
You notice it in small moments first. A staircase feels oddly disorienting. Reading gets tiring faster than it should. Someone points out that your head is tilted in photos, or you realize you've been angling your face without thinking just to make the world look single again.
That pattern often sends people down the wrong path. They blame fatigue, glasses, posture, neck strain, or TMJ tension. Sometimes those are part of the picture, but sometimes the starting point is a small eye movement nerve with a very specific job. When that nerve misfires, the body starts compensating from the eyes down through the neck and jaw.
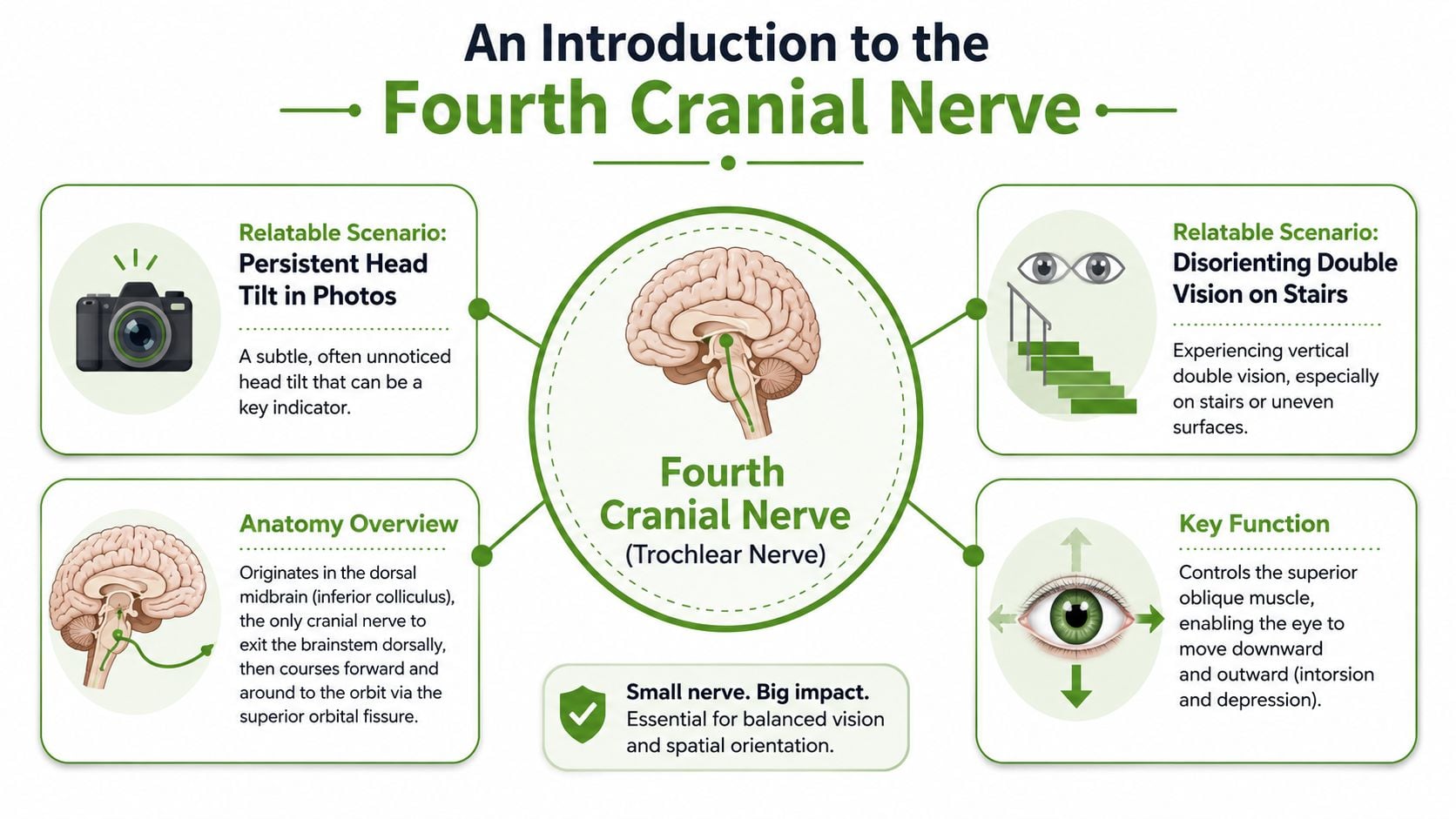
An Introduction to the Fourth Cranial Nerve
A patient with a subtle head tilt, neck tightness, and “TMJ flare-ups” after long days of reading or computer work does not always have a primary jaw or cervical problem. Sometimes the starting point is the 4th cranial nerve, also called the trochlear nerve.
