
A sip of coffee. A light breeze. The edge of a toothbrush. For some people, one of those tiny moments sets off a violent burst of facial pain that feels completely out of proportion to the trigger. It can be so fast and so sharp that people stop mid-sentence, freeze at the sink, or avoid eating on one side of the mouth because they're afraid of what happens next.
That fear is part of the condition. Facial neuralgia doesn't just hurt. It trains you to anticipate pain before daily life even begins.
The good news is that severe facial nerve pain is no longer a mystery condition managed only with trial and error. We understand much more about how these nerves misfire, why standard painkillers often fail, and which treatments can calm the nerve, reduce triggering, and in some cases address the deeper reason the pain keeps returning. If you're looking for practical, evidence-based facial neuralgia pain relief, there are more options than “take stronger pills” or “go straight to surgery.”
That Sudden Shock of Pain Understanding Your Experience
Many patients describe the first attack the same way. They think something catastrophic just happened. A cracked tooth. A hidden infection. A sudden dental disaster. Then the pain vanishes as quickly as it arrived, only to come back the next time they talk, chew, shave, wash their face, or step outside into cold air.
What makes facial neuralgia so unsettling is the mismatch between trigger and reaction. A normal sensory event produces an extreme pain response. That can make people feel isolated, especially when the face looks normal from the outside and friends or family don't understand why a kiss on the cheek or a gust of wind could be unbearable.
Why the pain feels so disruptive
The face is crowded territory. Nerves, muscles, jaw joints, teeth, sinuses, and airway structures all live close together. When one part starts sending distorted pain signals, the whole system can feel threatened. Eating becomes guarded. Sleep gets lighter. Jaw muscles tighten. Anxiety climbs because you never know when the next strike will hit.
Facial neuralgia is severe, but it is treatable. The most important step is getting the pain classified correctly instead of assuming every facial pain problem is “just TMJ” or “just dental.”
Some people feel only brief electric shocks. Others also develop lingering soreness, burning, or muscle guarding between attacks. Both patterns matter. They influence which treatments are likely to help and which ones may waste time.
Relief starts with the right frame
The first practical shift is this. Don't judge the seriousness of the condition by the size of the trigger. Facial neuralgia often behaves like an alarm system with the sensitivity turned too high. Once you understand that, the path to relief becomes clearer. The goal isn't to “tough it out.” The goal is to calm an overreactive nerve, reduce what keeps provoking it, and look for root causes that standard care sometimes misses.
What Is Facial Neuralgia and Why Does It Hurt So Much
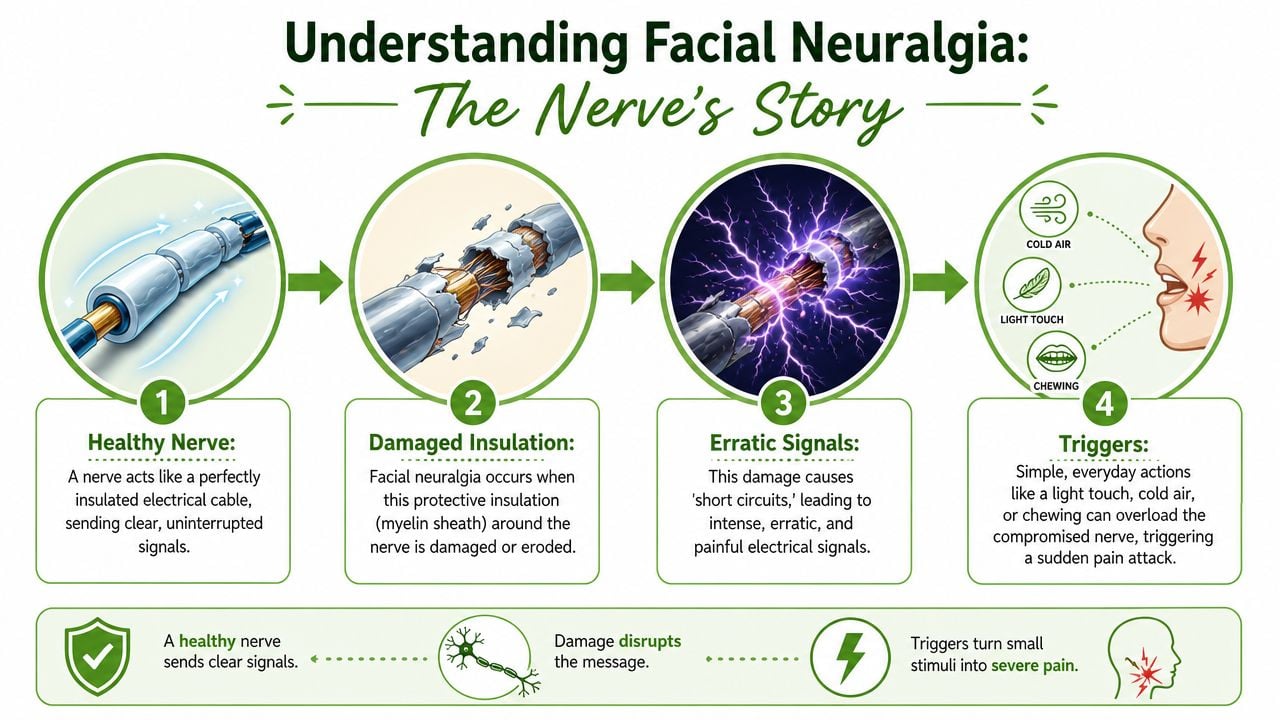
Facial neuralgia means pain generated by an irritated or damaged facial nerve. The best-known and most severe form is trigeminal neuralgia, which involves the trigeminal nerve. That nerve carries sensation from much of the face and also helps coordinate chewing.
