
If you're reading about oral surgery for sleep apnea, you're probably already tired of being tired. Maybe you snore hard enough to wake your partner, maybe you rip off your CPAP mask halfway through the night, or maybe you've done “all the right things” and still wake up foggy, dry-mouthed, and worn down.
That frustration exists. But surgery shouldn't be treated like the automatic next step just because CPAP has been difficult or your symptoms are still hanging on. Oral surgery for sleep apnea is a serious tool, not a default solution. In the right patient, it can change a life. In the wrong patient, it can mean recovery, expense, and risk without solving the underlying problem.
Is Surgery the Answer for Your Sleep Apnea
Patients generally don't need to begin in an operating room. They need a careful answer to a more important question: why is the airway collapsing in the first place?
For some people, the issue is strongly anatomical. The jaws may sit too far back, the tongue base may crowd the airway, or the soft palate may collapse in a way that makes non-surgical treatment harder. In those cases, surgery may deserve real consideration. For others, the better path may be a custom oral appliance, myofunctional therapy, breathing retraining, positional strategies, or a combination of treatments.
When surgery belongs in the conversation
Surgery makes the most sense when a patient has already had a proper evaluation, has a clear structural cause, and either hasn't responded to conservative care or can't tolerate it enough to get meaningful benefit.
That distinction matters. A person who “failed CPAP” because the mask fit was poor is different from someone with severe obstruction tied to jaw position. A person with facial pain or TMJ dysfunction also needs extra caution, because aggressive intervention around the jaws can create new problems even when the airway goal is sound.
Clinical reality: The best treatment is the one that fixes the airway with the least disruption to the rest of your health, bite, comfort, and daily life.
A better way to think about the decision
Instead of asking, “Which surgery should I get?” ask these questions first:
- Where is the airway collapsing? At the soft palate, tongue base, multiple levels, or because of skeletal structure?
- How severe is the sleep apnea? Mild, moderate, and severe cases don't all deserve the same plan.
- What have you already tried well enough to judge? Not every abandoned treatment was given a fair trial.
- What else is going on? TMJ pain, headaches, bite instability, nasal breathing problems, and tongue function all change the decision.
The right plan isn't always the most aggressive one. Often it's the most precise one.
Mapping the Surgical Landscape Key Procedures Explained
The names can sound intimidating, but most sleep apnea surgeries aim to do one of two things. They either remove or tighten tissue that blocks airflow, or they reposition structures so the airway has more room.
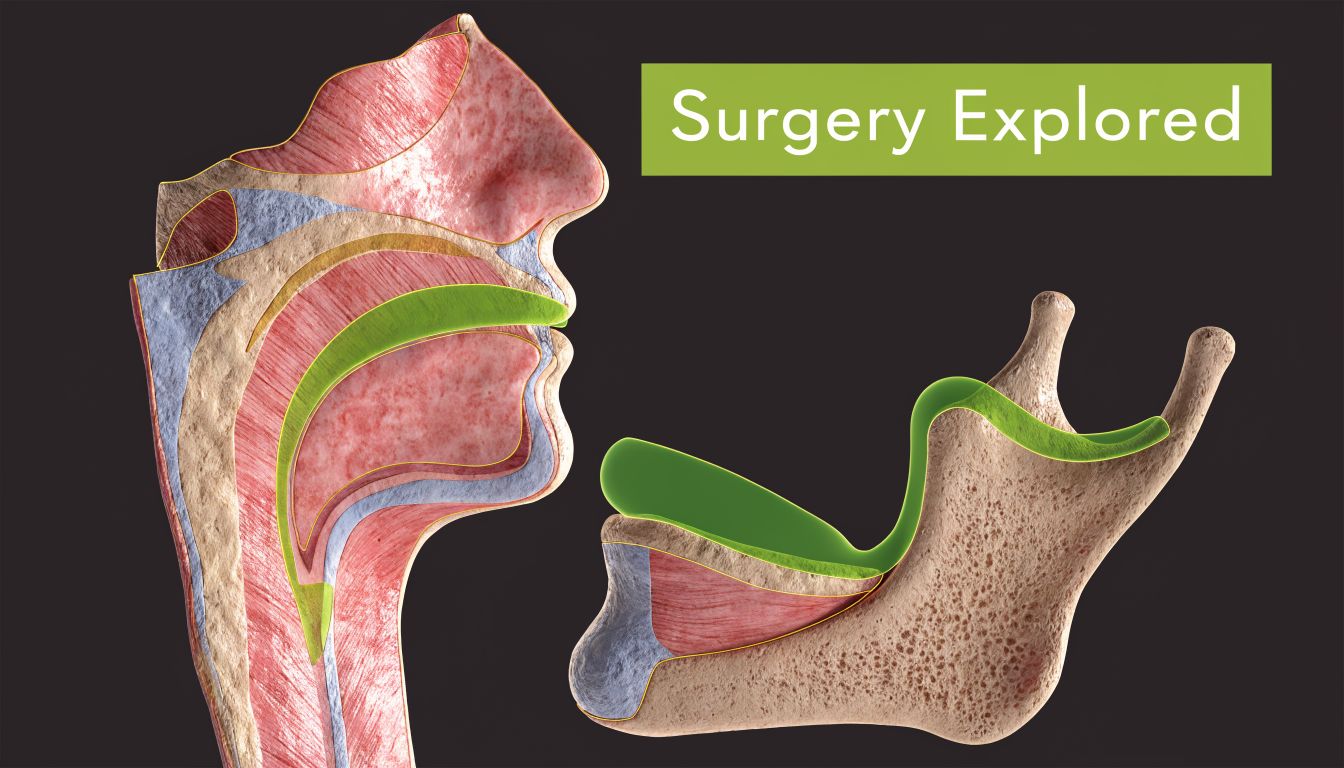
Soft tissue surgery
A common example is uvulopalatopharyngoplasty, often shortened to UPPP. This surgery targets tissue in the back of the throat, usually around the soft palate and uvula, to create more space.
Think of it as trimming and reshaping the back curtain of the airway. That can help in selected patients, especially when the soft palate is a major site of collapse. But it doesn't move the tongue base forward, and it doesn't correct a recessed jaw. That's why it can fall short when obstruction happens lower down or at multiple levels.
