
Some readers arrive here after a pediatric visit that left them with more questions than answers. Their baby clicks while nursing, slips off the breast, or feeds for a long time but still seems unsatisfied. Others are adults who've spent years chasing separate problems like jaw tension, poor sleep, mouth breathing, neck tightness, headaches, or speech frustration, without anyone asking whether a small band of tissue under the tongue might be part of the pattern.
A restrictive tongue tie or lip tie can be easy to miss because the symptoms don't always look dramatic. They often look ordinary. Feeding struggles. Crowded teeth. Snoring. A tongue that never seems to rest on the palate. A child who compensates. An adult who has adapted for so long that the compensation feels normal.
A laser frenectomy procedure can be an important turning point, but it helps to see it for what it is. It isn't a magic reset. It's a precise release of tethered tissue that creates the possibility for better movement, better posture, and better function. What happens after that release often determines whether the change becomes lasting relief.
The Hidden Cause of Common Health Struggles
A baby can pass a routine exam, gain some weight, and still turn every feeding into a struggle. The latch slips. Nursing hurts. Feedings run long, then start again before anyone has recovered. Parents are often told to adjust position, try a different bottle, or wait for maturity to solve it.
Older children and adults usually present differently. The complaint may be open-mouth posture, restless sleep, speech effort, jaw tension, clenching, or a constant sense that the mouth and throat are working harder than they should. Those problems can look unrelated on the surface.
In some patients, the common thread is restricted oral tissue.
When the tongue or lip cannot move through a normal range, the body builds workarounds. Feeding mechanics change first for many infants. Later, the pattern can show up in swallowing, tongue rest posture, nasal breathing, speech clarity, and muscle strain through the jaw, face, and neck. If parents are trying to sort out what is expected development versus a sign that something is off, this milestone guide for new parents can help frame the bigger picture.
When the symptom is a compensation
Many families and adult patients spend months, sometimes years, treating the downstream problem. They rotate bottles, start speech exercises, use night guards, work on posture, or pursue sleep support. Those steps may still have value, but progress often stalls if the tongue remains tethered and cannot learn a better pattern.
That is why evaluation has to focus on function, not appearance alone. A small frenulum can cause very little trouble in one patient and a great deal in another. The difference is how that tissue affects latch, tongue elevation, seal, swallowing, resting posture, and breathing behavior over time. If you want a broader view of how those patterns can show up beyond infancy, this overview of tongue-tie complications is a helpful reference.
Restricted tissue changes movement. Movement shapes development.
That distinction matters because a laser frenectomy procedure works best as the start of functional rehabilitation, not the end of it. Releasing tissue can create access to better tongue mobility, but lasting improvement in feeding, speech, sleep, and breathing usually depends on what the patient does with that new range of motion. In myofunctional practice, that means pairing the release with guided exercises and orofacial myofunctional therapy so the mouth, tongue, and airway can adopt healthier patterns instead of returning to old compensations.
Understanding Tongue Ties and Lip Ties
A frenulum is a normal band of tissue. Everyone has one under the tongue and one connecting the lip to the gums. The problem isn't the existence of the tissue. The problem is when that tissue is short, thick, tight, or positioned in a way that limits movement.
Imagine an anchor line that's too short. The boat can move, but not freely. It compensates instead.
A tongue tie involves the lingual frenulum under the tongue. A lip tie involves the labial frenulum under the lip. Either can restrict motion, but the functional consequences differ by age and by the patient's overall oral posture and breathing pattern.
What restriction looks like in daily life
In infants, the issue often shows up first during feeding. The tongue may not lift, cup, or extend well enough to create an efficient latch. The result can be frustrating for both baby and parent.
In children, the signs broaden:
- Speech strain: Some sounds may be harder to produce cleanly when the tongue can't lift or move with enough range.
- Messy mechanics: Chewing, swallowing, and clearing food from the mouth can look inefficient.
- Oral posture changes: A low resting tongue posture can encourage mouth-open posture over time.