This nerve supplies one extraocular muscle, the superior oblique. On paper, that sounds limited. In practice, it is one of the small control systems that keeps binocular vision steady when the eyes move down and inward, especially during reading, stair descent, and other near-work tasks below eye level.
The mechanics are easy to miss. The superior oblique works like a pulley-guided stabilizer for the eye. If the trochlear nerve is weakened by stretch, trauma, ischemia, or a central process, the two eyes stop lining up with the precision the brain expects. Patients usually do not describe that in anatomical terms. They report vertical double vision, visual fatigue, a chronic head tilt, or a sense that their neck and jaw are always trying to “find” a more comfortable position.
Why this nerve is unusually vulnerable
The trochlear nerve has several anatomical features that make it clinically important. It is the thinnest cranial nerve, it has the longest intracranial course, it exits the brainstem dorsally from the posterior midbrain, and its fibers cross before they exit. A long, slender nerve on an unusual route has more opportunities to be injured or compressed than a shorter, more protected pathway.
That matters in real patients. Minor head trauma can affect it. Microvascular injury can affect it. Brainstem and subarachnoid processes can affect it. Congenital weakness can stay hidden for years, then show up once compensation fails.
Fourth nerve palsy is also not just an ophthalmology footnote. Its annual incidence is 5.73 per 100,000 individuals, and it often presents in midlife, according to this population-based study on fourth cranial nerve palsy.
In clinic, the larger point is functional. A small ocular misalignment can recruit the whole musculoskeletal system into compensation. The patient tilts the head to reduce diplopia. The neck muscles adapt. The jaw position shifts. In some patients, especially those already dealing with bruxism, airway compromise, poor sleep, or persistent orofacial pain, that extra compensation load can worsen symptoms far outside the orbit.
That is why isolated trochlear nerve dysfunction deserves a broader diagnostic lens. The eye problem may be the trigger, but the consequences often show up in the neck, face, bite, sleep quality, and day-to-day stamina.
Recognizing the Signs of Trochlear Nerve Issues
A common presentation goes like this. A patient reports that reading has become tiring, stairs feel less reliable, and by late afternoon the neck and jaw are tight for no clear reason. They may mention intermittent double vision. Just as often, they describe feeling tilted, strained, or visually unsettled without having the language for diplopia.
What the patient usually feels
The core complaint is usually vertical diplopia, sometimes with image rotation. One image sits slightly higher than the other, and the visual world can feel subtly twisted. Patients notice this while reading, looking at a phone, eating, or stepping down from a curb. Tasks that should be automatic start demanding attention.
Symptoms tend to show up most clearly in downward gaze, especially when the eyes also have to adduct. That is why stairs, books, screens, and lap-level work trigger symptoms so often. A patient may not say, “my superior oblique is underacting.” They say, “I lose my place,” or “stairs make me hesitate.”
Fatigue matters here. Early in the day, some patients compensate well. By evening, the reserve is gone, and the visual strain spills into posture, concentration, and balance.
Why the head tilt matters
A habitual head tilt is one of the most useful bedside clues. The patient is trying to place the eyes in a position where fusion is easier and visual conflict is lower. It is an adaptation driven by the visual system.
