
Cleft lip repair is typically done around 3 to 6 months, and cleft palate repair around 9 to 12 months. That timeline is a flexible guide, not a rigid rule, because your baby's team also has to balance feeding, breathing, growth, and anesthesia safety.
If you're reading this soon after a diagnosis, you may feel like everything arrived at once. You were probably told a lot of new words in one conversation, and now the question sitting at the top of your mind is simple: When will surgery happen, and why that age? The reassuring answer is that cleft care usually follows a well-established path, but your child's doctors don't choose dates from a generic calendar. They choose them based on function.
Your Guide to the Cleft Care Journey
Most parents first want dates. That makes sense. A date feels concrete when everything else feels uncertain.
But the cleft surgery journey makes more sense when you think of it this way: each step is timed to help your child do an important job well. Feed. Breathe. Grow. Hear. Speak. Surgery is part of that process, not the whole process.
What parents often need explained early
A baby with a cleft lip, cleft palate, or both doesn't move through care as a series of isolated events. A coordinated team watches how your child is eating, gaining weight, breathing, and preparing for later milestones like speech. That's why two children with a similar diagnosis might not have surgery on exactly the same day or even in exactly the same month.
For many families, the first few weeks are filled with practical concerns, not abstract ones:
- Feeding today: How do we help our baby take enough milk comfortably?
- Growth before surgery: Is weight gain on track?
- Planning ahead: What happens first, and what can wait?
- Support systems: Which appointments matter most right now?
If insurance and follow-up care are adding stress, a caregiver resource like this Guide to Medicaid dental for caregivers can help you ask better coverage questions as you organize treatment.
A steady timeline matters, but a safe and functional timeline matters more.
Many parents also feel better once they know they're not expected to figure this out alone. A cleft team usually coordinates surgery with feeding support, hearing checks, speech monitoring, dental planning, and family guidance. If you want an example of how a coordinated program is structured, a dedicated cleft palate clinic can show how these specialties fit together around one child.
The question behind the question
When you ask about cleft lip and palate surgery age, you're often asking something deeper: Will waiting hurt my child? Will earlier surgery help more? Why not fix everything immediately?
Those are the right questions. The answers depend on the job each surgery needs to do. Lip repair is often done earlier because the lip helps with seal, feeding mechanics, and facial form. Palate repair is timed differently because the palate has a major role in separating the mouth from the nose and supporting normal speech patterns as language begins to emerge.
The Cleft Lip and Palate Surgery Timeline
At your first cleft team visit, one of the hardest parts is hearing that care happens over years, not in one operation. That can sound overwhelming until the timeline is tied to purpose. Each step is timed around what your child needs to do next: feed safely, breathe well, learn speech sounds, and grow with the best possible support for the teeth, jaw, and nose.
The early milestones
Across major cleft programs, the broad pattern is similar. Lip repair is often done in early infancy, and palate repair usually follows later in the first year, as described in Seattle Children's overview of cleft care timing.
The gap between those surgeries is intentional. The lip can often be repaired once a baby is healthy enough for anesthesia and growing steadily. The palate is timed with a different goal in mind: closing the opening early enough to support normal speech development, while choosing an age that is still safe for the child and appropriate for healing.
Parents often ask why everything cannot be repaired at once. The short answer is that each procedure has a different job. Surgeons are not only closing a gap. They are helping set up how the mouth and nose will work together over time. If you want a closer look at how cleft palate repair is performed and why technique matters, it helps explain why timing is so closely linked to function.
