
If you're reading this with a baby asleep on your chest, or while staring at your own upcoming frenectomy appointment, you're probably feeling two things at once. Relief that a restriction is finally being addressed, and uncertainty about what happens next.
That uncertainty is reasonable. A frenectomy releases tight tissue, but the procedure itself doesn't automatically create new movement patterns. Healing tissue wants to close. Muscles often fall back into familiar habits. In infants, that can affect latch and feeding comfort. In older children, teens, and adults, it can show up as limited tongue mobility, awkward swallowing, jaw tension, or frustration that the tongue still doesn't seem to move the way it should.
The most useful way to think about frenectomy exercises is this. The release creates opportunity. The exercises protect and train that opportunity. Some exercises are gentle wound-management stretches for babies. Others are active drills that teach the tongue and surrounding muscles how to work differently.
Families often need practical guidance, not vague instructions to “do stretches.” Adults need something more specific than infant aftercare sheets. If you're looking for broader support options alongside recovery, this overview of comprehensive tongue tie care Dulwich Hill gives a helpful example of the kind of multidisciplinary care many patients benefit from.
Your Guide to Frenectomy Exercises and Recovery
A frenectomy can be done for a tongue tie, lip tie, or both. The release frees restricted tissue. What happens after that matters just as much.
In practice, I tell families and adult patients to separate recovery into two jobs:
- Protect the healing site from reattachment
- Build functional movement so the new mobility is effectively used
Those jobs overlap, but they aren't identical. A newborn needs brief, precise aftercare performed by a caregiver. A teenager or adult needs conscious retraining, because years of compensation don't disappear in one appointment.
Why exercises matter after the release
After any oral release, the body begins healing immediately. That's normal. The challenge is that healing tissue can reconnect in a way that reduces the mobility you just gained.
For infants, aftercare often includes targeted manual movements done several times a day. For adults, recovery usually needs active tongue drills, mirror work, and attention to oral rest posture. A passive stretch alone may open the area, but it won't teach the tongue where to rest, how to raise, or how to move without recruiting the jaw, lips, or floor of mouth.
Core idea: A successful frenectomy isn't just an open wound that heals. It's a change in anatomy that needs guided function.
Age changes the exercise plan
The biggest mistake I see is assuming one handout works for everyone.
- Infants need short, calm, caregiver-led stretches timed around feeding and soothing.
- Children often do best with simple drills turned into games, using mirrors and cues they can understand.
- Teens and adults need neuromuscular re-education. They have to feel where the tongue is, notice old habits, and practice new patterns consistently.
That difference matters because people don't fail recovery from lack of effort alone. They fail when the instructions don't match the age, healing stage, or actual functional problem.
The sections below walk through what to expect, how to do infant frenectomy exercises gently, and how older patients can rebuild tongue mobility with purpose rather than guesswork.
What to Expect Before and After a Frenectomy
Preparation lowers stress. It also makes the first couple of days much easier, especially when you're tired and trying to remember instructions.
In the days before the procedure
Have your setup ready before the appointment, not after.
- Create a calm recovery spot: Pick one area with good lighting, a clean surface, burp cloths or tissues, and whatever soothing items usually help.
- Plan feeding support: If your baby is nursing, have lactation support lined up if needed. If you're bottle feeding, keep usual supplies washed and ready. If you're an older child or adult, stock soft, easy foods that don't require a lot of chewing.
- Practice hand positioning: Caregivers usually feel more confident when they've already learned how to support the baby's head and access the mouth gently.
- Clarify the aftercare routine: Ask your provider exactly when exercises begin, how often they're expected, and what the wound should normally look like during healing.
- Arrange backup help: The hardest sessions are often the first few. Another calm adult can make a big difference.
Some families also find it useful to review examples of effective treatment for lip and tongue ties so they understand how the procedure and follow-up care fit together.

The first 48 hours after the procedure
This period is usually more emotional than dangerous. The area looks raw. Babies may fuss. Adults may feel tightness more than dramatic pain.