Adults may not think of a tie at all. They may report jaw tightness, overworked neck muscles, tongue fatigue, restless sleep, or a lifetime of feeling that the tongue “doesn't fit” comfortably in the mouth.
For parents unsure what to look for early on, this guide on how to tell if baby has tongue tie can help you recognize common functional signs.
Why diagnosis should focus on function
A restrictive frenulum doesn't matter because it “looks tight.” It matters when it interferes with what the tongue or lip needs to do.
That means a useful evaluation asks questions like these:
| Function | What clinicians look for |
|---|---|
| Feeding | Can the baby latch, transfer milk, and maintain suction comfortably? |
| Speech | Does tongue restriction appear to limit specific movements needed for articulation? |
| Breathing | Is the tongue resting low, encouraging mouth breathing instead of nasal breathing? |
| Swallowing | Does the patient thrust, compensate, or recruit extra facial muscles? |
| Jaw comfort | Do the jaw and neck muscles appear to be overworking to compensate for poor tongue mobility? |
Different ages, different goals
The reason for treatment changes with age.
For a newborn, the priority may be breastfeeding comfort and efficiency. For a school-age child, it may be speech clarity, oral rest posture, or dental development. For an adult, it may be part of a larger plan involving TMJ symptoms, sleep-disordered breathing, and muscle tension.
Clinical perspective: The same tissue restriction can produce very different symptoms in different patients. That's why the exam should never stop at “yes or no” for a tie.
A frenectomy makes sense when release of the tissue is likely to improve function, and when the patient or family is prepared to support the healing and retraining that follow.
Why a Laser Frenectomy Is the Modern Solution
A common scenario in my practice is a parent who says, “We were told the tie was released, but feeding still feels hard,” or an adult who expected a quick procedure to solve years of mouth breathing, tongue tension, or jaw fatigue. In many of those cases, the issue is not the idea of treatment. It is the treatment plan. A laser frenectomy works best as the start of functional change, not as an isolated procedure.
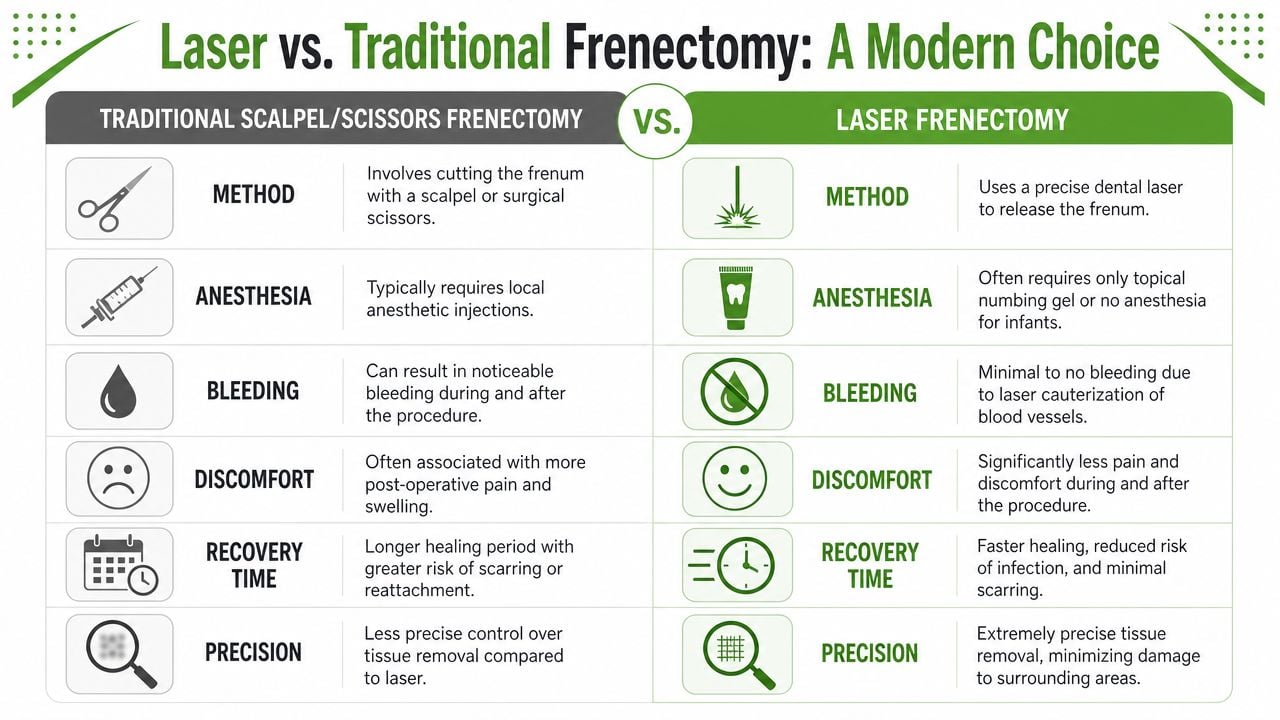
Traditional frenectomy methods use scissors or a scalpel to cut restrictive tissue. They can release the tie, but they often create more bleeding, more swelling, and a less controlled surgical field. A laser approach gives the clinician better visibility and more precise tissue management, which usually makes the procedure easier on the patient and easier to guide carefully.