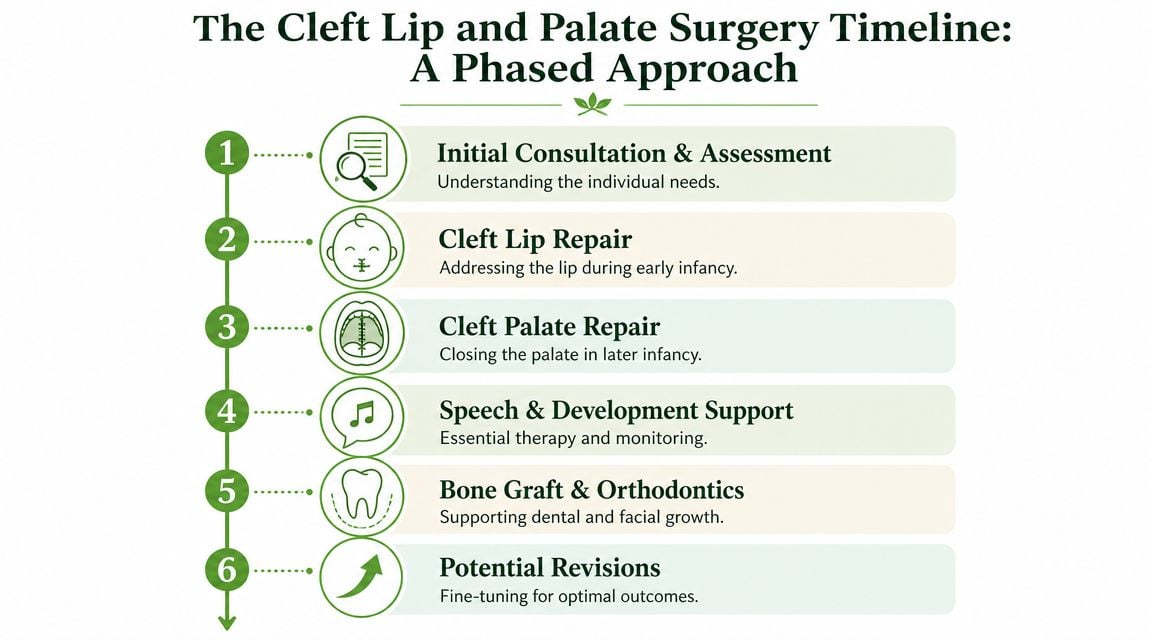
Typical Cleft Surgery Timeline
| Surgery | Typical Age | Primary Goal |
|---|---|---|
| Initial consultation and assessment | Early after diagnosis | Clarify feeding, airway, cleft type, hearing needs, and the treatment plan |
| Cleft lip repair | 3 to 6 months | Improve lip function, seal, and facial form |
| Cleft palate repair | 9 to 12 months | Separate the mouth from the nose and support speech and feeding |
| Speech and development support | Ongoing after early repairs | Monitor speech, swallowing, hearing, and oral function |
| Bone graft and orthodontic planning | Later childhood | Support teeth, jaw structure, and the dental arch |
| Possible revisions or jaw procedures | As growth continues | Improve bite, breathing, appearance, or other functional concerns |
Why the order matters
The order follows development.
A baby needs enough strength and medical stability for early surgery. Then the team looks ahead to speech. The palate matters because it helps direct air and sound correctly. If that structure is not working well as words begin to develop, children can start building speech habits around the opening, and those habits may need therapy later even after a successful repair.
That is why cleft care goes beyond a calendar. It is a function-based plan.
- Lip repair comes early because improving lip seal can support feeding mechanics, control of secretions, and the way the lip and nose work together.
- Palate repair is timed before speech patterns mature so the child has a better foundation for producing pressure sounds clearly.
- Therapy continues after surgery because repaired anatomy still has to be used well. Speech-language pathologists, audiology, dental specialists, and orofacial myofunctional therapy can all play a role in how children breathe, swallow, and coordinate oral muscles.
- Bone grafts and jaw procedures happen later because those decisions depend on facial growth and tooth development, not just age on a birthday chart.
- Revisions can be part of good planning because the face changes as a child grows, and treatment sometimes needs to adjust with that growth.
One helpful way to frame the timeline is this: the team is building function in layers. First comes safe healing and basic structure. Then come speech, breathing, dental support, and facial growth.
Cleft care in phases is planned care, designed to support long-term speech, breathing, feeding, and growth.
The timeline often feels more manageable once the reason behind each stage becomes clear.
Primary Surgeries Cleft Lip and Palate Repair
You meet the surgeon, hear two procedure names, and leave wondering why one repair may happen first while the other waits. That question is one of the hardest parts of early cleft care, because to a parent, both needs feel urgent.

