
Your partner snores every night, but laughs it off. Your child sleeps with their mouth open and always seems congested. You wake up after a full night in bed and still feel wrung out, foggy, and oddly tense in your jaw.
A lot of people treat those signs as separate problems. Snoring is just noise. Mouth breathing is just a habit. Jaw pain is just stress. Poor sleep is just part of getting older or being busy.
Sometimes that's true. But sometimes those everyday complaints point to the same underlying issue: restricted airflow. When the body has trouble moving air smoothly, especially during sleep, it can show up in ways that don't look dramatic at first. The clues may be loud, like gasping or choking sounds. They may also be quiet, like restless sleep, dry mouth, headaches, or a child who never seems settled at night.
That's why understanding airway obstruction symptoms matters. It helps you tell the difference between a nuisance, a chronic breathing problem, and a true emergency.
Is It More Than Just Noisy Breathing
A common pattern goes like this. An adult starts snoring more often, wakes with a dry mouth, and feels tired despite spending enough time in bed. Over time, they may notice jaw tightness, clenching, or morning headaches. They may not think “breathing problem.” They think stress, bad sleep posture, or getting older.
Parents often see a different version. Their child sleeps noisily, breathes through the mouth, tosses around, and seems cranky or unfocused during the day. Some children struggle with restless sleep for so long that the family starts to see it as normal.
It often isn't.
Breathing should be quiet, easy, and efficient. When air has trouble moving through the nose, throat, or lower airways, the body compensates. A person may open the mouth, shift the jaw, tense neck muscles, snore, gasp, or sleep lightly instead of soundly. Over time, those patterns can affect energy, concentration, pain levels, and sleep quality.
Practical rule: If a breathing sound repeats night after night, or if poor sleep comes with fatigue, dry mouth, headaches, or jaw discomfort, it deserves attention.
Some people describe a feeling that they “can't get a satisfying breath,” especially at rest or when trying to fall asleep. That experience overlaps with what many patients call air hunger symptoms. It doesn't always mean a dangerous blockage in that moment, but it can be an important clue that breathing mechanics or airway function need a closer look.