A modern laser frenectomy procedure typically uses a dental soft-tissue laser, often a diode laser. The practical advantage is straightforward. The laser releases the tissue while helping control small vessels at the same time, so the site stays cleaner and the release can be performed with less disruption to surrounding tissue.
Laser versus traditional methods
Patients usually care about four things:
- Bleeding and visibility: Laser treatment often produces a cleaner field, which helps the clinician see the fibers being released and work with more control.
- Tissue response: Many patients have less swelling and irritation than they expect from oral surgery.
- Appointment experience: These releases are often brief and can frequently be done with topical or local anesthesia, depending on age and case details.
- Recovery management: There is usually less immediate wound care than with older methods, although aftercare exercises still matter.
Those advantages are meaningful, but they should be framed truthfully. Laser technology improves the procedure. It does not replace good judgment, careful diagnosis, or follow-through after the release.
Why the technology changes outcomes
Laser treatment's value is not that it feels newer. It is that it can create a precise release with less procedural noise around it. That matters because the goal is not merely to remove tissue. The goal is to free movement that the patient can then use for better latch, better oral rest posture, clearer speech movements, more efficient swallowing, and in some cases healthier nasal breathing during sleep.
That is where many treatment plans fall short. If the tongue has spent months or years compensating, the nervous system and muscles do not automatically switch to healthier patterns the moment the restriction is released. The patient still needs to learn how to rest, lift, seal, swallow, and breathe differently.
Here's a short video for patients who want to see the approach in context.
Trade-offs that patients should understand
Laser is a strong tool, not a complete treatment plan. In a straightforward infant case, a release may quickly improve latch and maternal comfort. In an older child or adult with long-standing compensation, body tension, speech habits, or sleep-related concerns, the procedure is only one part of care.
For lasting success, I look closely at whether orofacial myofunctional therapy (OMT) is part of the plan. OMT helps patients retrain tongue posture, lip seal, nasal breathing, chewing, and swallowing after the release. Without that retraining, patients can keep using the same dysfunctional patterns with newly available mobility.
For families comparing providers, the better questions are practical ones. How is function being assessed before treatment? How is aftercare taught? Is OMT recommended before and after the release when appropriate? Those answers often have more impact on breathing, sleeping, speaking, and long-term comfort than the laser device alone.
The Laser Frenectomy Procedure Step by Step
Anxiety drops when patients know what the appointment will feel like. Patients often expect something bigger than what a laser release usually is. In reality, the procedure is brief, controlled, and focused on a small area of tissue.