The reason the surgeries are staged is simple. The lip and the palate do different jobs, so the team times each repair around the function they are trying to protect. Early decisions are not only about closing an opening. They are about building the foundation for feeding, breathing, speech, and facial growth.
Cleft lip repair
Cleft lip repair is often the first major surgery families encounter. It improves appearance, but that is only part of the goal. The surgeon is also rebuilding a lip that can form a better seal, help manage saliva and milk, and support the shape and function of the nose.
Many clinicians learned the classic rule of 10s as a guide for lip repair readiness: about 10 weeks of age, 10 pounds, and hemoglobin around 10 g/dL, as described in Cleveland Clinic's cleft surgery overview. Today, teams often use that benchmark as a reference point rather than a fixed rule. A baby's feeding, growth, airway, and overall health matter more than hitting a date on the calendar exactly.
That matters for parents to hear. If surgery is scheduled a little later than expected, it usually means the team is protecting safety and recovery, not losing the window for good results.
Why lip repair happens in early infancy
The upper lip works like the front seal of the mouth. When that seal improves, babies may handle feeding mechanics more effectively, and the lip and nose can begin working together in a more balanced way.
Early infancy is often a good time for this repair because the team is trying to support function while the baby is still developing basic patterns for sucking, swallowing, and facial movement. Parents may hear “early” and worry that the process is being rushed. In practice, early timing usually means the baby is healthy enough to benefit and strong enough to recover well.
Cleft palate repair
Palate repair follows a different logic. The palate is the wall between the mouth and the nose. When that wall is open, feeding can be less efficient, air escapes differently, and later, speech sounds that need pressure inside the mouth can become harder to produce clearly.
This is why palate timing gets so much attention. Surgeons are not only closing tissue. They are trying to give the child a better physical setup for speech before speech patterns are firmly established. If you want a clearer picture of the anatomy and surgical approach, this overview of how cleft palates are repaired can help.
A repaired palate also needs good teamwork after surgery. Speech-language pathologists, audiologists, dental specialists, and clinicians trained in orofacial myofunctional therapy may all help a child learn to use the repaired structures well for speech, breathing, and swallowing.
Here's a helpful visual overview before we go further.
Why the palate isn't repaired at the same time as the lip
This can feel confusing at first. If both areas need surgery, why separate them?
Because each procedure has its own purpose, technical demands, and timing goals. Lip repair is often scheduled once the baby is medically ready and the team believes early improvement in lip function will help. Palate repair is planned around a different set of priorities, especially speech development, healing, airway considerations, and growth.
A useful way to picture it is a house built in stages. One crew secures the front entry so the home works better right away. Another crew comes at the point when the interior wall can be rebuilt without disrupting the rest of the structure. In cleft care, timing follows that same logic. The team is choosing the moment when each repair is most likely to support long-term breathing, feeding, and speech.
Factors That Influence Surgical Timing
A standard timeline is useful. Your child's actual timeline is more personal.
Some families hear one date at diagnosis and a different date later on. That can feel unsettling, but it usually reflects careful decision-making, not confusion. Teams are balancing developmental goals with surgical and anesthesia safety.
The balance between function and safety
Parents often wonder whether surgery age is driven more by speech goals or by safety. The answer is both. The American Society of Plastic Surgeons notes in its cleft lip and palate repair review that timing varies widely by team protocol and the child's health, and that this timing often involves balancing the benefits of early surgery for speech with the need to make sure the child is medically ready.
That's why a timeline may shift even when everyone agrees on the overall goals.