Noisy breathing is one sign. It's not the whole story. Airway problems can be loud, subtle, chronic, or sudden. The key is recognizing the pattern early instead of waiting for it to become impossible to ignore.
Decoding the Signs of Airway Obstruction
Some signs are easy to hear. Others are easier to see. A few are mostly felt in the body as poor sleep, fatigue, or a sense that breathing never seems fully effortless.
This visual helps organize the big picture.
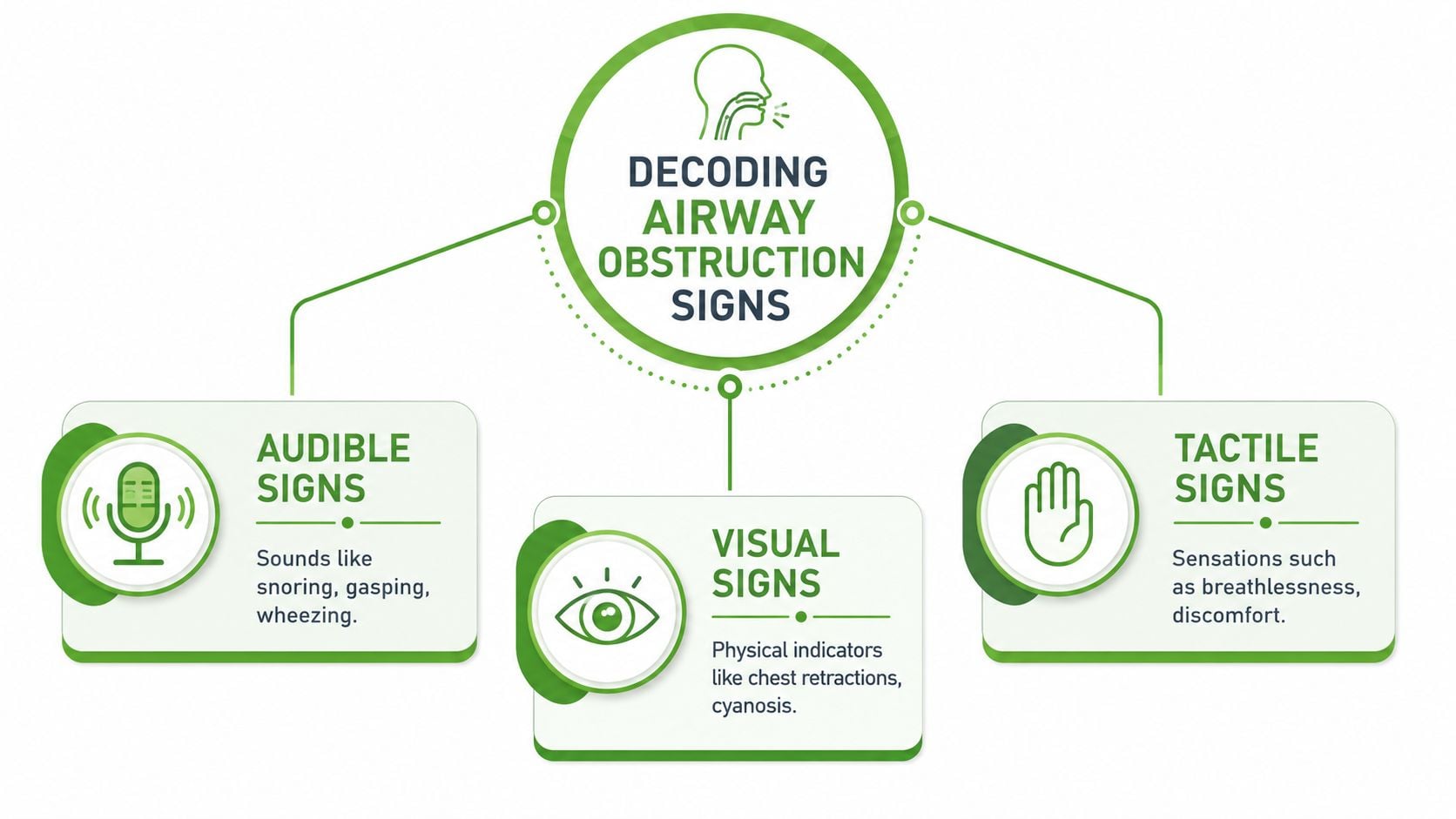
Audible signs
The sound of breathing can offer a clue about where the problem is happening.
- Snoring often points to vibration and narrowing in the upper airway during sleep.
- Stridor is a harsher, high-pitched sound that often suggests upper-airway narrowing.
- Wheezing is more of a whistling sound and is usually linked with lower-airway narrowing.
- Gasping, gurgling, or choking sounds suggest airflow is being interrupted more significantly.
A simple way to think about it is location. If the sound seems louder in the throat or neck, the upper airway may be involved. If it sounds more like a whistle coming from the chest, lower-airway narrowing becomes more likely.
Clinical guidance notes that the way obstruction sounds and looks can help reveal its location and cause. Upper-airway obstruction may cause noisy breathing, accessory muscle use, and tracheal tug, and children may be affected by anatomy such as a large tongue, enlarged adenoids or tonsils, or laryngomalacia, as described in upper-airway obstruction guidance during anesthesia.
Visual signs
What you see matters just as much as what you hear.
- Mouth breathing during the day or sleep
- Chest retractions or chest-wall recession, where the skin pulls inward with breaths
- Accessory muscle use, such as visible neck strain while breathing
- Tracheal tug, where tissues at the lower neck pull inward
- Restless sleep, frequent position changes, or sleeping with the head extended
- Bluish skin or lips, which is an emergency sign
Children with disrupted breathing often don't present like tired adults. Some become hyperactive, irritable, or hard to settle. If you're trying to sort out whether a child's poor sleep may relate to breathing, this page on child sleep apnea symptoms can help connect the dots.
A short video can make these distinctions easier to recognize in real life.