A useful analogy is an electrical cord. A healthy nerve acts like a well-insulated wire. It transmits information cleanly. A neuralgic nerve behaves more like a frayed cord. The insulation is compromised, signals leak, and harmless input can trigger a painful short circuit.
The trigeminal nerve and its territory
The trigeminal nerve has three main branches. One serves the forehead and eye region, another the cheek and upper jaw, and another the lower jaw. That's why trigeminal neuralgia can show up in different parts of the face and why people sometimes confuse it with sinus trouble, tooth pain, or jaw pain.
If you want a broader review of how different pain patterns are sorted clinically, this overview of what causes facial pain is a useful starting point.
What usually goes wrong
Several problems can disturb the nerve's normal function:
- Compression: A blood vessel may press on the nerve and irritate it over time.
- Injury: Trauma, facial procedures, or dental treatment can leave a nerve more reactive.
- Disease-related change: Some neurological conditions can affect the nerve's protective covering.
- Post-inflammatory irritation: After infection or tissue inflammation, the nerve may stay hypersensitive.
The pain is intense because the trigeminal system is built to detect touch, temperature, and threat with extraordinary precision. When that system misfires, the brain receives an urgent danger signal even when the stimulus is minor.
Why ordinary pain medicine often disappoints
This is one of the hardest lessons for patients. Neuralgia isn't the same as a strained muscle or a bruised joint. Anti-inflammatory drugs and common pain relievers may help secondary soreness, but they often don't stop the core electric attack because the problem is faulty nerve signaling, not tissue inflammation.
Clinical perspective: When brushing your teeth triggers a jolt of pain, that points toward a nerve firing problem. It doesn't automatically mean the tooth is the source.
That distinction matters. Effective facial neuralgia pain relief starts with matching the treatment to the biology of the pain.
First-Line Medical Treatments for Pain Control
When trigeminal neuralgia is suspected, the standard first move is usually not an opioid, not a stronger anti-inflammatory, and not another round of general pain medicine. The most established first-line treatment is a group of anticonvulsant medications that calm abnormal nerve firing.
According to Mayfield Clinic's trigeminal neuralgia overview, about 80% of patients experience at least short-term pain relief with medication. That's why medication remains the usual starting point even though it's not the whole story.
Why anticonvulsants became the standard
Carbamazepine became the early benchmark because it can control pain in many patients during the initial stages of the disease. Over time, clinicians also began using oxcarbazepine, gabapentin, lamotrigine, and pregabalin when the first option didn't work well enough or caused side effects.
That shift matters historically. Treatment moved away from broad painkillers and toward medicines that target the nerve's abnormal firing pattern more directly.