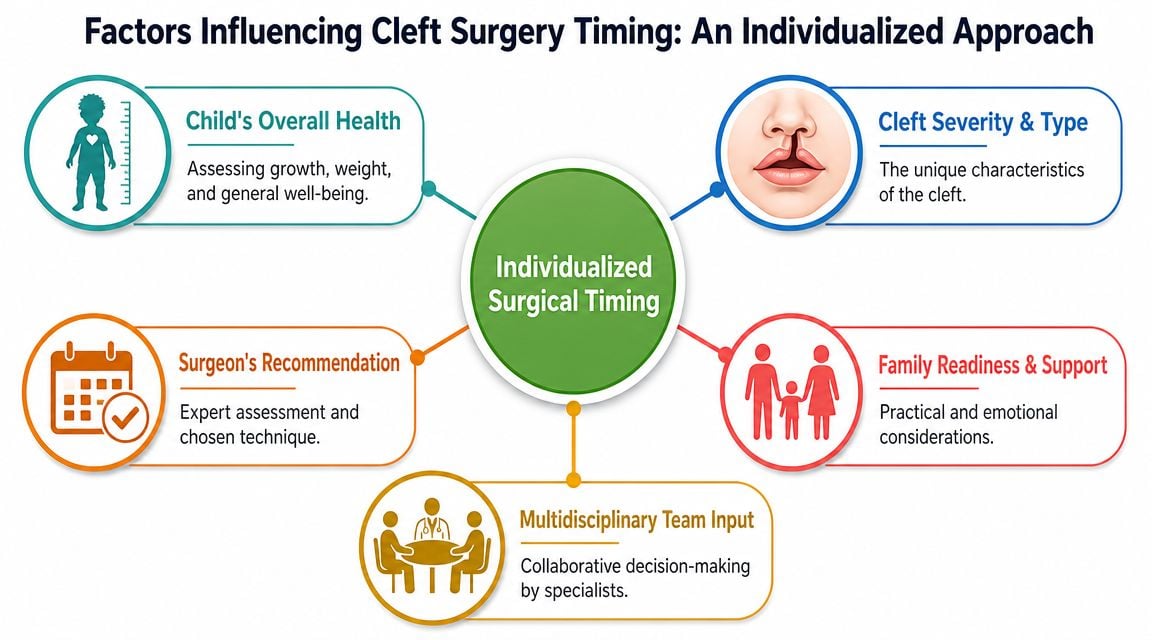
What your team is watching
Several factors commonly influence the timing of surgery:
- Growth and nutrition: Babies need enough strength and reserve to recover well from anesthesia and surgery.
- Airway stability: If breathing is a concern, the team may address that before moving ahead.
- Feeding efficiency: A baby who's struggling to feed may need targeted support so growth improves first.
- Other health conditions: Heart, lung, genetic, or neurologic issues can change the timing.
- Cleft pattern and severity: The anatomy itself affects surgical planning.
- Team protocol: Different experienced centers may use slightly different timing windows.
What looks like a delay on paper may actually be a safer, smarter plan for your child.
Why one child's schedule may not match another's
This is one of the hardest parts for families in online support groups. You may hear another parent say their baby had surgery earlier, and it's easy to wonder whether your child is being left behind.
Usually, that comparison doesn't help. One baby may be feeding well and gaining steadily. Another may need more time to build weight or manage airway concerns. The same diagnosis label doesn't guarantee the same timing.
When you ask your team, “Why this month?” you deserve a practical answer. It should include both sides of the decision: what developmental benefit they're aiming for, and what medical readiness signs they want to see.
Later Procedures Bone Grafts and Revisions
For many families, the early surgeries are so emotionally intense that it's hard to think years ahead. But cleft care often continues as your child grows, especially when teeth, jaw shape, and facial balance become more important.
Bone grafts support the dental arch
Later childhood may include alveolar bone grafting, which helps provide support where the gum ridge and dental arch need continuity. In practical terms, this helps create a better foundation for teeth and for the shape of the upper jaw.
Parents sometimes hear “another surgery” and worry that the first surgeries didn't work. That's usually not the right way to think about it. A bone graft often addresses a different stage of development. It's tied to how the dental arch matures and how permanent teeth need support.
Revisions are part of long-term care for some children
As children grow, some need additional procedures to improve lip appearance, nasal shape, speech-related anatomy, bite, or jaw relationships. These are often refinements based on growth, not signs of failure.
A 2023 study from the Al Madinah Region in Saudi Arabia reported that after initial cleft lip repair, 47.9% of children experienced imbalance in facial expression and about 40% of parents sought additional procedures, according to the published study on outcomes after repair. That doesn't mean every child should expect the same experience. It does show that cleft care often extends beyond the first operation.
If you want a clearer sense of how later-stage planning fits into the full reconstructive journey, this overview of cleft palate reconstruction can help frame those conversations.