That adaptation has consequences. A persistent tilt loads the upper cervical muscles asymmetrically. In the right patient, that can aggravate suboccipital pain, trigger temporalis and masseter overuse, and change how the jaw tracks during speech or chewing. In our clinic, an isolated eye movement disorder starts overlapping with TMJ complaints, facial pain, and poor sleep. A patient who clenches at night or already has sleep-disordered breathing has less room to compensate well.
A chronic head tilt can begin as a visual solution and end as a neck, jaw, and pain problem.
What this can look like in clinic
Some patients report obvious double vision. Others present through the side effects of compensation. They have a long-standing head posture, vague dizziness on stairs, reading fatigue, or a flare in unilateral neck and jaw tension after visually demanding work.
Children and adults with old, compensated weakness can be especially hard to spot from history alone. They may have adapted for years and only become symptomatic after illness, stress, concussion, sleep loss, or another hit to their compensatory reserve.
Later in the evaluation, a visual demonstration often helps patients connect symptom to anatomy:
Signs that should raise suspicion
A fourth nerve problem becomes more likely when these features cluster:
| Pattern | Why it matters |
|---|---|
| Vertical or diagonal double vision | Points to a vertical alignment problem rather than refractive blur |
| Worse symptoms in downgaze | Fits the superior oblique muscle's job during reading and stairs |
| Compensatory head tilt | Strong clue that the patient is trying to preserve binocular single vision |
| Symptoms during stairs or reading | Common functional triggers in daily life |
The practical mistake is to isolate each symptom into a different silo. Glasses alone do not explain the pattern. A neck diagnosis alone does not explain it either. Anxiety can amplify symptoms, but it does not produce the characteristic gaze dependence, vertical misalignment, and compensatory posture seen with trochlear nerve dysfunction.
Investigating the Common Causes of Fourth Nerve Palsy
Once the symptom pattern fits, the next question is simple and important: why did this happen? The answer shapes both urgency and treatment.
Congenital cases
Some people have a congenital fourth nerve palsy and compensate for years. They may have a subtle head tilt in childhood photos, a history of “always preferring” one head position, or long-standing visual adaptation that only becomes obvious when stress, fatigue, illness, or age reduces compensation.
These cases can be surprisingly well hidden. The patient may not complain until binocular reserve drops and the old imbalance starts breaking through.
Trauma and rapid deceleration
For acquired isolated palsy, trauma is one of the main practical categories to investigate. The trochlear nerve's long intracranial route makes it vulnerable to stretch during rapid head deceleration. Motor vehicle accidents and boxing are classic examples.
The clinical point is direct. A patient doesn't need a penetrating injury or dramatic orbital damage to injure this nerve. Sudden motion alone can be enough. That vulnerability is summarized in the NCBI review of trochlear nerve palsy, which notes that rapid deceleration trauma is the most common cause of acquired isolated fourth nerve palsy.
Practical rule: If vertical diplopia began after concussion, whiplash, a crash, or a blow to the head, keep the 4th cranial nerve high on the differential.
Microvascular and other acquired causes
In older adults, especially those with diabetes, microvascular ischemia becomes part of the discussion. Hypertension also appears in the etiologic background of fourth nerve palsy. In practice, this means the eye finding may be the first clue that a patient's broader vascular health needs attention.
A useful way to think about causes is this:
- Congenital origin: Often compensated for a long time, then decompensates.
- Traumatic injury: Often follows rapid deceleration or closed head trauma.
- Microvascular ischemia: More relevant in older adults with vascular risk factors.
- Idiopathic presentations: Sometimes the pattern is clear even when the trigger isn't.
What doesn't work is assuming every vertical diplopia case has the same cause. A congenital decompensation, a post-traumatic palsy, and a microvascular palsy may look similar at first glance, but they don't carry the same implications.
The Diagnostic Process From Symptoms to Certainty
A good diagnosis starts with pattern recognition, but it can't end there. Apparent superior oblique weakness is not the same thing as a confirmed fourth nerve palsy. That distinction matters because treatment based on the wrong label can send the patient in the wrong direction.
