
You may be reading this after another rough night. You snored, woke up gasping, ripped off your CPAP mask, or stared at a sleep study report full of terms that felt more alarming than helpful. Now someone has mentioned jaw surgery, and you're trying to answer a hard question: is this a life-changing fix, or too big a leap?
That question deserves a careful answer.
Maxillomandibular advancement, often called MMA, is one of the most powerful treatments available for obstructive sleep apnea. It can dramatically enlarge the airway by moving the upper and lower jaws forward. But this is also major surgery with real recovery, real trade-offs, and one uncomfortable truth patients don't hear often enough: even with strong overall success rates, doctors still can't reliably predict who will be fully cured before surgery.
What Is Maxillomandibular Advancement
Maxillomandibular advancement, or MMA, is an operation that moves both the upper jaw (maxilla) and lower jaw (mandible) forward. In sleep apnea treatment, the goal is functional. By bringing the jaw framework forward, the surgeon increases the space behind the tongue and soft palate, where the airway often narrows or collapses during sleep.
For some patients, that idea is confusing at first. Sleep apnea can sound like a problem caused only by soft tissues. In reality, the shape and position of the facial bones often set the stage for how crowded the airway is before sleep even begins.
Why this surgery can work so well
MMA differs from procedures that only remove, trim, or tighten tissue in one spot. It changes the skeletal framework that supports the entire upper airway. That broader effect helps explain why surgeons and sleep specialists often view it as one of the strongest surgical options for obstructive sleep apnea, especially in people whose anatomy leaves limited room behind the tongue.
A review in the Journal of Oral and Maxillofacial Surgery describes MMA as a procedure that enlarges the pharyngeal airway by advancing the facial skeleton and is widely used for patients with moderate to severe OSA who cannot tolerate other therapy in this overview of surgical sleep apnea treatment.
The key point is simple. MMA changes the physical boundaries around the airway, not just the tissue that falls inward during sleep.
Who usually considers MMA
Patients usually reach this discussion after other treatment paths have been explored. MMA is most often considered for moderate to severe OSA, for people who cannot use CPAP consistently, for patients who have not improved enough with oral appliances or other procedures, or for those whose facial and jaw structure appears to contribute to airway crowding.
Some people have an obvious recessed chin or underdeveloped midface. Others do not. A person can have sleep apnea related to jaw position without having a face that clearly signals "jaw surgery" to friends or family. If you're considering sleep apnea surgery options, it helps to see MMA as one part of a wider treatment spectrum, especially since it changes anatomy more extensively than many other operations.
You can also review this local collection of resources on oral surgery for sleep apnea to understand how MMA fits within the broader category.
What patients often misunderstand
Patients often hear that MMA has high success rates and assume that means the outcome for them is easy to predict. That is where the decision gets harder. MMA is highly effective at a group level, but a fully predictable "cure" for one individual is much harder to promise before surgery.
That predictability gap matters in real life. Two patients can have the same diagnosis on paper and very different results because sleep apnea is shaped by several factors at once, including anatomy, weight, muscle tone during sleep, nasal breathing, sleeping position, and how severe the collapse is at different airway levels.
So the conversation should stay grounded. MMA can be life-changing for the right patient, but it is still major surgery. That is why a careful team usually works through conservative options first, then asks a more precise question: does this person's anatomy make MMA a reasonable step, given both the potential benefit and the commitment involved?
Function comes first
Many patients worry first about facial appearance. That concern is understandable. Yet in sleep medicine, the first question is whether moving the jaws forward is likely to create more stable breathing through the night.
Appearance can change, sometimes subtly and sometimes more noticeably. The purpose of the operation, however, is to improve airway function and reduce obstructive events during sleep. That distinction helps patients evaluate MMA with clearer expectations and less fear.
The MMA Surgery Journey What to Expect
You meet the surgeon, hear that both jaws will be moved forward, and your first thought is often simple: What does that look like for a real person, day by day?