What works and what often doesn't
A practical comparison helps:
| Approach | Typical role in neuralgia care | Main limitation |
|---|---|---|
| Anticonvulsants | Calm overactive nerve signaling | May lose effectiveness or cause side effects |
| General painkillers | May help associated soreness | Often weak against shock-like nerve pain |
| Repeated medication escalation | Sometimes necessary short term | Can miss an untreated driver of pain |
Medication can be highly useful, especially early. But it has trade-offs. Some patients get strong relief. Some get partial relief. Some feel sedated, foggy, or otherwise unable to tolerate the dose needed for control. Others improve at first, then notice the benefit fades or the attacks break through.
How to think about medication realistically
Medication is best viewed as a stabilizer, not automatically a cure. It can lower the volume on the nerve and create breathing room. That's valuable. It may also help clarify the diagnosis because true trigeminal neuralgia often responds in a recognizable way.
But if medication only partly helps, stops helping, or causes side effects you can't live with, that doesn't mean you've failed treatment. It means the treatment plan needs to widen. In practice, good care asks two questions at the same time:
- Is the nerve being calmed?
- Why is it still so easy to provoke?
That second question becomes especially important when pain is worse overnight, first thing in the morning, or during periods of poor sleep.
The Hidden Link Between Your Airway and Facial Pain
A pattern many people notice before anyone explains it is this. The face hurts more after a rough night of sleep. Morning pain is sharper. Snoring is louder. Jaw tension is worse on waking. They assume that's just stress or bad luck.
Sometimes it isn't.

Why nighttime breathing can change nerve pain
If breathing is repeatedly disrupted during sleep, the body doesn't spend the night in true repair mode. Instead, it cycles through strain. That can promote inflammation, fragmented sleep, mouth breathing, jaw muscle overuse, and a generally more reactive nervous system. In a patient who already has an irritable trigeminal nerve, that's a poor combination.
The overlooked question is not only “What medicine calms the nerve?” It's also “What keeps the nerve sensitized every night?”
A study discussed in this PMC article on obstructive sleep apnea and trigeminal neuralgia reported that 40% of patients with medication-resistant trigeminal neuralgia had undiagnosed obstructive sleep apnea, and their pain scores dropped by an average of 65% after non-surgical airway therapy. That is a meaningful signal that airway health can be part of real facial neuralgia pain relief, not just a side issue.
Clues that airway problems may be part of your case
Consider the airway more seriously if several of these fit:
- Morning worsening: Pain, jaw tightness, or headaches are worse when you wake up.
- Snoring or gasping: A bed partner notices noisy breathing or pauses in breathing.
- Dry mouth on waking: Mouth breathing overnight can dry tissues and strain the jaw and face.
- Poor sleep despite exhaustion: You're tired, but sleep doesn't feel restorative.
For readers who want a practical explanation of breathing retraining and oral posture, this guide on myofunctional therapy for mouth breathing is relevant because airway mechanics and facial tension often overlap.
What root-cause airway care can look like
Not every patient needs the same airway strategy. Evaluation may include sleep screening, breathing pattern assessment, oral posture review, and discussion of non-surgical options such as oral appliances or guided breathing work. A useful example of that broader model is airway care at Seven Oaks Dentistry, where dentistry and sleep-focused evaluation are considered together rather than as separate silos.
Later in the workup, it helps to see the breathing concepts visually:
Poor sleep doesn't just lower your pain tolerance. In some patients, disordered breathing may be one reason the nerve remains irritable in the first place.
A root-cause approach changes the plan. If sleep-disordered breathing is feeding the pain, adding more medication without addressing the airway may only give partial relief.
Advanced Therapies When Medication Is Not Enough
Once medication stops giving meaningful relief, treatment decisions need to become more precise. I frame the next step around the pain mechanism. Is the nerve being compressed, is the goal to interrupt pain transmission, or is the tissue around the nerve staying inflamed and irritable? Those are different problems, and they do not all respond to the same procedure.
A pinched electrical wire is a useful comparison here. If a blood vessel is pressing on the trigeminal nerve, the most logical fix is to relieve that pressure. If the nerve is firing abnormally and surgery is not a fit, some procedures reduce pain by disrupting the signal itself. If prior treatment failed and the area remains irritated, a restorative approach may deserve discussion.