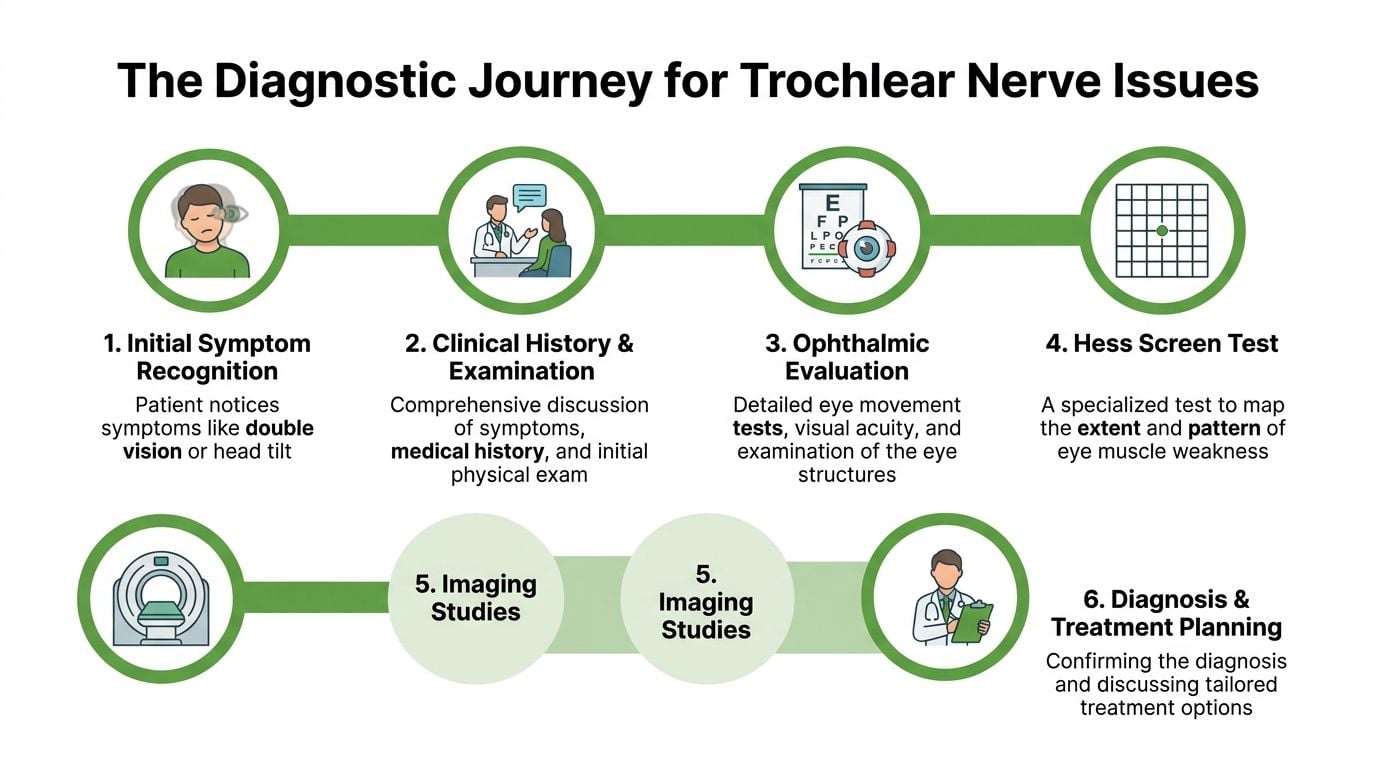
The exam is more than “follow my finger”
The in-office workup begins with history. When did the double vision start? Was it sudden or gradual? Did it follow trauma? Is it worse in downgaze? Does head tilt help? Are there vascular risk factors? Has the patient had similar symptoms before?