The journey is longer than the operation itself. MMA asks for planning before surgery, patience after surgery, and a clear understanding that even a technically successful procedure can heal differently from one patient to the next. That predictability gap matters here too. Surgeons can measure bones and study the airway carefully, but recovery and final sleep results still cannot be promised with perfect precision for any one individual.

Before surgery
Preparation usually involves more than one specialist. Many patients are evaluated by a sleep physician, an oral and maxillofacial surgeon, and sometimes an orthodontist. Each person is looking at a different part of the same problem. One focuses on the sleep disorder, another on the jaw bones and airway space, and another on how the teeth will meet after the jaws are moved.
That last point can be confusing. Patients often assume the surgery is only about opening the airway. It is also about preserving a functional bite. The upper and lower jaws have to move in a way that creates more room behind the tongue and soft palate while still letting the teeth fit together properly after healing.
A published review notes that surgeons commonly aim for large enough advancement to create a meaningful airway change, often at least 10 mm in the lower jaw, and it also reported improvements in symptoms and quality of life for many patients after surgery in this open-access review. That does not mean every patient gets the same result. It means planning the size and direction of movement is one of the biggest decisions before anyone enters the operating room.
If anesthesia is one of your biggest worries, this overview of oral surgery anesthesia options can help make the process feel more concrete.
On the day of surgery
MMA is done under general anesthesia in a hospital or surgical setting. The surgeon makes controlled cuts in the upper and lower jaw bones, brings both jaws forward, and secures them with plates and screws. The basic idea is mechanical. Moving the facial framework forward also pulls attached soft tissues forward, which can enlarge the space where airflow tends to collapse during sleep. A detailed surgical review describes this forward movement and fixation as the core of the procedure in this review of maxillomandibular advancement for obstructive sleep apnea.
Many patients expect severe pain to be the main issue right away. Swelling, stuffiness, fatigue, and a strange sense that the face does not feel quite normal are often more noticeable than sharp pain during the first phase.
Bring your focus to basics. Rest. Fluids. Help at home.
The first days after surgery
Early recovery can feel slow, messy, and frustrating. Your face swells. Speaking may sound different. Eating becomes a project rather than a routine task. Sleep may still be disrupted for a while because your body is healing and your nose or throat may feel congested.
A simple plan helps:
- Food: Prepare soft foods ahead of time that are easy to swallow and do not require much chewing.
- Support: Arrange for help with transportation, medications, and daily tasks during the first stretch of recovery.
- Work: Tell family and coworkers that your energy, speech, and schedule may be limited for a while.
- Expectations: Healing is uneven. A better morning can be followed by a more swollen evening.
What recovery feels like emotionally
This part deserves attention too.
Patients often cope better when they expect recovery to be inconvenient and sometimes discouraging. The face is swollen, the bite feels unfamiliar, and sensation may be temporarily altered. That combination can make people wonder whether what they are feeling is normal.
Often, it is. Healing after a major jaw operation rarely feels graceful. It feels more like your body is rebuilding around a new frame, the way a house needs time to settle after structural work. That is one reason MMA should never be treated like an easy shortcut for sleep apnea. It can be life changing for the right patient, but it asks for real commitment before, during, and after surgery.
Weighing the Outcomes Benefits Versus Risks
A patient sits in clinic after years of poor sleep, failed masks, and growing exhaustion. The question is simple on the surface: if MMA can work so well, why not just do the surgery? The honest answer is that this procedure can be life changing, but it is also a major structural operation with real trade-offs, and no surgeon can promise a cure for one specific person.
That uncertainty is the predictability gap. MMA often improves obstructive sleep apnea because it enlarges the airway at its bony framework. But "highly effective" is not the same as "guaranteed." Two patients can have similar sleep study numbers and very different results after surgery because anatomy, healing, nerve recovery, weight changes, bite stability, and the pattern of airway collapse all matter.