What you may notice:
- Tenderness and swelling: Mild discomfort is expected.
- A white or yellow healing patch: This often worries people, but it can be part of normal healing tissue.
- Temporary changes in feeding or speech: A baby may latch differently while learning a new pattern. Older patients may notice that the tongue feels unfamiliar or clumsy.
- Fatigue and irritability: Recovery takes effort, even after a brief procedure.
What helps most right away
Keep the first two days simple.
- Use a steady routine: Do exercises at predictable times instead of waiting until the baby is already upset or the adult patient is exhausted.
- Focus on gentleness: Fast, forceful movements usually increase resistance and fear.
- Soothe immediately after: Feed, cuddle, rock, or use another calming routine so the session ends with regulation.
- Watch function, not just the wound: Better tongue lift, easier latch, less compensation, and smoother movement matter as much as appearance.
Most of the anxiety in the first two days comes from not knowing what's normal. If the tissue looks unusual but your provider told you to expect that appearance, don't let the look of the wound alone convince you something has gone wrong.
Post-Frenectomy Exercises for Infants
Parents often expect infant frenectomy exercises to feel technical. They don't need to. The best routines are brief, consistent, and calm.
The strongest evidence in the material we have points to this: the incidence of tongue-tie readhesion can reach 33.5% without exercises, but diligent stretching can reduce the need for a revision procedure from 37% down to just 5.6%. In one study, infants in the stretching-adherent group had a 0% rate of persistent feeding difficulties post-surgery (PMC study on postoperative exercises and outcomes).
That doesn't mean parents need to perform aggressive maneuvers. It means the healing site needs consistent, skillful attention.
For families considering the procedure itself, a pediatric dental overview of infant and child tongue-tie treatment options can help frame where exercises fit into the bigger plan.
A gentle routine works better than a perfect one
Attach the exercises to something you're already doing, such as a diaper change, a feed, or a nap transition. That lowers the chance you'll forget and helps your baby predict what comes next.
This visual shows the sequence in a parent-friendly way:
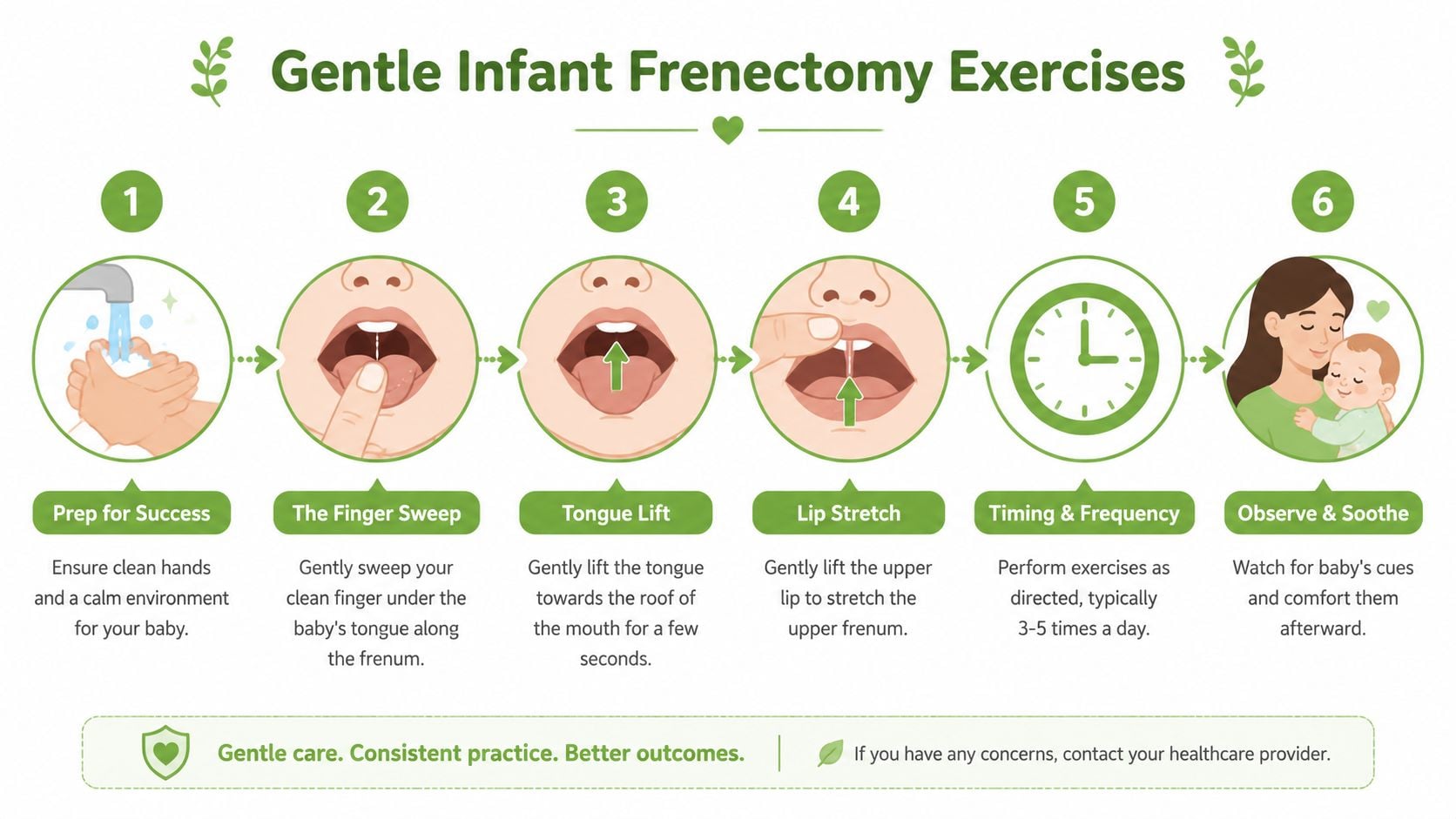
The main infant stretches
The following names are easier for families to remember than technical labels, but they map closely to common post-release movements.
Swoop and lift
Place a clean finger under the tongue and gently glide to the release site. Lift just enough to open the area and prevent the tissue edges from settling back together too tightly.
Why it helps: this is the movement that most directly addresses reattachment risk after a tongue release.
Diamond check
When the tongue lifts, many providers want caregivers to briefly expose the open release area. The purpose isn't to force a deep stretch. It's to make sure the space is staying open during early healing.
Why it helps: parents can see whether the site still opens well or whether movement is becoming restricted.
Fingertip roll
Using a clean fingertip, make small, controlled rolling motions over the release area, as instructed by your provider.
Why it helps: this can help keep the healing tissue pliable rather than stiff.
Lip lift
For an upper lip release, gently lift the lip upward to keep the area mobile and help the lip flange more easily during feeding.
Why it helps: babies often need that flexibility for a comfortable latch.
A practical demonstration can help some families understand the pacing and hand placement better than written instructions alone:
Frequency and technique
One published protocol identified 6 to 8 sessions daily over 15 days as the most effective approach, with each movement held for 5 to 10 seconds and performed slowly to prevent tissue reattachment (PubMed summary of postoperative lingual frenotomy regimen). A step-by-step pediatric exercise guide also describes tapering from 6 to 8 times daily in the first phase to 3 to 4 times daily later in recovery, with each session kept brief (Floss Academy infant frenectomy exercise guide).
What helps parents do this consistently
- Wash hands first: Confidence starts with a clean, simple setup.
- Use one cue phrase: Something like “open, lift, soothe” helps keep the sequence consistent.
- Keep sessions short: Lingering usually makes babies more upset.
- Finish with comfort: Feeding, skin-to-skin, rocking, or holding matters.
A baby doesn't need a tense parent with perfect technique. A baby needs a calm adult doing the right movement consistently.