Felt signs
Not every airway issue announces itself with dramatic noise. Sometimes the body tells the story in less obvious ways.
| What a person feels | Why it may matter |
|---|---|
| Morning headache | Sleep may be fragmented, with poor nighttime breathing |
| Dry mouth on waking | Mouth breathing may be replacing nasal breathing |
| Daytime fatigue | Sleep quality may be poor even if sleep time seems adequate |
| Difficulty concentrating | Repeated nighttime breathing disruption can leave the brain under-rested |
| Jaw soreness or clenching | The body may be bracing or repositioning during sleep |
Noisy breathing gets attention. Quiet exhaustion, jaw tension, and restless sleep often get dismissed, even when they come from the same airway problem.
Age changes the pattern
Infants may show trouble feeding, noisy breathing, or poor coordination during sucking and breathing. Children may mouth-breathe, snore, sleep restlessly, or seem wired and irritable rather than sleepy. Adults may notice snoring, unrefreshing sleep, jaw pain, chronic fatigue, or a growing sense that sleep isn't restoring them.
That's one reason generic symptom lists often fall short. They don't always explain that airway obstruction symptoms can look different depending on age, anatomy, and whether the narrowing is happening in the nose, throat, or lower airways.
Grading Symptom Severity From Mild to Emergency
A parent hears soft snoring every night and assumes it is harmless. An adult wakes with jaw soreness, dry mouth, and a foggy head, then pushes through the day. These signs may sit on the mild end of the spectrum, but they still matter because they can be early clues that the airway is not staying open as easily as it should.
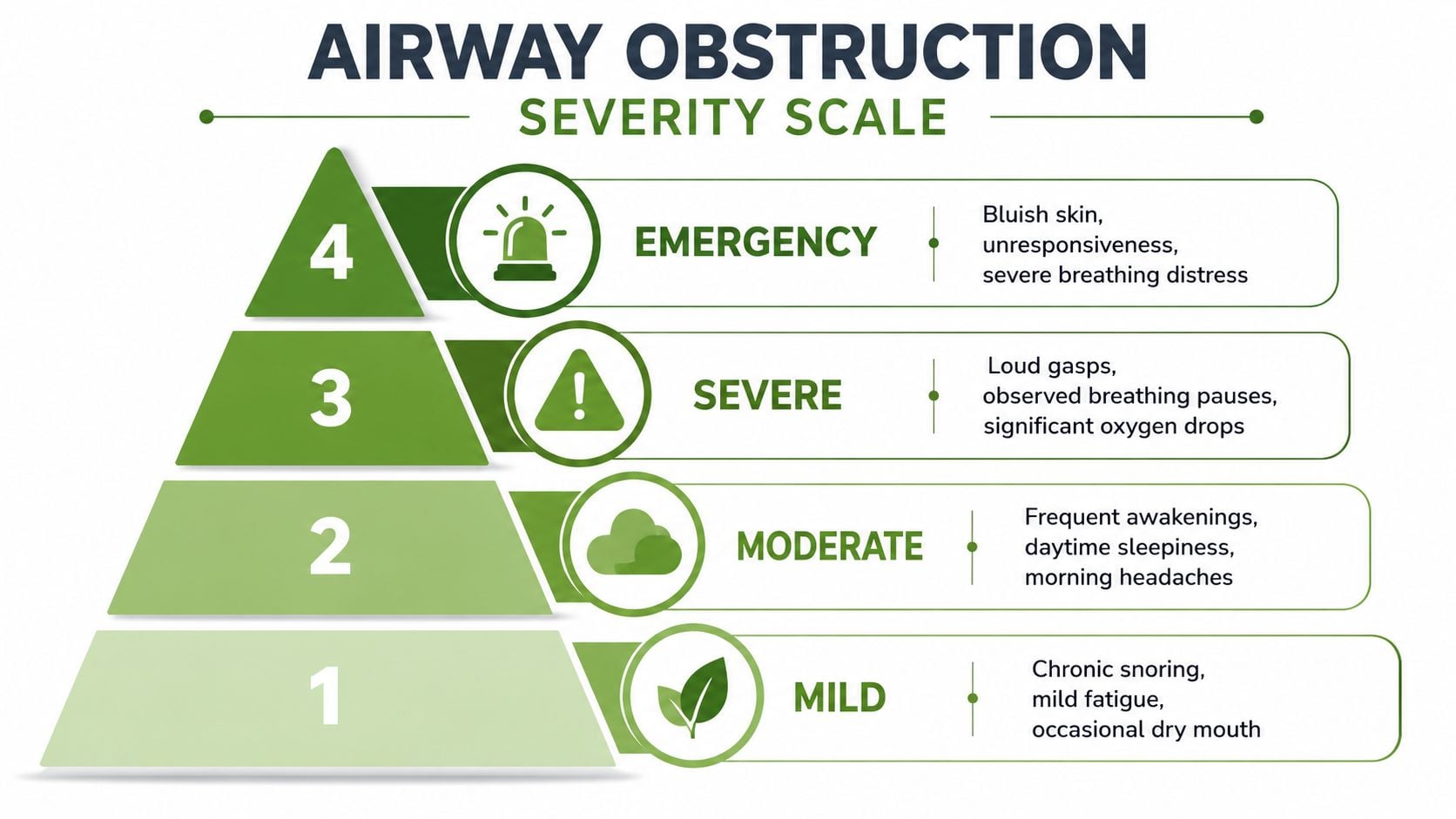
Mild and chronic signs
Mild symptoms are easy to dismiss because they often look familiar. Snoring, mouth breathing, restless sleep, waking with a tight jaw, or feeling only partly refreshed can become a person's “normal.”
That does not make them harmless.
A partly narrowed airway works like a bent straw. Air still moves, but the body has to work harder to pull it through. Over time, that extra effort can show up as poor sleep quality, clenching, morning discomfort, and low energy. In children, the pattern may look like light snoring, open-mouth posture, or sleep that never seems fully settled.
Moderate patterns that deserve evaluation