Tongue-related procedures
Another category includes procedures aimed at the tongue base, such as genioglossus advancement. The idea is to bring forward the attachment of the tongue muscle so the tongue is less likely to fall backward during sleep.
This is more targeted than broad palate surgery. It can be useful when imaging or sleep endoscopy shows tongue-base collapse. But by itself, it may not be enough when the airway problem involves several structures at once.
Jaw advancement surgery
Maxillomandibular advancement, or MMA, moves both the upper jaw and lower jaw forward. In plain terms, the surgeon repositions the facial skeleton to create a wider airway behind the tongue and soft palate.
This is the most structurally powerful option in oral surgery for sleep apnea. A source discussing MMA describes it as advancing both jaws 8 to 12 mm and enlarging the pharyngeal airway space by up to 100%, with planning guided by 3D volumetric CT scans and use often reserved for severe cases with specific skeletal patterns and AHI greater than 40 (MMA surgical overview).
Here's a simple comparison:
| Procedure | Main target | Best fit |
|---|---|---|
| UPPP | Soft palate and throat tissue | Palatal obstruction |
| Genioglossus advancement | Tongue attachment | Tongue-base collapse |
| MMA | Entire jaw framework and airway space | Severe OSA with skeletal contribution |
If you're trying to understand how jaw procedures fit into broader facial surgery planning, this overview of jaw realignment surgery options helps patients connect airway concerns with bite and skeletal structure. For Spanish-speaking patients comparing regional specialists, this page on cirugía maxilofacial en Katy, TX gives useful background on orthognathic treatment.
Surgery changes anatomy. That can be exactly what's needed when anatomy is the main driver. It can also be too much treatment when the problem is better handled with a device, therapy, or coordinated care.
Weighing the Outcomes Surgical Success Rates and Risks
The first thing patients ask is fair: does it work?
The harder question is better: what does “work” mean? In sleep medicine, success usually doesn't mean “you had surgery.” It means your apnea burden dropped meaningfully and your sleep, oxygenation, and symptoms improved in a lasting way.

What the strongest data supports
Among surgical options, MMA has some of the best outcome data. A meta-analysis reported an 86% success rate using the definition of at least a 50% reduction in AHI and a final AHI below 20, with a 43.2% cure rate defined as AHI below 5. The same source reported major complications in 1.0% of cases (meta-analysis on MMA outcomes and complications).
That doesn't mean every patient gets cured. It means the right candidate has a strong chance of substantial improvement.
A long-term view matters too. Some procedures look good early and disappoint later. MMA stands out because outcomes have shown durability in well-selected patients, especially when the underlying anatomy points clearly toward jaw advancement as the main fix.
Why older procedures often disappoint
Many people have heard of soft tissue procedures first because they've been around longer and are commonly discussed. The problem is that removing tissue from one area can miss the bigger picture.