Then comes the eye movement exam. Clinicians look for hypertropia, torsion, gaze dependence, and the effect of head tilt. The Bielschowsky head tilt test is part of that reasoning process. Prism measurements may help quantify the deviation, and more detailed orthoptic or neuro-ophthalmic testing can map the pattern.
The key diagnostic trap
Careful specialists separate themselves from superficial diagnosis, as up to 30 to 40 percent of patients with apparent superior oblique weakness may not have a true 4th nerve palsy, but instead a mimic such as myasthenia or skew deviation, especially in patients over 50, according to Stanford Neuro-Ophthalmology's discussion of 4th nerve palsy.
That's a major number clinically. It means a plausible bedside impression is not always the final answer.
Common mimics include:
- Myasthenia gravis: Variable weakness can imitate almost any ocular motility disorder.
- Skew deviation: A central vestibular or brainstem problem can create vertical misalignment.
- Giant cell arteritis in older adults: This must stay on the radar when age and symptoms fit.
- Other cranial neuropathies: Vertical diplopia can overlap with broader ocular motor disorders, including patterns discussed in 6th nerve palsy causes.
When imaging and lab work matter
Not every patient needs the same testing, but many need more than a chairside exam. MRI may be used to rule out a structural lesion along the brainstem or nerve pathway. In older adults, especially when symptoms or systemic features raise concern, laboratory screening may be needed to help exclude inflammatory or vascular mimics.
Don't confuse a recognizable pattern with a complete diagnosis. In neuro-ophthalmology, the mimic that gets missed is often more important than the obvious diagnosis that gets named quickly.
What a root-cause approach looks like
A root-cause approach asks two questions at the same time. First, is this a fourth nerve palsy? Second, if it is, what category explains it best: congenital, traumatic, microvascular, central, or something else?
That's the difference between naming an eye movement abnormality and understanding the patient. It also prevents common mistakes, especially in older adults, in post-traumatic cases, and in patients whose neck, facial pain, or balance complaints distract from the ocular source.
Treatment Options and Recovery Outlook
Treatment starts with the cause and the timeline. A recent traumatic palsy, a likely microvascular palsy, and a long-standing congenital decompensation do not get the same plan. The practical question is simple: does this patient need time, symptom control, or a stable long-term correction?
Observation versus active symptom control
Observation is often appropriate early, especially when the pattern and history suggest a palsy that may improve on its own. That choice has a trade-off. It respects the natural recovery window, but it does not make double vision easier to live with in the meantime.
Short-term symptom control can matter just as much as the diagnosis. Patients who drive, work on screens, read for long periods, or feel off balance in busy visual environments often need help before the nerve has declared its final outcome.
A practical comparison looks like this:
| Approach | Best use | Limitation |
|---|---|---|
| Observation | Early recovery window, stable exam, likely spontaneous improvement | Symptoms may continue during recovery |
| Occlusion or temporary adaptation | Short-term suppression of diplopia | Reduces binocular vision and depth cues |
| Prism correction | Useful when the deviation can be optically offset | Less effective for marked torsion or changing alignment |
| Surgery | Persistent, stable deviation causing functional impairment | Depends on accurate diagnosis and stable measurements |
Prism glasses and when they help
Prisms help selected patients function better day to day. They do not repair the trochlear nerve. They shift the image enough to reduce the strain of trying to fuse two misaligned targets.
Temporary prisms are often the most sensible starting point while alignment is still changing. Patients weighing that option may find value in understanding stick on Fresnel prisms, especially if they want to test symptom relief before ordering permanent lenses.
Prisms also have limits. They are less satisfying in variable deviations, significant torsion, or cases where the original diagnosis is wrong. In practice, that is where patients get frustrated. The glasses are blamed, but the larger issue is usually an unstable measurement or a mimic that was never fully sorted out.
Rehabilitation and surgery
Rehabilitation has a narrow but real role. Selected patients benefit from work on fusion, visual comfort, and adaptation, particularly after the acute phase has settled. It should support the diagnosis, not substitute for it.