Moderate symptoms start to affect daily life in a clearer way. Sleep may be broken by frequent waking, tossing, gasping, or pauses in breathing noticed by a bed partner or parent. Daytime consequences become harder to ignore, including sleepiness, headaches on waking, irritability, trouble focusing, or behavior changes in a child.
This is also the stage where the “hidden” symptoms in this article deserve attention. Jaw pain, tooth grinding, poor oral posture, and chronic mouth breathing are not separate from the airway conversation. They can be part of the body's attempt to create space for airflow, especially during sleep.
When symptoms reach this level, an evaluation can help sort out whether the problem is coming from the nose, tongue position, jaw structure, throat tissues, or sleep-related collapse.
Severe and emergency symptoms
Severe symptoms mean airflow may be restricted enough to threaten oxygen delivery or rapid worsening. At that point, the question is no longer whether the pattern is affecting sleep. The question is whether breathing is safe right now.
Emergency warning signs include:
- Struggling to breathe
- Trouble speaking because breathing is difficult
- Noisy breathing that is getting worse quickly
- Blue lips or blue skin
- Confusion
- Loss of responsiveness
Cleveland Clinic notes that partial airway obstruction can cause wheezing, stridor, gurgling, snoring, or difficulty breathing or speaking, while blue discoloration, confusion, and loss of consciousness are danger signs, as described in this airway obstruction emergency overview.
If a child is working hard to breathe, or an adult cannot speak normally and is not moving air well, get emergency help right away.
A simple way to decide
A practical guide helps:
- Monitor closely if symptoms are mild but keep happening, especially snoring, mouth breathing, jaw tension, or restless sleep.
- Schedule an evaluation if sleep is regularly disrupted, fatigue persists, breathing pauses are noticed, or symptoms are affecting mood, focus, pain, or behavior.
- Seek emergency care now if breathing is labored, speech is limited, lips turn blue, or consciousness changes.
Severity is not only about how loud or dramatic a symptom seems. Frequency matters. Sleep disruption matters. Daytime function matters. A quiet pattern that shows up night after night can still point to a meaningful airway problem.