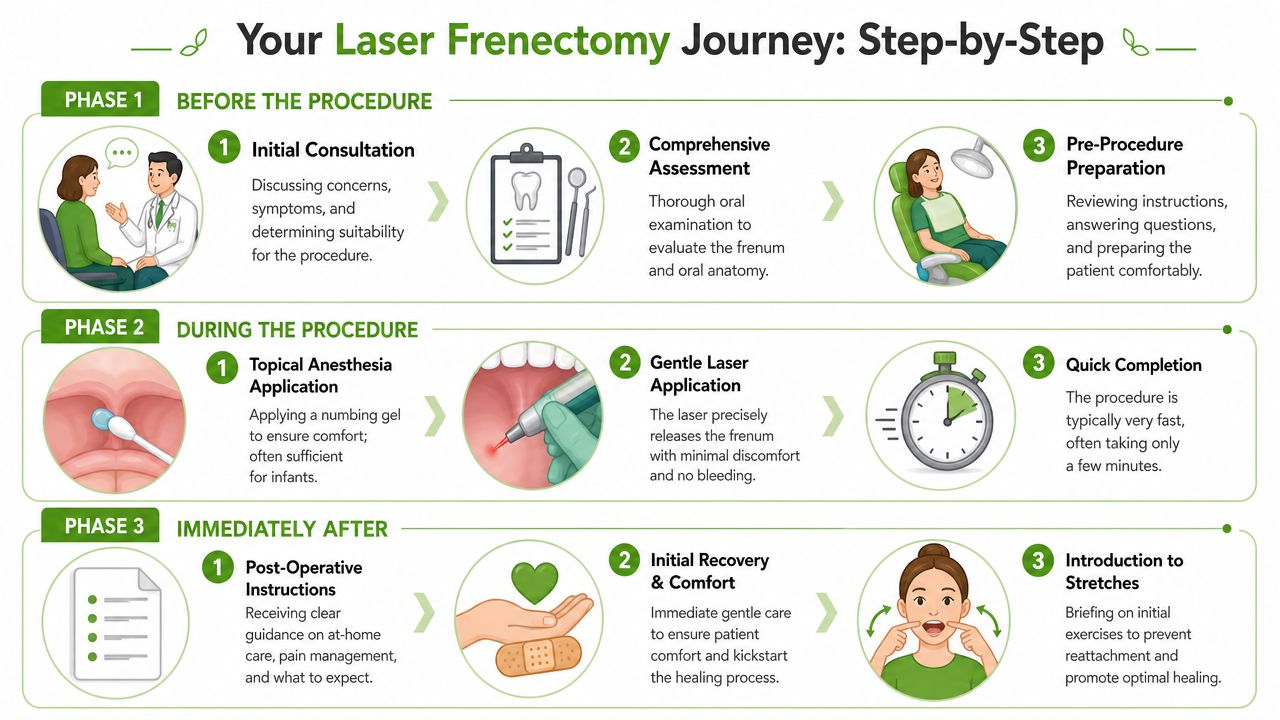
The day itself usually unfolds in three phases: evaluation and preparation, the release, then guided aftercare.
Before the release
The visit starts with a focused examination. The clinician looks at anatomy, but also at how the tongue and lips function during rest, movement, swallowing, speech, or feeding. For infants, that may include a feeding history. For older children and adults, it often includes questions about breathing, oral posture, tension, and compensation patterns.
Preparation is typically simple. Many laser releases can be done with topical numbing gel. Infants often tolerate the process well because the release is quick and there's no scalpel or suturing involved.
The calmest procedures tend to happen when the family knows the plan, understands the reason for the release, and is prepared for the exercises that follow.
During the procedure
Once the area is numb, the laser is used to release the restrictive frenulum with controlled, localized energy. The exact feel varies by patient, but it is typically not described as a dramatic event. Patients usually notice how fast it is.
What parents and adult patients can expect:
- Positioning: The tissue is gently exposed so the provider can see clearly.
- Precise release: The laser frees the restriction while minimizing disruption to nearby tissue.
- Immediate check: Tongue or lip mobility is reassessed right away.
The goal isn't to create a large wound. The goal is to release the tether thoroughly enough to allow the needed movement.
Right after the appointment
The first conversation after the release matters as much as the procedure itself. Patients need to know how to care for the site and what normal healing looks like.