Surgery is usually reserved for persistent cases after the deviation has stabilized. Timing matters. Operating too early can lock in a correction for a problem that was still changing, while waiting too long can prolong disability in a patient whose pattern is clearly established.
There is also a group that falls between eye care and pain care. Some patients start with vertical diplopia, then develop jaw tension, temple pain, neck guarding, and a habitual head posture that keeps the visual world single at the expense of the musculoskeletal system. When that compensation pattern takes hold, evaluation by an orofacial pain specialist can add useful answers alongside neuro-ophthalmic management.
Recovery outlook depends on the mechanism. Some acquired palsies improve substantially with time. Others plateau and need optical correction or surgery for durable function. The right goal is not just better alignment on exam. It is comfortable binocular vision, less compensatory strain, and a treatment plan that matches the actual driver of the problem.
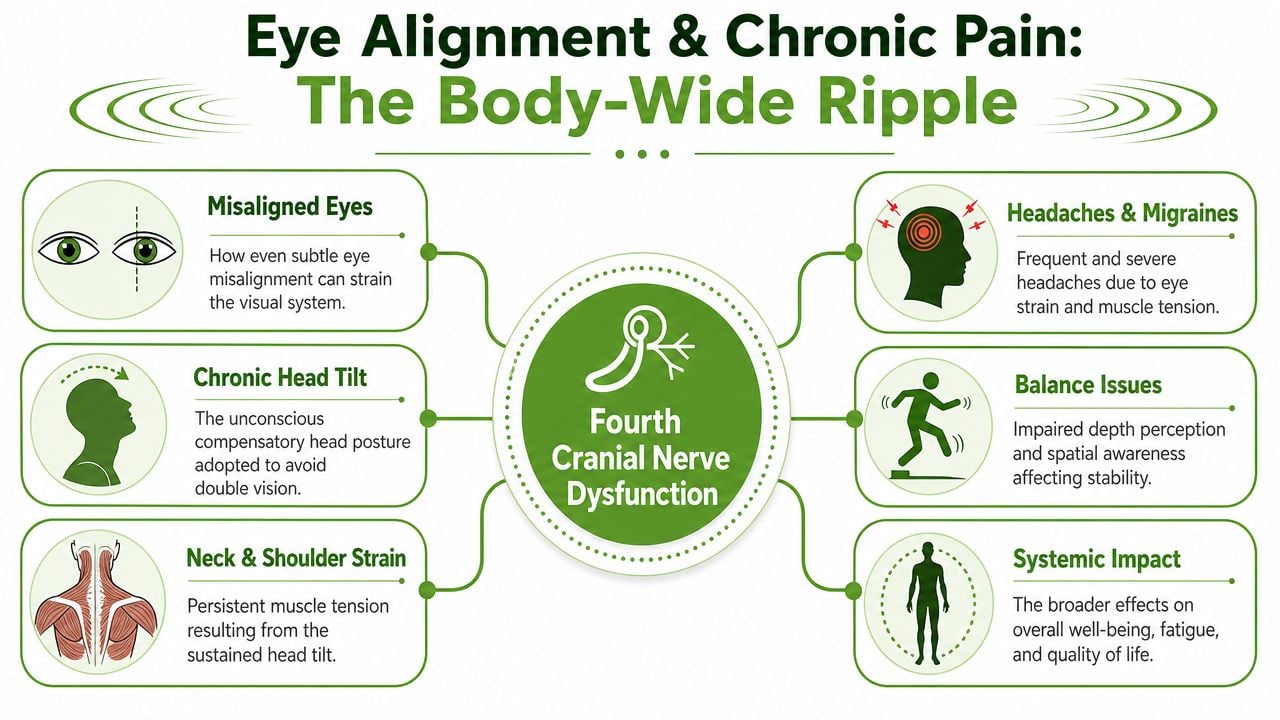
The Link Between Eye Alignment and Chronic Pain
This is the part many patients never hear. A fourth nerve palsy is not only an eye alignment problem. It can become a postural problem, a pain problem, and in some cases a sleep problem.