The upside
MMA treats the problem more like widening a narrow hallway than propping the door open each night. By moving the upper and lower jaws forward, it can create more room behind the tongue and soft palate. For the right patient, that can mean fewer breathing events, less effort to breathe during sleep, and less dependence on nightly equipment.
The potential benefit is not only about the sleep study report. Patients who improve often notice changes in daily function that feel much bigger than a number on a page:
- Easier mornings
- Better alertness and concentration
- Less disruptive snoring
- More confidence traveling or sleeping away from home without equipment
There is also a practical appeal here. MMA does not depend on perfect nightly adherence the way CPAP does. If the surgery works well, the airway change is built into your anatomy.
The downside
MMA asks a great deal of the patient. It is jaw surgery, not a minor airway procedure. The risks include pain, swelling, bleeding, infection, bite changes, relapse of jaw position, need for orthodontic planning in some cases, hardware concerns, and a long recovery arc even when healing goes well.
The issue many patients focus on after the swelling fades is altered sensation. Numbness or tingling of the lower lip, chin, gums, or cheeks is common after jaw movement. In many people it improves over time. In some, it does not return fully. That may sound abstract before surgery, so it helps to make it concrete. Sensation changes can affect kissing, shaving, applying lipstick, noticing food on the lip, or feeling that your face is fully your own again.
Appearance matters too. Advancing the jaws usually changes the profile. Some patients welcome that change. Others feel neutral. Some need time to adjust, even if the surgical result is technically excellent. Functional concerns can also persist in a minority of patients, including changes in bite comfort, chewing, or swallowing mechanics.
A balanced way to think about it
The decision is not "benefits versus risks" in the abstract. It is whether the likely gain in breathing and quality of life is worth the cost, recovery, and uncertainty for you.
| Potential benefit | Potential trade-off |
|---|---|
| Larger airway space | Major surgery with a demanding recovery |
| Lower sleep apnea burden | Sensory changes that may last |
| Less reliance on CPAP or an oral appliance | Permanent facial and bite changes |
| Better daytime function and quieter sleep | Possible need for future dental, bite, or hardware follow-up |
This is why careful consent matters so much. A good MMA candidate is not only someone with severe sleep apnea. It is someone whose anatomy fits the procedure, who understands that improvement is more predictable than cure, and who has already given serious attention to conservative options when appropriate.
For some patients, MMA is the right answer. For others, the wiser answer is to keep working through lower-risk treatments first. That is not settling. It is good medicine.
MMA Compared to Other Sleep Apnea Treatments
A common real-life situation looks like this: someone has moderate or severe sleep apnea, feels exhausted, has tried CPAP or is worried they will not tolerate it, and starts wondering whether surgery would finally solve the problem.
That is the right question to ask, but it needs one more layer. The decision is rarely about finding the strongest treatment on paper. It is about choosing the treatment that fits your airway, your daily life, and your tolerance for uncertainty. MMA is powerful, yet there is still a predictability gap. We can often predict improvement better than we can predict a complete cure for one specific person.