Most aftercare plans include:
- Wound management: Gentle stretches or lifts to reduce the chance of the tissue healing back in a restrictive way.
- Comfort support: Guidance on soothing the area and managing expected tenderness.
- Function practice: Age-appropriate exercises that begin teaching the tongue or lip how to use its new mobility.
For some families, that starts immediately with feeding support. For older children and adults, it often includes a more structured plan for tongue posture, swallowing, and breathing mechanics.
What doesn't help
Passive observation rarely gives the best result. If the release is done well but the tongue stays in the same low, compensated pattern, patients may feel disappointed because the anatomy changed but the habit did not.
That's why a careful clinic doesn't stop at “procedure completed.” The release is just one event inside a larger treatment process.
Recovery and The Key to Lasting Success
A parent may notice a better latch on day one. An adult may feel more tongue freedom as soon as the numbness wears off. Those early changes are encouraging, but they are not the endpoint.
Long-term success depends on what the tongue, lips, jaw, and airway do during healing and after it.
A restricted tongue learns workarounds. After release, those patterns do not disappear on their own. The tongue may still rest low. Swallowing may still recruit the lips or chin. Mouth breathing may still be the default. If those habits stay in place, patients can miss much of the benefit the procedure was meant to create.
Orofacial myofunctional therapy, or OMT, addresses that gap. It helps convert new mobility into useful function for breathing, sleeping, feeding, and speech.
Why exercises matter after the release
The laser release creates access to movement. Therapy and home care help the body use that movement well and keep it during healing.
Without guided follow-through, I often see the same problem repeat. The anatomy improved, but the function stayed stuck in an older pattern. That is why aftercare is not a side note. It is part of the treatment itself.
What OMT actually works on
Myofunctional therapy is more than stretching the site. A good plan targets the habits that developed around the restriction and the new skills needed after release.
- Tongue posture: Training the tongue to rest against the palate instead of sitting low in the mouth
- Swallow pattern: Reducing tongue thrust and excess facial muscle use during swallowing
- Lip seal: Supporting a comfortable closed-mouth posture when appropriate
- Breathing mechanics: Reinforcing nasal breathing and reducing chronic mouth-breathing habits