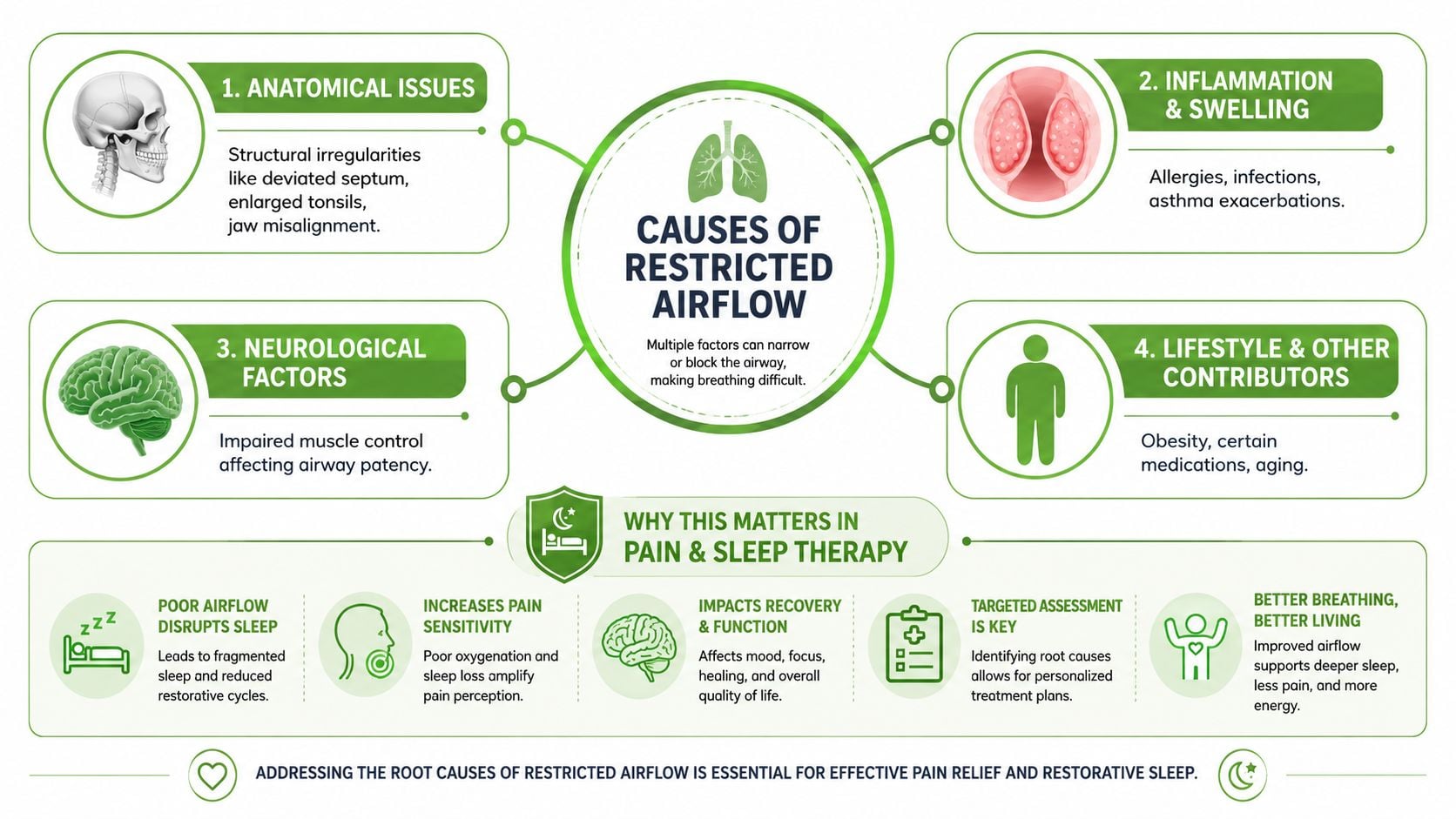
The Hidden Causes Behind Restricted Airflow
A restricted airway often builds slowly. A child snores and seems restless. An adult wakes with jaw pain, dry mouth, or a headache and assumes stress is the whole story. These symptoms can look unrelated, yet they often point to the same problem. Air is not moving as freely as it should.
The airway works like a flexible tube supported by bone, soft tissue, muscle tone, and posture. If one part narrows, the whole system has to compensate. That is why airway obstruction is not only about loud breathing. It can show up as poor sleep, clenching, mouth breathing, attention problems, or morning facial tension.
