJ-focused care, regenerative injections in selected cases, airway-focused treatment, and myofunctional therapy can reduce strain and improve adaptation. In some patients, those same tools used earlier can lower the need for surgery at all by addressing root causes rather than only the final jaw position.
Unpacking the Causes of Post-Surgical Complications
Long-term complications don’t come from bad luck alone. They usually come from a mix of anatomy, mechanics, biology, and adaptation. Some risks are built into the procedure itself. Others depend on the patient’s joints, nerves, muscles, healing capacity, and the condition that led to surgery in the first place.
Procedure-related factors
The first category is mechanical. Orthognathic surgery requires cutting and repositioning bone in areas that sit close to important sensory nerves, joint structures, and muscle attachments. That proximity explains why numbness can happen even when the procedure is carefully planned and properly performed.
Hardware also matters. Plates and screws stabilize the new position, but they don’t eliminate the need for coordinated healing. The bones must heal, the condyles must seat well, and the muscles must adapt to the new geometry of the face and jaws.
A technically precise operation can still leave a patient with long-term symptoms if the new position creates strain elsewhere. That’s one reason post-operative care shouldn’t stop at checking incisions and radiographs.
Patient-specific factors
Biology changes outcomes. Older patients often recover sensation more slowly. Patients with pre-existing TMJ irritation may struggle more with joint adaptation. Those with chronic clenching, poor tongue posture, mouth breathing, or dysfunctional swallowing patterns may continue applying unhelpful forces to the new jaw position after surgery.
That’s also why two patients with the same procedure can have very different recoveries. One adapts quickly. Another develops persistent tightness, headaches, or a return of joint pain because the muscle system never fully reorganizes.
Why muscles and joints matter so much
The jaw doesn’t operate as a set of bones alone. It works as a functional unit involving the temporomandibular joints, masticatory muscles, tongue, airway, and cervical support system. When one part changes quickly, the rest have to catch up.
Common contributors include:
- Pre-existing TMJ stress: An irritated joint may not tolerate a new loading pattern well.
- Oral posture problems: Low tongue posture and open-mouth habits can influence stability.
- Parafunction: Clenching, grinding, and daytime jaw bracing can overload healing tissues.
- Airway strain: Patients who mouth breathe or struggle with sleep-disordered breathing may keep compensatory patterns that undermine recovery.
A jaw position can be surgically correct and still function poorly if the muscles, joints, and airway patterns around it aren’t addressed.
Risk assessment should be individualized
Patients often ask whether a side effect is “common.” That’s not the most useful question. The better question is whether you are a high-risk patient for that side effect.
A thoughtful risk discussion should include the size of the planned movement, the condition of the TM joints, age, symptom history, airway issues, and whether a rehab strategy is already in place. If your consult focuses only on where the bone will go, without equal attention to how the system will function afterward, the planning is incomplete.
The Risk of Relapse and Worsening TMJ Symptoms
One of the most misunderstood jaw surgery long term side effects is relapse, meaning the jaw drifts back toward its original position after surgery. Patients often assume that once the jaw is moved and fixed in place, the result is permanent. Bone healing helps, but it doesn’t erase muscle pull, joint remodeling, or unstable mechanics.
The available long-term data makes this risk hard to dismiss. Relapse of skeletal alignment post-orthognathic surgery affects 4% to 20% of patients long-term, with higher rates in larger surgical movements, according to this overview of long-term jaw surgery results. That same source notes that in airway-focused cases, relapse can worsen pharyngeal collapse and raise OSA severity by 5 to 10 events per hour on the apnea-hypopnea index.
Why relapse happens
Relapse is usually mechanical, not mysterious. The jaw has to hold its new position against muscular forces, joint behavior, and tissue memory. If those forces aren’t balanced, the system drifts.
A few common drivers stand out:
- Muscle pull: Old movement patterns don’t disappear just because the jaw was repositioned.
- Condylar changes: If the joint position changes unfavorably, the bite can change with it.
- Fixation limits: Hardware stabilizes the healing phase, but it can’t make weak mechanics strong.
- Large corrections: Bigger movements place greater demands on adaptation and stability.
When patients aren’t warned about relapse, they may interpret later changes as personal failure or assume they “did recovery wrong.” In reality, this is a known long-term concern that deserves active surveillance.
The missing TMJ conversation
Many patient discussions about relapse stop at appearance or bite. That misses the more important issue for many adults, which is TMJ function. A jaw that shifts can change how the joint loads, how the teeth meet, and how the muscles fire. That can set off clicking, limited opening, chewing pain, temple headaches, facial tension, and a sense that the jaw never fully relaxes.