- Coordination: Building controlled movement without strain
Patients who want a clearer picture of the home program can review these frenectomy exercises as part of recovery.
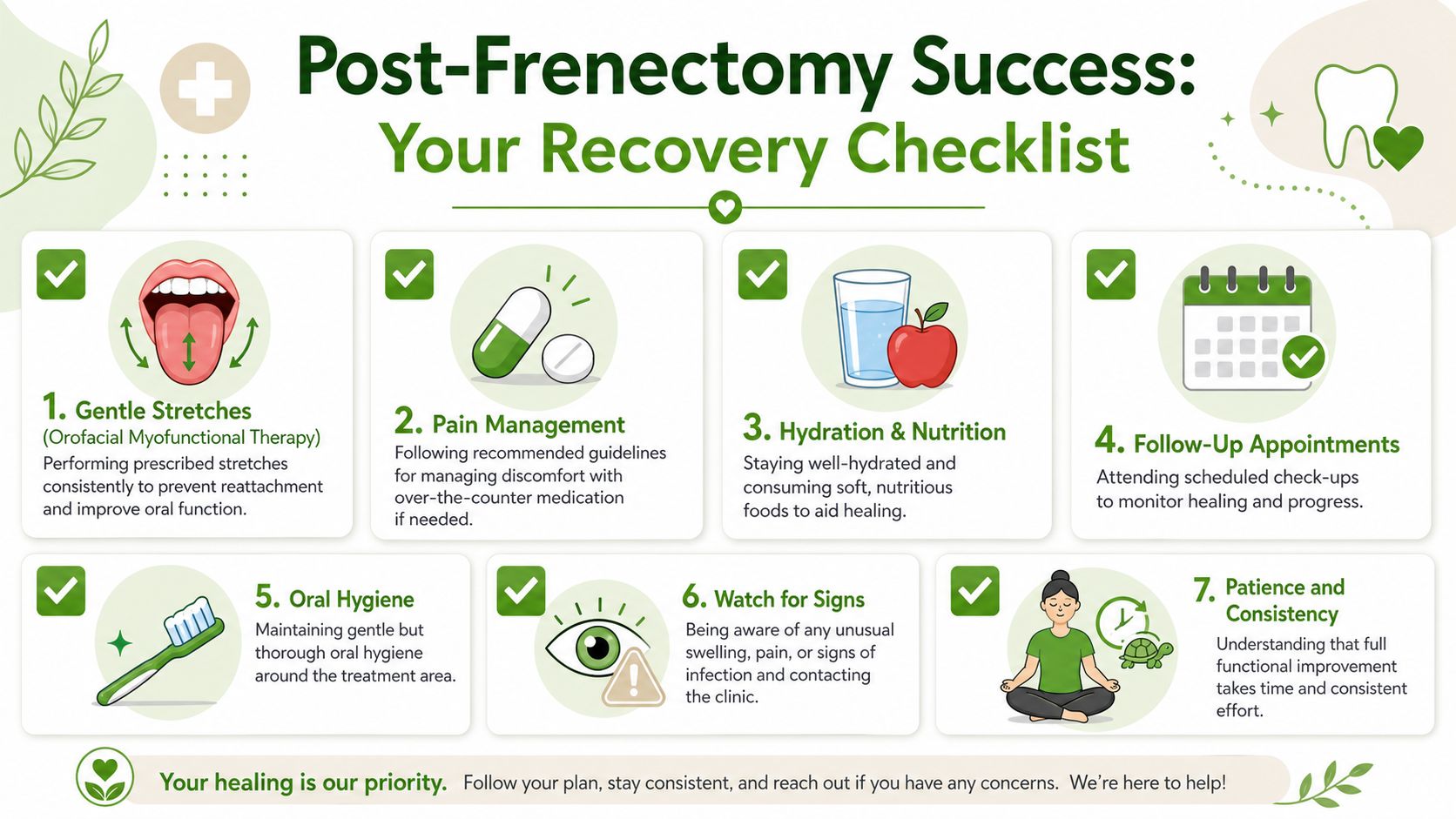
What recovery usually requires from the patient
Recovery is active, especially in the first days and weeks. Patients and parents usually do best when they know exactly what their role is and why it matters.
| Recovery element | Why it matters |
|---|---|
| Wound stretches | Helps reduce the chance of the released tissue healing back together in a restrictive pattern |
| Functional drills | Teaches the tongue how to lift, move side to side, and coordinate more effectively |
| Breathing work | Supports nasal breathing and steadier oral rest posture |
| Follow-up visits | Lets the care team identify guarding, compensation, or early loss of progress |
What I tell patients: The release creates the opportunity. Repetition turns that opportunity into a lasting change.
The biggest mistake
The most common mistake is treating the procedure like a one-time fix.
Infants often need feeding support after the release because improved mobility still has to be integrated into latch and milk transfer. Children may need help turning that mobility into better oral rest posture and clearer speech habits. Adults often need more deliberate retraining because compensation can involve breathing, jaw tension, sleep quality, and years of overuse.
Pain and Sleep Therapy Center provides laser frenectomy as part of a broader evaluation that can include TMJ, airway, and myofunctional factors. That coordinated model matters because the procedure works best as a catalyst for functional improvement, not as an isolated event.
Impact on Breastfeeding Speech Sleep and TMJ
The reason patients consider a frenectomy isn't the appearance of the tissue. It's the effect that tissue has on daily life. When the release is paired with proper functional retraining, the benefits can reach well beyond the mouth.
Breastfeeding and early feeding
In infants, the immediate concern is usually latch. A restricted tongue may struggle to lift and cup properly, which can make milk transfer inefficient and feeding uncomfortable. Parents may notice clicking, leaking, shallow latch, or long feeds that don't seem satisfying.
After release, feeding often improves because the tongue can move with less restriction. But the best outcomes usually happen when feeding support continues after the procedure. Babies still need to learn a new pattern, and parents often need reassurance about what normal adjustment looks like.