Tongue Mobility Drills for Children and Adults
Older children and adults usually don't need the same kind of passive aftercare that infants do. They need retraining.
The key issue is compensation. After years of restricted movement, the tongue may have learned to stay low, push forward, twist, or recruit the jaw and neck to do jobs it couldn't do efficiently on its own. A release changes the anatomy, but it doesn't erase those habits overnight.
A 2025 study in PMC notes that for adults and teens, a frenectomy alone “might not yield desired effects” because entrenched muscle memory patterns persist, and the focus of therapy should be “kinesthetic awareness rather than speech improvement” (PMC article on adjunctive kinesthetic therapy after frenectomy).
If you're working on these patterns in a structured program, these kinds of orofacial myofunctional therapy exercises are the broader category your provider may draw from.
What older patients are really training
Children old enough to follow directions, teens, and adults benefit when they understand the target of each drill.
They're usually working on:
- Tongue elevation without jaw thrust
- Lateral control without lip pulling
- Steady oral rest posture
- Functional swallowing with less compensation
- Awareness of where the tongue is in space
Drills that build useful control
Spot hold
Place the tongue tip on the spot just behind the upper front teeth, then hold it there while the rest of the tongue broadens upward as much as possible.
Why this drill matters: it starts teaching a more stable oral rest position and cleaner elevation.
Roof press
Press the full tongue gently into the palate, not just the tip. Hold the contact while keeping the jaw quiet.
What to watch for: many adults think the whole tongue is up when only the tip is up. A mirror helps.
Tongue pops
Suction the tongue to the palate and release it with a pop. Keep the lips soft and the jaw from overworking.
Why it helps: this improves suction control and coordinated elevation.
Cheek sweeps
Move the tongue into one cheek, then the other, with deliberate side-to-side control.
Why it helps: this trains lateral mobility and exposes asymmetry quickly.
Controlled extension and return
Stick the tongue out straight, then draw it back in without dropping it heavily to the floor of the mouth.
What this teaches: smooth excursion and retraction without strain.
How to practice without reinforcing bad habits
Adults often try too hard. That creates tension and defeats the purpose.
Use this checklist:
| Focus | Better choice | Less helpful choice |
|---|---|---|
| Effort | Gentle, precise motion | Max force |
| Feedback | Mirror and body awareness | Guessing |
| Repetition | Short, regular practice | One long session |
| Goal | Cleaner movement | Bigger movement at any cost |
If your neck tightens, your jaw juts, or your lips grip during a tongue drill, the tongue isn't doing the job independently yet.
For children, turn these into games. “Can your tongue find the spot?” works better than a lecture. For adults, accuracy matters more than speed. Slow practice is often what finally reveals the old compensation pattern.
Your Recovery Timeline and When to Seek Help
A parent often calls our clinic on day three and says the same thing: “It looked better yesterday, and today it looks white and tighter.” That pattern can be normal. Early frenectomy healing often looks alarming before it looks better, especially if you are checking the area closely several times a day.
A better question than “How long does healing take?” is “What should I expect at this stage, for this age group?” Infants need wound care and feeding observation. Older children and adults need that, plus neuromuscular retraining so the tongue does not return to its old compensation pattern.