When the eyes don't align comfortably, the body recruits a workaround. The most common one is head tilt. If that posture is brief, it's adaptation. If it becomes constant, the neck and jaw start paying the price.
How a visual problem becomes a musculoskeletal problem
A chronic compensatory head position loads the cervical muscles asymmetrically. Over time, patients may develop neck tightness, upper trapezius overuse, suboccipital tenderness, and headaches that feel mechanical or cervicogenic. Some also clench more because the face and neck are working harder to stabilize position.
That overlap matters in clinics that see TMJ disorders and facial pain. A patient may present with jaw tension, temple pain, or unilateral neck strain, but the driver isn't always inside the joint. Sometimes the jaw is reacting to a visual alignment disorder that has changed head posture all day, every day.
Common downstream effects include:
- Neck strain: The sternocleidomastoid and upper cervical muscles work unevenly.
- Headache patterns: Visual strain and muscle guarding can coexist.
- TMJ aggravation: Jaw muscles often join the compensation pattern.
- Balance complaints: Subtle visual misalignment can make spatial orientation feel less reliable.
The sleep connection clinicians shouldn't ignore
There is also an airway angle that deserves more attention. In patients with sleep disorders, a compensatory head position adopted to reduce diplopia from CN IV palsy may worsen airway collapse during sleep, as noted in Radiopaedia's overview of the trochlear nerve.
That point is easy to underestimate. A position that helps the eyes during the day may not help the airway at night. In a patient with snoring, obstructive breathing symptoms, bruxism, or chronic fatigue, that interaction can matter.
A useful clinical habit is to ask one more question: “What has this head posture been doing to the neck, jaw, and airway?”
A broader pain framework
When chronic pain enters the picture, symptom management alone rarely solves the whole problem. Patients may explore supportive options for pain relief while the underlying diagnosis is being sorted out. For those reviewing adjunctive approaches, this guide on explore using CBD for chronic pain gives a practical overview of one commonly discussed option. It's not a diagnosis, and it's not a substitute for targeted care, but patients often ask about it.
In the same way, facial pain symptoms shouldn't automatically be treated as isolated dental or muscular issues. Persistent unilateral facial discomfort, atypical headache patterns, or neuralgic symptoms may justify a closer look at related pathways and differential diagnoses such as facial neuralgia pain relief.
What works best is integrated thinking. If the eyes are misaligned, the neck compensates. If the neck compensates, the jaw may follow. If the head posture persists into rest and sleep, the airway may be affected too. Treating only the last link in that chain often leaves the first one untouched.
Restoring Balance and Clarity
The 4th cranial nerve has one job, but when that job breaks down the effects spread quickly. Patients may notice double vision, a head tilt, trouble on stairs, or reading fatigue. Over time, those visual adaptations can feed neck pain, headache patterns, jaw tension, and even sleep-related issues.
The biggest clinical mistake is oversimplification. Not every apparent superior oblique weakness is a true fourth nerve palsy. Not every fourth nerve palsy has the same cause. And not every patient with chronic facial or cervical strain started with a local pain disorder.
The best outcomes usually come from accurate diagnosis first, then a treatment plan that matches the cause, the recovery phase, and the patient's functional burden. Sometimes that means watchful waiting. Sometimes it means prisms. Sometimes it means surgery. Often it means recognizing that the eyes, neck, jaw, and airway aren't separate systems in real life.
When the diagnosis is correct, treatment gets simpler. When the root cause is missed, compensation tends to spread.
If you're dealing with double vision, a chronic head tilt, TMJ strain, facial pain, or sleep-related symptoms that don't seem to fit neatly into one specialty, Pain and Sleep Therapy Center takes a root-cause approach that looks at how eye alignment, musculoskeletal compensation, and airway function can interact. Their team evaluates the full pattern so treatment isn't aimed only at the loudest symptom.