Typical patient education often fails to connect post-surgical relapse with longer-term TMJ degeneration or to explain why conservative treatments may matter after surgery. That gap is one reason many patients end up chasing symptoms years later instead of treating the functional cause earlier.
If you’re trying to understand symptom patterns that come and go, this explanation of what causes TMJ to flare up is a helpful companion because flares are often tied to loading, muscle habits, and joint sensitivity rather than one isolated event.
A practical patient resource can also help bridge the day-to-day side of this problem. This guide to relieving jaw discomfort covers common symptom triggers and care considerations that matter when a jaw remains irritable after structural treatment.
Before watching the next clip, keep one thing in mind. A patient can have a “successful surgery” on paper and still need ongoing TMJ management in real life.
If the bite changes after surgery and the joint starts clicking or aching, don’t assume it will automatically settle with time. That pattern deserves evaluation.
Why this matters for airway patients too
Relapse isn’t only a cosmetic or orthodontic concern. In airway cases, losing forward support can reduce the benefit the patient expected from surgery. That can mean the jaw looks acceptable but sleep quality worsens again, fatigue returns, or snoring and fragmented sleep continue.
That’s why stability has to be judged by function, not just by whether the immediate post-op images looked good.
A Proactive Approach to Long-Term Recovery and Management
The worst post-surgical plan is “wait and see” when symptoms keep showing up. Long-term recovery works better when it’s managed like rehabilitation, not just follow-up. That means treating sensory changes, joint loading, muscle imbalance, breathing pattern dysfunction, and tissue irritation as active problems with active solutions.
Existing patient guidance often doesn’t make that point clearly enough. It frequently fails to connect relapse with long-term TMJ degeneration or explain how non-surgical interventions such as myofunctional therapy may help prevent relapse-related complications, as noted in this discussion of jaw surgery long-term side effect gaps. Patients need to hear a more accurate message. Post-surgical care is ongoing, not one-and-done.
What active recovery looks like
Good long-term management is targeted. Different symptoms need different tools.
- For numbness and altered sensation: sensory re-education can help the brain interpret touch more accurately again. Patients often benefit from structured exposure to light touch, temperature awareness, and movement feedback.
- For jaw stiffness and muscle guarding: physical therapy and guided mobility work can reduce protective overuse and improve opening, chewing endurance, and coordination.
- For joint overload: treatment should focus on reducing inflammation, improving mechanics, and lowering parafunctional habits such as clenching or bracing.
- For unstable muscle patterns: orofacial myofunctional therapy can retrain tongue posture, lip seal, nasal breathing, and swallow function so the new jaw position isn’t constantly being challenged.
Where regenerative care fits
When a patient has persistent TMJ pain, ligament laxity, or irritated joint tissues after surgery, regenerative options deserve a serious look. Treatments such as Platelet-Rich Fibrin (PRF) and Prolotherapy are designed to support healing rather than masking pain. They’re especially useful when the patient wants to avoid another invasive procedure or when the problem is soft tissue quality rather than a gross structural failure.
Cold laser therapy also has a role. It’s often used to calm irritated tissues, support recovery, and reduce pain sensitivity in the surrounding muscles and joints.
These options aren’t magic. They also aren’t cosmetic add-ons. In the right patient, they form part of a coherent strategy: reduce inflammation, improve tissue behavior, retrain function, and protect the surgical result.
Strength and function still matter
Many adults focus on the jaw itself and forget that general recovery principles count too. Sleep, nutrition, physical conditioning, and gradual rebuilding of capacity all influence how well the body adapts after a major procedure.
For broader rehabilitation principles, Dr. Jim's post-op strength advice is a useful read because it reinforces a point that applies here too: function returns best when recovery is progressive and intentional, not passive.
If you’re in the thick of recovery, this practical guide to jaw surgery recovery can help you think in phases rather than expecting everything to normalize on a fixed timeline.
Clinical perspective: The best long-term outcomes usually come from combining structural care with functional retraining. One without the other leaves too much unresolved.
What doesn’t work well
A few common mistakes keep patients stuck:
- Ignoring persistent bite changes because the surgery is already over.
- Assuming numbness can’t improve once the first healing window has passed.
- Treating recurring TMJ symptoms as unrelated to surgery or relapse.
- Using appliances or exercises without a diagnosis of what’s unstable.
- Jumping to revision surgery too quickly before addressing muscle and joint drivers that may be treatable conservatively.