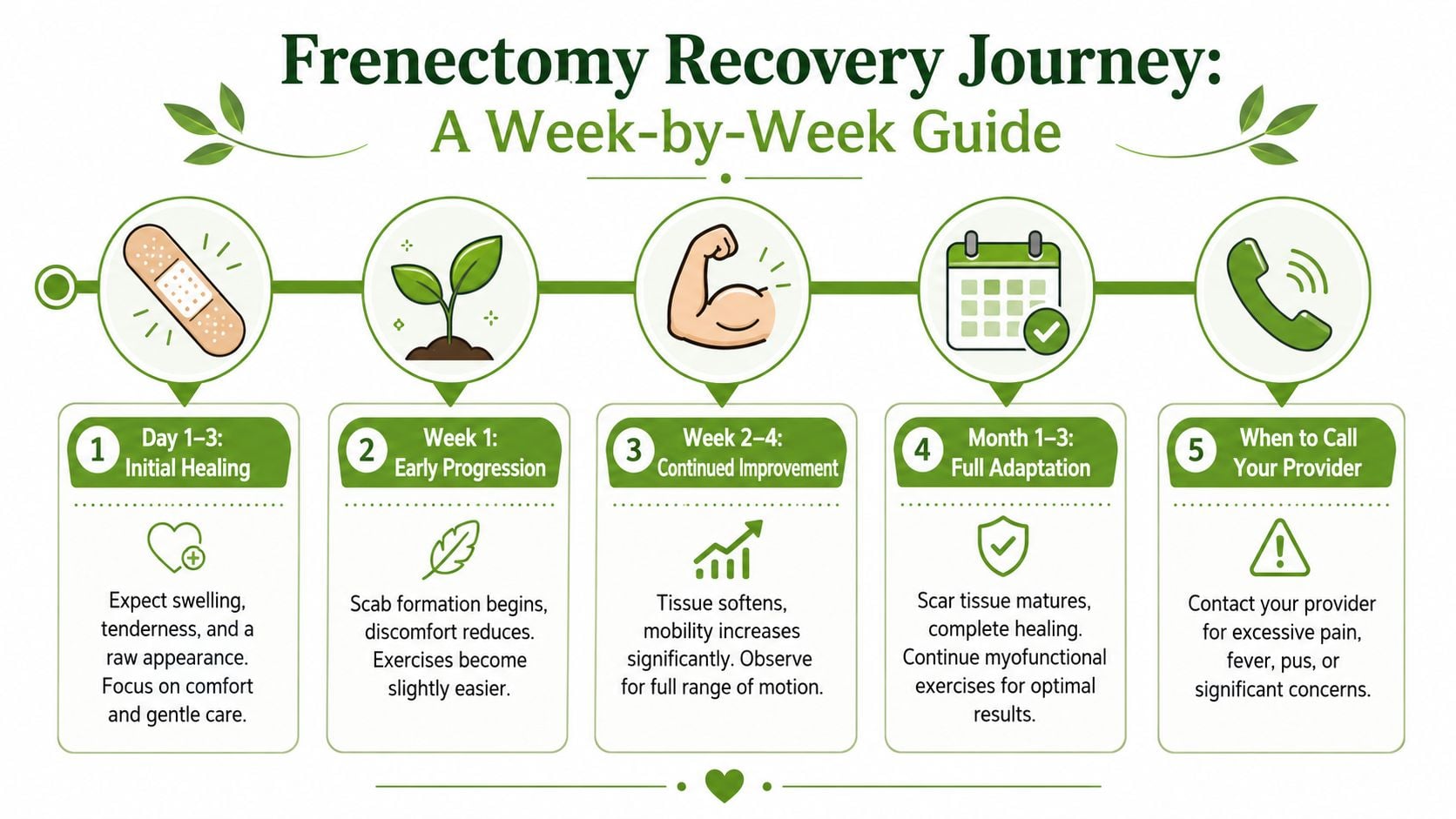
Days 1 to 5
The site may look open, white, or yellow. That appearance is usually part of normal healing, not infection by itself. Infants may be fussier with stretches or feeds. Children and adults often notice soreness, awkward tongue movement, and fatigue with exercises.
During this phase, the goal is simple. Keep the area mobile without turning every session into a struggle.
Watch for:
- a gradual return of comfortable movement
- the ability to complete prescribed exercises without increasing distress each day
- feeding that is stable or improving in infants
- speech and saliva control that feel clumsy but not progressively worse in older patients
Days 5 to 14
This is the period when families and adult patients can get mixed signals. The wound often looks smaller, but the tissue is actively contracting and remodeling. Tongue motion may feel tight in the morning and better later in the day.