A practical comparison
| Treatment | What it does | Main advantage | Main limitation |
|---|---|---|---|
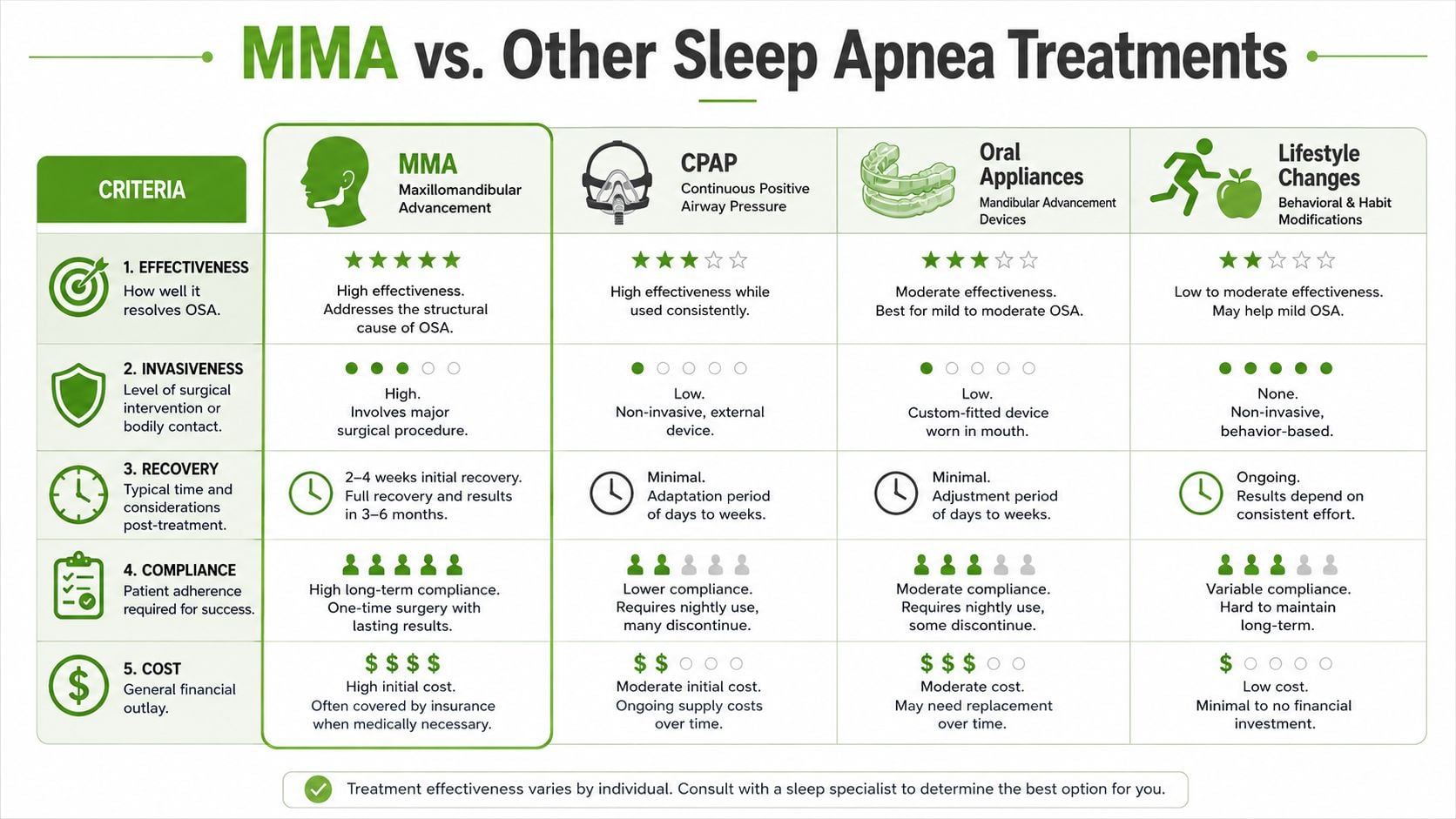
| CPAP | Uses pressurized air to keep the airway open during sleep | Non-surgical and highly effective when used consistently | It helps only while you are wearing it |
| Oral appliance | Holds the lower jaw forward during sleep | Less cumbersome than CPAP for some patients | Response varies by anatomy and severity |
| Lifestyle and airway-focused care | Addresses contributors such as weight, nasal blockage, sleep position, and breathing habits | Low risk and often helpful as part of a larger plan | Usually not enough by itself for severe structural collapse |
| MMA | Surgically moves both jaws forward to create more airway space | The strongest anatomy-changing surgical option | Major operation with lasting facial, dental, and recovery implications |
MMA versus CPAP
CPAP works like a pneumatic splint. It uses air pressure to hold the airway open from the outside in. MMA works by enlarging the airway framework itself.
That difference matters.