Sleep-related collapse
During sleep, the muscles that help hold the airway open relax. In some people, the upper airway becomes too narrow and partly collapses again and again. That pattern is common in obstructive sleep apnea.
The result is often more than snoring. A person may gasp, grind their teeth, clench their jaw, toss and turn, or wake feeling as if they never reached deep rest. Bed partners often notice the breathing changes first. Parents may notice that a child sleeps in odd positions, kicks the covers off, or seems hard to wake in the morning.
Poor sleep is often the downstream effect. The breathing problem comes first.
Nasal blockage and mouth breathing
The nose is the preferred path for airflow. It filters particles, humidifies air, and helps the tongue and lips stay in a more stable resting position. When nasal breathing is limited by congestion, swelling, allergies, or narrow nasal passages, the body often switches to mouth breathing just to keep air moving.
That workaround can create other problems. Open-mouth posture tends to lower the tongue, dry the mouth, and change how the jaw rests. During sleep, that lower tongue posture can leave the throat less supported. In children, long-term mouth breathing may also affect facial growth and sleep quality. In adults, it may show up as snoring, dry mouth, fatigue, or worsening jaw tension.
Jaw position and TMJ strain
Jaw position changes airway space. If the lower jaw sits farther back, shifts unevenly, or is under constant strain from clenching, the tongue may have less room and the airway behind it may narrow.
This is one reason jaw pain and breathing symptoms can travel together. A person may come in focused on TMJ pain, popping, tooth wear, or morning soreness, while the larger issue is nighttime airway stress. At centers such as the Pain and Sleep Therapy Center, clinicians pay close attention to this overlap because the jaw is not separate from breathing. It is part of the support system around the airway.
The body sometimes responds to a threatened airway by tightening nearby muscles. That protective effort can leave the jaw and face overworked by morning.
Tongue posture and tongue-tie
The tongue needs space and mobility to rest against the palate and support healthy oral function. If tongue movement is restricted, or if the tongue consistently rests low in the mouth, airway support may be less stable.
In infants, a tongue-tie may affect latch, feeding, and early oral function. In older children, it may contribute to open-mouth posture, messy swallowing patterns, or restless sleep. In adults, poor tongue posture can overlap with snoring, dry mouth, clenching, and narrow dental arches.
These patterns do not prove the same cause in every person. They do show why symptoms that seem minor or unrelated deserve a closer look.
A restricted airway often reflects both structure and function. Bones, soft tissue, tongue posture, and breathing habits all matter.
Why root cause matters
Treating the loudest symptom alone can miss the actual driver. A decongestant may not solve a jaw-based airway issue. A night guard may protect teeth but not explain why clenching is happening. A parent may hear “behavior problem” when chronic sleep disruption is part of the picture.
That is why age and cause both matter. In children, enlarged tonsils, adenoids, tongue-tie, and poor oral posture may be more visible pieces of the puzzle. In adults, nasal blockage, jaw position, airway collapse during sleep, and TMJ strain may play a larger role. If you are trying to understand whether sleep apnea screening is part of the next step, this guide on how to diagnose sleep apnea at home explains what home testing can and cannot show.
A primary care study noted earlier also supports taking ongoing symptoms seriously. Airflow obstruction showed up often enough in routine adult care that it should not be dismissed as a rare finding.
How these causes overlap
Several problems can narrow the same airway at once.
- Structural narrowing may come from tonsils, adenoids, nasal anatomy, or jaw position.
- Functional problems may include low tongue posture, poor lip seal, or mouth breathing habits.
- Sleep-related muscle relaxation can let already crowded tissues narrow further.
- Inflammation or illness can make a mildly narrow airway much tighter.
That overlap explains why one person's snoring is mainly a nose problem, while another person's snoring is tied more closely to jaw position, tongue posture, or sleep-related collapse. The visible symptom may look the same. The cause underneath it may be very different.
How We Uncover the Root Cause
A thorough airway evaluation usually starts with the story. When did the symptoms begin? Do they happen during the day, at night, or both? Is the main issue snoring, fatigue, jaw pain, restless sleep, mouth breathing, feeding difficulty, or all of the above?