For infants, continue the aftercare plan exactly as prescribed by the treating provider. For children and adults, this is often the point where movement quality matters more than force. A tongue that reaches higher with a quiet jaw is healing more usefully than a tongue that pushes hard while the neck and lips tense.
If jaw guarding starts to show up, some adults also notice temporomandibular joint discomfort. That usually means the tongue is still borrowing help from nearby muscles instead of working independently.
Weeks 2 to 4
Surface healing is usually well underway by now, but function is still catching up. This matters most for older children and adults. A release changes the tissue. It does not automatically teach better rest posture, cleaner swallowing, or efficient tongue elevation.
That is why many patients benefit from orofacial myology treatment and movement retraining during this stage. The work shifts from protecting the wound to building reliable patterns that hold up during eating, speaking, and rest.
Normal healing signs
These findings are common during recovery:
- white or yellow healing tissue
- mild tenderness that gradually improves
- temporary fussiness during infant aftercare
- temporary speech awkwardness or tongue clumsiness
- day-to-day fluctuation, with overall progress across the week
Call your provider promptly if you notice
- pain that is getting worse instead of easing
- fever
- pus or a foul odor
- significant swelling
- bleeding that does not stop as instructed
- an infant who refuses to feed and does not settle
- a clear drop in mobility after it had started to improve
One practical rule helps. Look for the overall trend, not a perfect day. If function is slowly improving, healing is usually on track. If symptoms are intensifying, feeding is deteriorating, or movement is shrinking, the site needs a closer look.
How Myofunctional Therapy Enhances Healing
A release solves a structural problem. It doesn't automatically solve a functional one.
That's where many patients get stuck. The tissue is no longer tethered in the same way, but the person still swallows with compensation, rests with the tongue low, breathes through the mouth, or recruits the jaw and neck when the tongue should be doing the work.
Some clinicians have questioned whether simple stretching alone is enough. A 2024 AAP review, as summarized in a discussion of the evidence, noted a lack of evidence that simple stretching alone improves outcomes, and some practitioners have raised concerns that aggressive manual stretching may create oral aversion or trauma. That line of thinking supports the role of functional activities, which is the core of myofunctional therapy (discussion referencing the AAP review and functional activity approach).
What therapy adds beyond wound care
Myofunctional therapy addresses the habits that existed before surgery and the new patterns needed after it.
That usually includes:
- Oral rest posture: where the tongue, lips, and jaw settle when you're not eating or speaking
- Swallowing coordination: reducing thrusting, grimacing, or compensatory head movement
- Breathing support: helping oral posture and nasal breathing work together
- Muscle balance: decreasing unnecessary strain in the face, jaw, and neck
This is especially important in older children and adults, where years of adaptation can create secondary issues. Some patients also notice that unresolved oral tension overlaps with jaw symptoms. If jaw strain is part of the picture, a resource on temporomandibular joint discomfort can help patients understand how muscle habits and joint symptoms may connect.
Why personalized guidance matters
The right post-frenectomy plan isn't just a list of tongue movements. It matches the patient's age, anatomy, symptoms, and compensations.
An infant may need caregiver-led wound management and feeding support. An adult may need mirror drills, swallow retraining, and coaching to stop using the jaw as a substitute for tongue elevation. That difference is why a broader explanation of what orofacial myology is can be useful for patients who want to understand why therapy is often paired with a release.
Surgery creates access. Therapy teaches the body what to do with that access.
When that pairing is done well, frenectomy exercises stop feeling like an isolated task. They become part of a larger recovery process that protects healing, restores movement, and supports comfortable function over time.
If you're dealing with tongue restriction, jaw tension, sleep-disordered breathing, or post-frenectomy recovery questions, Pain and Sleep Therapy Center offers interdisciplinary care that looks beyond the procedure alone. Their team works with infants, children, and adults to address function, breathing, oral posture, and long-term healing so patients can move from temporary relief toward lasting change.