If the tongue, soft palate, and jaw position all contribute to collapse, a single-level surgery may leave major obstruction untouched. That's one reason many patients need a more thorough workup before anyone talks about cutting tissue.
Risk-benefit rule: The bigger the surgery, the stronger the reason should be. The more limited the expected benefit, the harder it is to justify a permanent procedure.
Risks patients should discuss plainly
Every surgery carries trade-offs. With sleep apnea surgery, those can include discomfort, swelling, recovery limits, temporary numbness or altered sensation, bite changes, and the possibility that symptoms improve only partially.
For jaw surgery in particular, patients should also talk through chewing changes, facial sensation, healing time, and how the procedure may interact with existing TMJ issues. If you want a practical example of how dentists explain complications and prevention in another surgical context, The Dental Retreat's implant failure advice is a good model for the kind of honest risk discussion patients deserve before any irreversible procedure. Patients considering skeletal surgery should also review longer-view concerns such as jaw surgery long-term side effects.
A good consultation doesn't sell surgery. It shows where surgery is likely to help, where it may not, and what you're giving up to pursue it.
Powerful Alternatives to Oral Surgery to Consider First
Most patients should exhaust conservative, targeted options before they commit to oral surgery for sleep apnea. That's not because surgery never works. It's because many people can improve substantially without changing their anatomy permanently.
The most effective non-surgical path often isn't one single therapy. It's a coordinated plan that addresses airway mechanics, tongue posture, nasal breathing, sleep position, and nightly adherence.

Oral appliances often outperform CPAP in real life adherence
Oral appliance therapy, especially a custom mandibular advancement device, deserves far more attention than it usually gets. These devices hold the lower jaw forward during sleep, which can help keep the airway open without a mask or hose.
One source reports about 90% compliance for oral appliance therapy compared with 50% for CPAP, and notes that around 70% of people with OSA have an AHI reduction of more than 50% with mandibular advancement device therapy. The same source states that for roughly one-third of patients, MAD therapy completely resolves OSA symptoms, and that about 48% reach complete resolution or maintain an AHI below 5 (oral appliance therapy effectiveness and compliance).
Those numbers matter because the best therapy on paper still fails if it sits on the nightstand. A treatment you use every night often beats one you can't tolerate.
Myofunctional therapy treats function, not just airflow
Orofacial myofunctional therapy is often best understood as physical therapy for the tongue, lips, cheeks, and swallowing pattern. It aims to improve oral posture, support nasal breathing, and reduce the dysfunctional habits that allow airway collapse to persist.
A cited content gap source notes that studies show myofunctional therapy can reduce AHI by 50% in adults and children as an adjunct or standalone approach (discussion of conservative options and myofunctional therapy). That doesn't make it a replacement for every severe case. It does make it a serious option that shouldn't be skipped just because surgery sounds more definitive.
Patients often underestimate how much tongue posture and mouth breathing matter. If the tongue lives low in the mouth and the lips stay open at night, the airway environment stays unstable. Therapy works on those mechanics directly.
Breathing retraining and habit correction
Breathing methods such as Buteyko breathing don't “cure” every airway problem, but they can play an important role in reducing dysfunctional mouth breathing and improving carbon dioxide tolerance, nasal use, and sleep quality.
These approaches are most useful when they aren't treated like internet hacks. They need to be integrated into a broader plan that includes diagnosis, airway assessment, and follow-through.
Here are the non-surgical options worth discussing before surgery:
- Custom oral appliance therapy: Best for patients who can't tolerate CPAP or want a more portable, less intrusive option.
- Myofunctional therapy: Useful when tongue posture, mouth breathing, swallowing pattern, or oral muscle weakness contribute to collapse.
- Breathing retraining: Helpful when chronic mouth breathing and poor nasal habits worsen nighttime symptoms.
- Lifestyle and positional strategies: Sometimes simple changes reduce symptom burden enough to avoid escalation.
Surgery is usually a late-stage decision. Function-first care often reveals that the airway can improve without cutting tissue or moving bone.
If you're exploring dental approaches that may help restore energy with dental sleep treatment, it's worth looking at how oral appliances fit into a broader sleep apnea plan rather than viewing them as a lesser substitute for surgery.
The Road to a Decision Your Pre-Treatment Evaluation
No one should approve surgery for sleep apnea based on snoring alone, a tired feeling, or a quick glance at the throat. A real decision starts with a workup that shows how severe the problem is and where the airway is failing.
Start with objective sleep data
A sleep study gives the baseline. That may be an in-lab polysomnogram or an appropriate home study, depending on the case. Without that starting point, it's impossible to judge severity or measure whether treatment worked.