The next step is a focused exam. A clinician may look at nasal breathing, lip seal, tongue mobility, palate shape, tonsil size, jaw position, head and neck posture, and how the TMJ functions. These details matter because the airway isn't a single pipe. It's a system influenced by bones, soft tissues, muscles, and habits.
What clinicians look for
A thorough visit often includes attention to:
- Sleep clues such as snoring, witnessed pauses, gasping, dry mouth, and unrefreshing sleep
- Oral structure including palate shape, tongue posture, and room for the tongue
- Jaw mechanics such as clenching, limited opening, joint noise, or pain
- Breathing pattern including nasal versus mouth breathing at rest
If home screening is part of the conversation, this guide to how to diagnose sleep apnea at home can help you understand what screening can and can't answer.
Why diagnosis can't rely on a checklist alone
A symptom checklist is helpful, but it doesn't show why the airway is compromised. One person's snoring may relate mostly to nasal obstruction. Another person's may be tied more closely to jaw position or sleep-related throat collapse. A child's noisy breathing may stem from enlarged tonsils, tongue posture, or another anatomic factor.
Good diagnosis doesn't stop at “you snore.” It asks what is narrowing, when it narrows, and what the body is doing to compensate.
Sometimes that means referral for sleep testing or collaboration with other professionals. The goal is simple. Match treatment to the actual cause.
When to Seek Help A Clear Action Guide
Patients don't need more information. They need a decision.
Go to emergency care now
Seek immediate emergency help if breathing is visibly hard work, if the person can't speak normally because they can't move enough air, or if the lips or skin look blue. Confusion, faintness, or loss of responsiveness also means urgent care right away.
For children, this threshold should be low. If a child is struggling to breathe, retracting strongly, or changing color, don't wait to see if it passes.
Start with primary care
Primary care is a reasonable first stop when symptoms are new, unclear, or tied to a broader illness. That includes ongoing cough, recurrent wheezing, congestion with breathing complaints, or a recent change in breathing quality after infection or allergy flare.
A primary care clinician can help sort out whether the issue sounds more like upper-airway narrowing, lower-airway disease, infection, inflammation, or something that needs specialist input.
Book a specialist evaluation for persistent or complex patterns
Specialist assessment makes sense when the problem is chronic, sleep-linked, or tied to anatomy and function.
Consider this route if you notice:
- Nightly snoring or gasping that keeps recurring
- Morning headaches or dry mouth that suggest sleep breathing may be poor
- TMJ pain, jaw clenching, or facial tension that seems worst after sleep
- Mouth breathing in a child that has become the norm
- Feeding or latch concerns in infants when tongue movement seems limited
- Restless sleep and daytime behavior changes that don't fit the amount of sleep on paper
The reason to seek help isn't fear. It's clarity. When chronic airway symptoms are left vague, people often bounce between labels such as poor sleep, stress, sinus issues, or behavior problems without addressing the breathing pattern underneath.
Your Path to Better Breathing and Restful Sleep
The encouraging part is that many airway-related problems are treatable once the cause is identified. Some people need sleep-focused treatment. Others need work on nasal breathing, oral posture, jaw mechanics, or tongue function. Children may need a more developmental and collaborative approach than adults do.
That's where targeted care matters. Depending on the findings, treatment may include orofacial myofunctional therapy to retrain tongue posture and oral muscle patterns, Buteyko breathing to improve breathing mechanics, non-surgical TMJ care to reduce strain and improve jaw position, or collaborative pediatric care for feeding and tongue-tie concerns. In some cases, families also explore orthodontic treatment for airway issues when jaw and facial development are part of the airway picture.
The Pain and Sleep Therapy Center addresses airway dysfunction, sleep-disordered breathing, TMJ problems, facial pain, and pediatric oral function with a root-cause approach rather than treating each symptom as a separate problem.
If you recognized yourself or your child in these patterns, don't dismiss them because they've become familiar. Snoring, jaw pain, mouth breathing, restless sleep, and constant fatigue can all be signals that the airway needs closer attention. Better breathing often starts with understanding why the body has been working so hard in the first place.
If you're ready to look beyond symptom management, visit Pain and Sleep Therapy Center to learn more, take the sleep quiz, or schedule a consultation.