CPAP can be an excellent first choice because it is reversible, fast to start, and does not permanently change the face, bite, or nerves. For a patient who can use it night after night, it may control sleep apnea very well without surgery. If you are exploring CPAP alternatives for sleep apnea, the key comparison is not only effectiveness. It is also whether you want a nightly device, a removable treatment, or a permanent structural change.
MMA asks for the opposite kind of commitment. Instead of long-term equipment use, it asks for one major intervention with a demanding recovery and permanent consequences. Some patients prefer that trade. Others do not, and that is a medically reasonable choice.
MMA versus oral appliances
Oral appliances sit between CPAP and surgery for many patients. They are usually custom-made, adjustable, and removable. That makes them much easier to stop or modify if they are uncomfortable.
They also give useful information. If a patient feels and sleeps better with the lower jaw held forward, that suggests jaw position is part of the airway problem. It does not guarantee MMA will cure the sleep apnea, but it can help show whether forward movement improves the airway.
An oral appliance is still a treatment you wear. MMA is a permanent change to the jaw position and the airway behind it.
MMA versus soft tissue surgery
Soft tissue procedures focus on structures such as the palate, tonsils, tongue base, or nasal passages. Those operations can help selected patients, especially when the blockage is concentrated in one area. MMA is different because it widens the airway at multiple levels at the same time.
A useful analogy is remodeling a hallway. Soft tissue surgery may trim part of what is bulging into the space. MMA moves the bony walls forward, which can create a broader change in the passage itself. That is one reason many surgeons view MMA as the strongest skeletal surgical option for obstructive sleep apnea.
Pain expectations often surprise patients. Jaw surgery sounds more painful than throat surgery, but many patients report that the throat-focused procedures feel harsher during swallowing and early recovery. The bigger issue with MMA is usually not pain alone. It is the total package of swelling, numbness, diet changes, bite monitoring, and time to heal.
So how should you compare them?
Start with the least invasive treatment that has a real chance of working for your anatomy and severity. Then ask a harder question: if that option fails, why did it fail? Poor fit, poor tolerance, incomplete effect, or the wrong anatomy?
That step matters because MMA is not merely a stronger version of every other treatment. It is a different category of treatment. For the right patient, it can be life-changing. For the wrong patient, or for a patient who has not yet worked through good conservative options, it can mean a major surgery without the clean, predictable endpoint people hope for.
That is why careful sequencing matters. Conservative options are not a detour. They are often part of making a smarter decision about whether MMA is worth the cost, recovery, and uncertainty.
Success Rates and Long-Term Recovery
A common moment in clinic goes like this: a patient hears that MMA has one of the highest success rates in sleep apnea surgery and assumes the decision should be simple. Then the harder question appears. What are the odds that you will feel dramatically better, and what are the odds that your sleep study will become fully normal? Those are related questions, but they are not the same.
Success and cure mean different things in sleep medicine. A treatment can lower the apnea-hypopnea index, improve oxygen levels, reduce snoring, and help daytime function, yet still leave some residual obstructive sleep apnea. That distinction matters because MMA is a major operation. The usual goal is meaningful improvement with acceptable tradeoffs, not a guaranteed perfect endpoint.

What the evidence shows
One widely cited meta-analysis of MMA outcomes in adults found high overall surgical success rates and lower cure rates, with cure defined as an AHI below 5 events per hour in this review of maxillomandibular advancement for obstructive sleep apnea. In plain language, many patients improve a great deal. A smaller group reaches a completely normal or near-normal sleep study.
That is the predictability gap. Group results are strong, but individual certainty is limited.
This gap is one reason I encourage patients to slow down and examine all reasonable conservative options first. If CPAP, oral appliance therapy, positional therapy, weight management, nasal treatment, or combination care can control the problem with less risk, that matters. MMA can be life-changing. It is still irreversible surgery, and no surgeon can promise a cure for a specific person just because the averages look good.