Common later goals
Later procedures may be recommended to help with:
- Dental support: Creating a more stable area for tooth eruption and orthodontic movement.
- Speech-related function: Improving anatomy if resonance or closure problems remain.
- Jaw fit: Correcting bite relationships that become clearer with growth.
- Lip or nose revision: Refining symmetry, contour, or function after healing and development.
Children grow. Their face grows with them. Cleft care has to grow too.
The Team Beyond the Surgeon Essential Therapies
Parents often feel a wave of relief after surgery is done. Then a new question shows up. How does my child learn to use this repaired anatomy well for feeding, breathing, and speech?
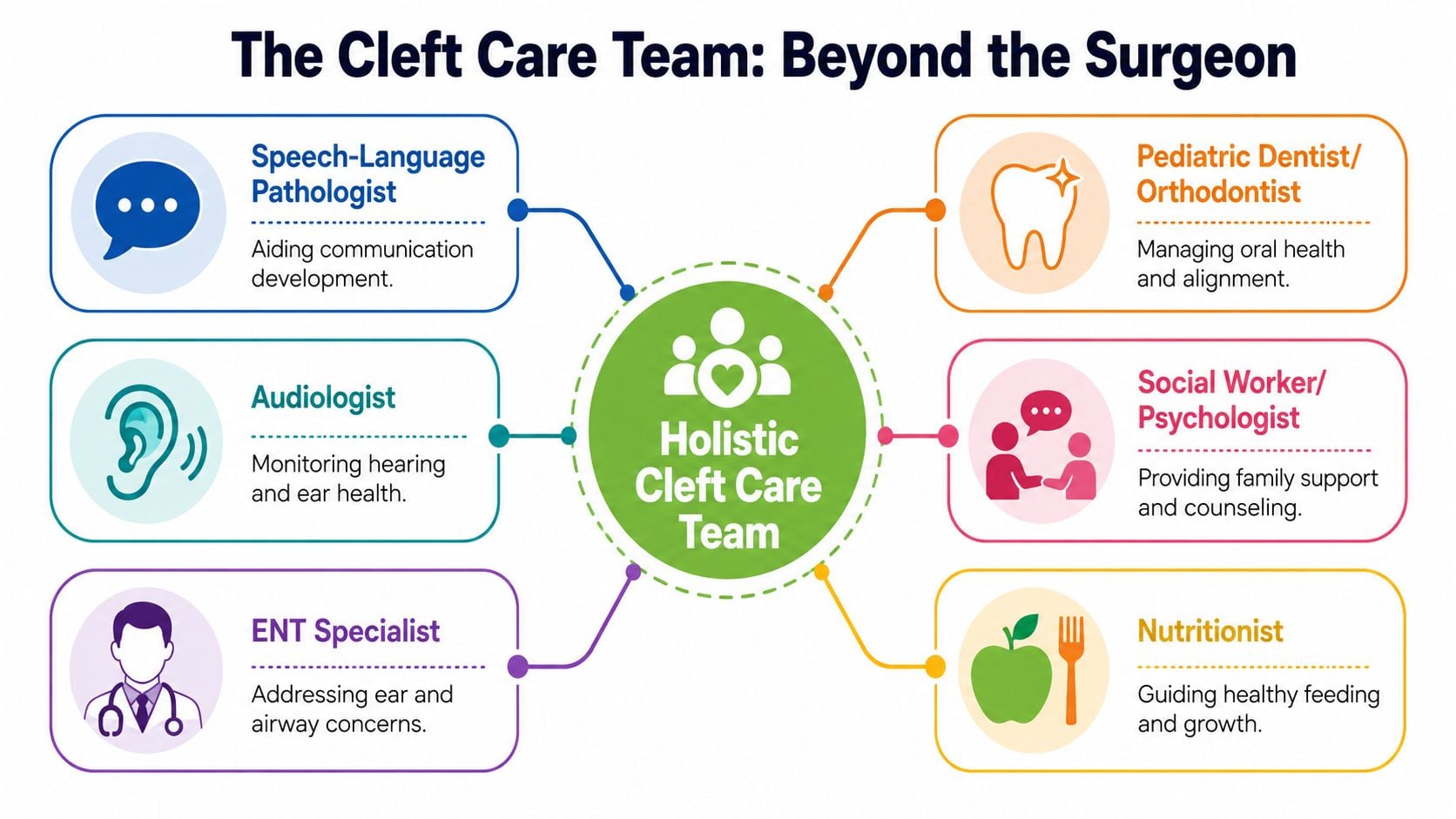
That question matters because cleft care is not only about closing a gap. It is about helping the mouth and airway work as a coordinated system over time. The best cleft programs bring together several specialists, each focused on a different part of that job.