A proactive plan doesn’t promise perfection. It gives the patient a better chance at comfort, function, and stability.
Can You Achieve Your Goals Without Surgery
This is the question more patients should ask earlier. If your goal is less pain, easier chewing, fewer headaches, a calmer TMJ, better nasal breathing, or improved sleep, surgery isn’t always the only path.
That doesn’t mean surgery is never needed. It means the indication has to be real. Many adults are told they need structural correction when the dominant problems are a mix of: inflamed joints, dysfunctional swallow patterns, chronic mouth breathing, tongue posture issues, clenching, poor cervical support, or airway strain that hasn’t been fully evaluated.
When non-surgical care makes the most sense
Conservative care deserves priority when symptoms seem driven by function more than deformity.
Examples include:
- TMJ pain with clicking or flare-ups: The problem may be joint irritation, muscle overuse, or oral posture dysfunction rather than a purely skeletal mismatch.
- Headaches and facial tension: These often improve when clenching patterns, breathing mechanics, and muscle overload are addressed directly.
- Mild to moderate bite discomfort: Some patients adapt far better once muscle balance and tongue posture improve.
- Sleep-related symptoms: Airway care may need to focus on nasal breathing, oral posture, and sleep-disordered breathing management rather than bone repositioning alone.
What root-cause treatment looks like
A non-surgical plan is strongest when it combines several disciplines instead of relying on one gadget or one exercise sheet.
That may include:
- Orofacial myofunctional therapy to retrain tongue position, lip seal, swallow, and breathing patterns.
- Regenerative therapies such as PRF or Prolotherapy when the TMJ and surrounding tissues need healing support.
- Cold laser therapy to calm irritated tissues and support tissue recovery.
- Airway-focused treatment for snoring, obstructive sleep apnea, or chronic mouth breathing.
- Behavioral and movement strategies to reduce clenching, jaw bracing, and compensatory tension.
Some patients still go on to surgery after this work. That’s fine. They often do so with a clearer diagnosis, healthier tissues, and a better support plan. Others improve enough that surgery becomes unnecessary or can be postponed.
The key decision point
If your recommendation for surgery was made without a deep look at joint health, muscle patterns, airway, and oral function, you don’t yet have the whole answer. A second opinion isn’t indecision. It’s good risk management.
For many patients, the smartest move isn’t choosing surgery quickly. It’s finding out whether the same goals can be reached with less risk first.
Essential Questions to Ask Your Oral Surgeon
A good consult should welcome detailed questions. If a provider seems irritated by them, that’s useful information by itself. Jaw surgery changes anatomy permanently, so the conversation should be specific, transparent, and focused on long-term function, not just the operation day.
Bring written questions. Don’t rely on memory in the room.
Questions that uncover real risk planning
- How will you evaluate my nerve risk before surgery? Ask how your anatomy affects the likelihood of lasting sensory change.
- What is my risk of relapse based on the size and direction of my planned movement? You want an individualized answer, not a generic reassurance.
- How are my TM joints being evaluated before surgery? If the joints are already unstable or inflamed, that should affect planning.
- What is your follow-up plan if my bite changes months later? Many long-term problems show up after routine post-op visits have ended.
Questions about rehabilitation, not just surgery
These questions matter because bone position is only part of the outcome.
- Do you recommend myofunctional therapy or physical therapy after surgery? If so, when should it begin?
- How do you monitor for relapse or joint loading problems over time?
- What symptoms should make me call you right away, even if they appear long after surgery?
- If I develop persistent TMJ pain, what conservative treatments do you use before discussing revision surgery?
- How do you coordinate care with orthodontists, sleep providers, and TMJ-focused clinicians if recovery gets complicated?
Patients do best when their surgeon can explain not only how the jaw will be moved, but how function will be protected afterward.
Questions to ask yourself
The final checklist isn’t for the surgeon. It’s for you.
- Am I pursuing surgery for a clearly defined problem?
- Have I explored conservative care that targets joints, muscles, and airway function?
- Do I understand which side effects might affect my daily life, even if the surgery is technically successful?
- Am I prepared for rehabilitation, not just surgery?
A well-informed patient doesn’t avoid surgery out of fear. A well-informed patient makes the decision with open eyes. That’s how you protect your long-term outcome.
If you're dealing with TMJ pain, facial tension, bite changes, snoring, or sleep-related breathing issues and want a careful second opinion before or after surgery, Pain and Sleep Therapy Center offers root-cause evaluation and non-surgical treatment focused on function, healing, and long-term stability.