What long-term recovery actually feels like
Recovery has two tracks running at the same time. One is medical healing of bone, soft tissue, bite, and sensation. The other is day-to-day adaptation, meaning sleep, speech, chewing, social comfort, and patience with a face that does not feel normal yet.
Early weeks
Many patients are more functional before they feel fully recovered. You may be answering emails, taking short walks, and sleeping better than expected while still dealing with swelling, lip or chin numbness, diet restrictions, and bite checks. A practical jaw surgery recovery timeline can help you picture the stages.
If you want a more procedure-specific overview, this guide to recovery after double jaw surgery explains the day-to-day rhythm in more detail.
Middle months
By several months out, the recovery story usually becomes less dramatic and more revealing. Swelling continues to settle. Eating and speaking tend to feel more natural. The bite often feels more stable. This is also when patients can judge the benefit more calmly because the noise of the early postoperative period has faded.
Some symptoms improve unevenly. Sensation may return gradually. Energy can improve before numbness does. Sleep study results may look better before your face feels fully like your own again.
Later healing
Final healing takes longer than many people expect. Orthognathic surgery literature consistently describes continued changes over many months, especially in swelling resolution, sensory recovery, and adaptation to the new jaw position as reviewed by the American Association of Oral and Maxillofacial Surgeons patient guidance on corrective jaw surgery. By the end of the first year, patients usually have a much clearer sense of both the functional result and the cosmetic result.
That long timeline matters emotionally. Early improvement does not always answer the whole question, and early frustration does not mean the final result will be disappointing.
The practical takeaway
MMA has one of the strongest track records among surgical treatments for obstructive sleep apnea. It also comes with a real recovery burden and an outcome that is easier to describe for groups than to predict for one person sitting in an exam room. That is why high success rates should start a careful conversation, not end it.
Is MMA Right for You A Patient-First Approach
You have tried to sleep with a mask. You have adjusted settings, changed cushions, and forced yourself through bad nights because you want to breathe and function again. Then someone mentions MMA, and it can sound like the definitive answer.
For some patients, it is a very reasonable option. For others, it is a major operation considered too early, before the underlying cause of airway collapse has been mapped clearly. That distinction matters because MMA is irreversible, recovery is demanding, and the result for any one person is never guaranteed.
The predictability gap
A hard truth deserves more attention: MMA has a strong overall record, but surgeons still cannot reliably predict who will reach a true cure, often defined as an AHI under 5, based on pre-surgical variables alone according to this review on MMA cure prediction.
This is the predictability gap.
Group outcomes can be encouraging while individual outcomes remain uncertain. In plain terms, a surgeon may be able to say, "This operation often helps people like you." What they usually cannot say with certainty is, "You will definitely be one of the people whose sleep apnea disappears."
That uncertainty should not scare you unnecessarily. It should make the decision more honest. MMA is not a shortcut past careful evaluation. It is a serious treatment choice made after the simpler, lower-risk paths have been examined fairly.
Why conservative care still matters
Sleep apnea is rarely just one thing. The airway behaves more like a narrow hallway with several pressure points than a single blocked door. In one patient, the jaw position is the dominant issue. In another, the bigger drivers may be nasal resistance, tongue posture, mouth breathing, weight changes, sleep position, or poor tolerance of a treatment that could still work with the right support.
That is why a patient-first approach starts by asking what problem needs solving before asking which surgery to schedule.
A careful sequence usually looks like this:
Clarify the diagnosis
Confirm the type and severity of OSA, your symptom pattern, and whether nasal, tongue, bite, or jaw anatomy appears to be a major contributor.Review non-surgical therapies thoroughly
CPAP, custom oral appliances, positional treatment, and breathing-focused therapies deserve a real trial when they fit the case.Separate structural problems from functional habits
Some patients have a skeletal airway problem. Others have several overlapping issues, such as chronic mouth breathing, poor tongue posture, nasal obstruction, or fragmented sleep habits.Discuss trade-offs in plain language
The right choice depends partly on values. One patient may accept lasting numbness for a strong chance of breathing better. Another may not. Both responses are reasonable.