Speech and oral development
In children, tongue mobility can influence articulation, chewing mechanics, and oral rest posture. A low, restricted tongue doesn't just affect individual sounds. It can shape how the mouth functions all day.
That matters because speech isn't only about the tongue moving during words. It's also about what the tongue does the rest of the time. A child who learns to rest the tongue in a healthier position and swallow more efficiently often gains more stable control overall.
Here's a breakdown:
- Release alone: Improves access to movement
- Therapy after release: Improves control of movement
- Consistent rest posture: Supports lasting functional change
Sleep and breathing
Adults often connect the dots only after years of symptoms. A tongue that lives low in the mouth can reinforce mouth breathing and poor oral posture. During sleep, that pattern may contribute to airway instability, snoring, restless sleep, and waking unrefreshed.
A frenectomy is not a universal sleep treatment. It won't replace a proper airway evaluation. But when tongue restriction is part of a larger breathing pattern problem, releasing the tissue can help create better conditions for nasal breathing and improved tongue posture during rest.
That's why airway-focused care matters. The anatomy may need to change, but the breathing pattern often needs to change too.
Better sleep outcomes don't come from a release alone. They come from matching the release with better breathing mechanics and better tongue posture.
TMJ, facial tension, and neck strain
TMJ pain is often multifactorial, but tongue restriction can contribute to the load. When the tongue can't stabilize and posture well, the jaw and neck may overwork to compensate. Patients then describe clenching, muscle fatigue, headaches, or tension under the chin and through the sides of the neck.
Adults are often surprised by this connection because no one previously linked tongue posture to jaw comfort. Yet the tongue is part of the whole musculoskeletal system of the mouth and upper airway. If its movement is limited, other structures often pick up the slack.
That doesn't mean every TMJ problem starts with a tie. It means a restricted frenulum can be one of the hidden drivers in a larger pattern of dysfunction.
Your Questions Answered and Next Steps
Patients usually have a few practical questions left by the end of this conversation. Here are the ones that come up most often.
Does the procedure hurt
Most patients tolerate a laser release well because it's quick and minimally invasive. Discomfort is usually more manageable than people expect. The bigger challenge is often staying consistent with aftercare rather than getting through the procedure itself.
Is someone too young or too old for treatment
No single age determines whether treatment makes sense. The right question is whether the frenulum is restricting function and whether the patient has a realistic plan for recovery and retraining. Infants, children, and adults can all be candidates when the evaluation supports it.
Will a frenectomy fix everything by itself
Usually not. It can remove a major mechanical barrier, but it doesn't automatically correct the habits built around that barrier. If breathing, swallowing, speech, or muscle tension patterns have adapted over time, those patterns often need active retraining.
What should I ask at a consultation
Ask practical questions:
- How do you decide whether the tie is functionally significant
- What aftercare do you require
- Do you coordinate with lactation, speech, or myofunctional therapy when needed
- How do you monitor healing and reattachment risk
If you want help preparing for that visit, these expert tips to ask the right questions can help you organize concerns ahead of time.
What are the next steps if I suspect a tongue tie or lip tie
Start with a functional evaluation, not just a quick visual check. Bring your symptom history. For infants, note feeding patterns and latch concerns. For children, note speech, chewing, mouth posture, and sleep issues. For adults, include jaw tension, breathing patterns, headaches, and sleep complaints.
The most useful treatment plans are collaborative. A provider may involve lactation support, myofunctional therapy, airway assessment, speech guidance, or TMJ-focused care depending on the patient's age and symptom pattern.
A well-done laser release can be a turning point. The patients who do best are usually the ones who understand that the procedure opens the door, then walk through it with consistent follow-through.
If you'd like a functional evaluation for tongue tie, lip tie, TMJ symptoms, or sleep-related breathing concerns, Pain and Sleep Therapy Center offers collaborative assessment with laser frenectomy, myofunctional therapy guidance, and airway-focused care for infants, children, and adults.