If you're early in the process, a guide to diagnosing sleep apnea at home can help you understand what home testing can and can't tell you.
Then identify the collapse pattern
“Sleep apnea” is a diagnosis, not a complete explanation. Two patients can have similar symptoms and very different anatomy.
A strong pre-treatment evaluation may include:
- Sleep study review to establish the apnea pattern and burden.
- Airway examination of the nose, palate, tongue, and jaw relationships.
- Bite and TMJ assessment to flag issues that could affect oral appliance use or make surgery riskier.
- Imaging or endoscopic evaluation when anatomy needs a closer look.
One of the most useful tools before surgery is drug-induced sleep endoscopy, often called DISE. It lets the clinician observe where the airway collapses during a sleep-like state instead of guessing from awake anatomy alone.
A short visual overview can make that process easier to understand:
Questions your evaluation should answer
A worthwhile consultation should leave you with specific answers, not vague reassurance.
- Is my obstruction mainly nasal, palatal, tongue-based, skeletal, or multilevel?
- Am I dealing with a problem that could respond to a custom device or therapy first?
- Would surgery address the main cause, or just one part of it?
- How might treatment affect my bite, jaw comfort, and daytime function?
A diagnosis is only the beginning. The treatment plan becomes reliable when the anatomy, function, symptoms, and sleep data all point in the same direction.
Finding Your Path Choosing a Treatment and Your Team
The best treatment plan usually comes from a team, not a single opinion. Sleep physicians, dental sleep medicine clinicians, ENTs, oral surgeons, myofunctional therapists, and pediatric providers often see different parts of the same problem. When they compare notes, patients get a safer and more accurate recommendation.
That matters even more when symptoms overlap with TMJ pain, facial tension, chronic mouth breathing, bite concerns, or pediatric airway issues. A surgeon may be excellent at moving bone, but that doesn't mean surgery is the best first answer.
Questions worth bringing to your consultation
Bring a written list. Patients remember less than they think once the appointment gets moving.
- Based on my testing, where is my airway collapsing most?
- What non-surgical options still deserve a proper trial in my case?
- If surgery is recommended, why this operation and not another one?
- What happens if the procedure improves my AHI but doesn't fully resolve my symptoms?
- How will this affect my bite, jaw comfort, and long-term function?
Pediatric decisions need extra restraint
In children, a conservative and interdisciplinary mindset matters even more. One source notes that 1% to 5% of children have OSA, and for tongue-tie related issues, laser frenectomy combined with myofunctional therapy can yield 85% improvement in breathing and a 62% long-term reduction in AHI, helping some families avoid more aggressive approaches (pediatric sleep apnea and tongue-tie discussion).
That doesn't mean every child needs frenectomy. It means children deserve evaluation for function, growth, tongue mobility, and breathing patterns before anyone reaches for adult-style surgical logic.
Choose the team that can justify restraint when restraint is the right call. That's often the clearest sign you're in the right hands.
Frequently Asked Questions About Sleep Apnea Surgery
Is oral surgery for sleep apnea usually the first treatment?
No. For most patients, it shouldn't be. Surgery is usually considered after a proper diagnosis and after non-surgical treatments such as CPAP, oral appliance therapy, myofunctional therapy, breathing retraining, or combined care have been evaluated.
How long is recovery?
Recovery depends on the procedure. Soft tissue surgeries and jaw surgeries don't feel the same and don't heal on the same timeline. Your surgeon should give you a procedure-specific recovery plan covering diet, swelling, activity, pain control, and follow-up sleep testing.
Will insurance cover it?
Sometimes, especially when the procedure is medically necessary and conservative treatment has been documented. Coverage varies widely, so ask for a preauthorization process, diagnosis coding details, and written estimates before you schedule anything.
How do I find the right specialist?
Look for someone who doesn't jump straight to surgery. A good clinician should review sleep testing, examine airway anatomy, discuss conservative options seriously, and explain risks in plain language. If your case is complex, ask whether your care involves coordinated input from sleep medicine, dental sleep medicine, ENT, surgery, and therapy providers.
Can surgery completely cure sleep apnea?
Sometimes, but not always. The stronger question is whether it will improve your breathing enough, safely enough, to justify the trade-offs. That's why candidacy and diagnosis matter so much.
If you're trying to decide whether surgery, an oral appliance, myofunctional therapy, or a more complete airway evaluation makes sense, Pain and Sleep Therapy Center offers a root-cause approach for sleep-disordered breathing, TMJ issues, and facial pain. Their interdisciplinary team helps adults and children sort out what isn't working, what should be tried first, and when a surgical referral is appropriate.