Questions worth asking before surgery
Bring these questions to any MMA consultation:
- What problem do you think the surgery is solving in my specific case?
- What non-surgical options have I not fully explored yet?
- How likely is improvement versus complete cure, and how do you define each?
- What changes in sensation, swallowing, bite, or appearance should I realistically expect?
- If I still have residual OSA after surgery, what would the next step be?
These questions do more than gather information. They help you see whether the recommendation is specific to you or based mostly on MMA's reputation as a strong procedure in general.
A reasonable way to think about MMA
The healthiest frame is to view MMA as a high-commitment option for the right anatomy and the right circumstances.
It often makes the most sense when the airway problem has a strong skeletal component, conservative care has been tried seriously or is not workable, and the patient understands the risks well enough to accept them. That is very different from choosing surgery mainly because you feel worn down and want the decision-making process to end.
If you are early in the process, slowing down is often wise. If no one has carefully assessed nasal breathing, oral posture, tongue function, sleep habits, and appliance options, there may still be lower-risk steps worth taking first.
The goal is not to talk you out of MMA. The goal is to make sure that if you choose it, you are choosing it for the right reasons, with clear eyes about both its power and its limits.
Frequently Asked Questions About Life After MMA
A common moment after the surgical consult goes like this. A patient hears that MMA can be one of the strongest procedures for obstructive sleep apnea, then goes home and starts wondering about the part statistics do not answer. What will everyday life feel like after surgery, and what if breathing improves but the result still does not feel like a full cure?
Those are the right questions. MMA can create a larger airway by moving the jaws forward, but recovery is not just about the airway. It is also about sensation, chewing, swelling, appearance, and how your body adjusts over time. That predictability gap matters. A procedure can be highly effective overall and still be hard to forecast for one specific person.
Will my face look different
Usually, yes.
Because the upper and lower jaws are moved forward, some change in facial appearance is expected. For some patients, that change feels balanced or even welcome. For others, it feels unfamiliar at first. The best way to approach this is to ask your surgeon to show you, as concretely as possible, what changes they expect in your case rather than relying on general impressions from other patients.
Is numbness really sometimes permanent
Yes, it can be.
The nerves that give feeling to the lips, chin, gums, and parts of the face sit close to where surgeons work. Temporary numbness is common after jaw surgery. Some sensation often returns gradually over months, but some patients are left with lasting altered feeling. That does not always mean severe disability. It can mean an area feels dull, tingly, or slightly different forever. Even so, it is a real tradeoff, and it deserves a direct conversation before surgery.
When do people feel normal again
“Normal” usually comes back in stages, not all at once.
You may be up and around relatively early, yet still dealing with swelling, fatigue, a restricted diet, speech changes, or a bite that feels strange. Sensation can recover on a different timeline than chewing. Energy can recover on a different timeline than appearance. Recovery after MMA works a bit like settling into a renovated house. The major structure is changed in one day, but it takes time before everything feels familiar and easy again.
A better question is this: How would I feel if my breathing improved, but my face never felt exactly the same again?
If MMA is effective, why not just do it
Because a strong procedure is not the same thing as a predictable cure.
MMA is a major, irreversible surgery. It asks a great deal from the patient during recovery, and it still does not guarantee that sleep apnea will disappear completely for every individual. That is the center of the decision. The issue is not whether MMA can work well. The issue is whether it is the right step for your anatomy, your severity, your tolerance for risk, and your willingness to accept that some symptoms or treatment needs may remain afterward.
If you're weighing surgery against conservative care, Pain and Sleep Therapy Center offers a patient-first approach focused on root-cause diagnosis, airway evaluation, and non-surgical sleep solutions before major intervention. That kind of careful workup can help you understand whether maxillomandibular advancement belongs at the end of your treatment path, or whether there are safer steps to try first.