Speech and feeding shape daily life
A repaired lip or palate gives a child better structure. Practice and therapy help that structure become useful in everyday life.
A speech-language pathologist watches how your child produces sounds, manages airflow, and develops resonance. A feeding specialist helps with sucking, swallowing, pacing, and oral coordination before and after surgery. Those skills are closely tied to growth, comfort, and family routines, so they are never side topics in cleft care.
A simple way to picture it is this. Surgery builds the instrument. Therapy helps the child learn how to play it.
Some children do beautifully with anatomy alone. Others need guided practice because they have learned workarounds before repair, or because healing does not automatically create efficient movement patterns.
Where orofacial myofunctional therapy fits
Orofacial myofunctional therapy focuses on how the lips, tongue, cheeks, and facial muscles work together during rest, breathing, swallowing, and speech-related tasks. In cleft care, that focus can be valuable because long-term outcomes depend on function, not only appearance.
For some children, the goals may include:
- Nasal breathing: Supporting healthier breathing patterns when the airway allows it
- Tongue posture: Encouraging a resting position that supports oral development and speech
- Lip function: Improving lip seal and coordination
- Swallowing patterns: Reducing habits that place extra strain on the mouth or interfere with efficient swallowing
This kind of therapy is usually one piece of a larger plan. It works best when the cleft team, speech professionals, dental providers, and medical specialists are all paying attention to the same long-term goals.
Pain and Sleep Therapy Center is one example of a clinic that offers orofacial myofunctional therapy within interdisciplinary care focused on breathing, swallowing, and oral posture.
Dental, hearing, and family support also matter
Teeth, ears, and speech development are connected more than many parents expect. Orthodontists and pediatric dental teams monitor eruption patterns, crowding, and arch development. Audiologists and ENT specialists track hearing and middle ear health, which can influence language learning and speech progress.
Families need support too.
Care coordinators, social workers, and psychologists often help parents keep track of appointments, school questions, insurance issues, and the emotional weight of long-term treatment. Even simple home routines can make follow-up feel more manageable. If your child later uses orthodontic appliances or retainers, this complete guide on retainer care can help make daily cleaning and maintenance feel more straightforward.
Common Questions About the Cleft Surgery Timeline
What if my child's surgery is later than the typical window
A later date doesn't automatically mean something is wrong. It often means the team is balancing developmental benefits with your child's health, growth, feeding, and anesthesia readiness. Ask what specific milestone they're waiting for. The answer should be concrete.
Will my child always have a visible scar or difference
Most children do have some lasting evidence of surgery, but scars and facial balance usually change over time as healing and growth continue. Some children later have revision procedures to improve form or function. Those decisions are often made gradually, not all at once.
Is the rule of 10s still a hard requirement
No. It remains a well-known historical readiness guideline for lip repair, but many teams now individualize timing instead of following it rigidly. If your child doesn't fit that benchmark exactly, the more important question is whether they're healthy enough for safe surgery and likely to benefit from it at that time.
If speech is the goal, does surgery alone solve speech problems
Not always. Surgery creates the structure needed for better speech, but children may still need speech therapy or other follow-up if they've developed compensatory patterns or have ongoing resonance issues. Good anatomy is the foundation. It isn't the entire outcome.
If you're trying to understand how breathing, oral posture, swallowing, and facial muscle function fit into long-term cleft outcomes, Pain and Sleep Therapy Center provides educational resources and clinical services related to orofacial myofunctional therapy, pediatric oral function, and airway-focused care. For families who want a fuller picture beyond surgery dates alone, that kind of interdisciplinary perspective can be a useful next step.