The established procedural options
Specialists commonly discuss several categories of advanced care:
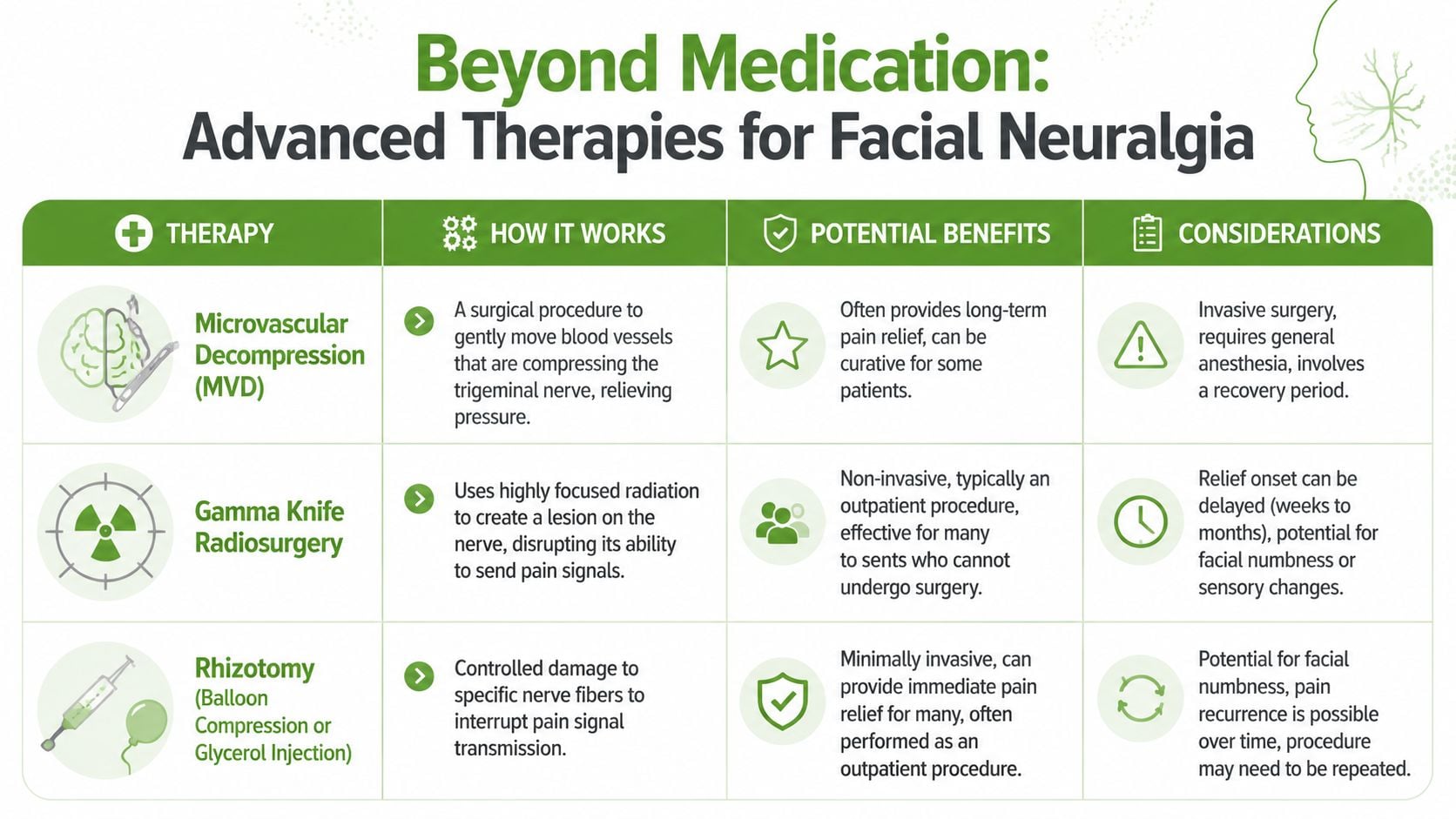
- Microvascular decompression: Best suited to cases where the history, exam, and imaging suggest vascular compression of the trigeminal nerve. The goal is to separate the vessel from the nerve and preserve nerve function.
- Gamma Knife radiosurgery: A non-incisional procedure that targets the nerve to reduce pain transmission over time.
- Rhizotomy procedures: These intentionally injure selected nerve fibers to lessen pain signaling.
- Nerve blocks or neuromodulation strategies: Used in selected patients to clarify the source of pain, reduce flare intensity, or help when symptoms do not fit a classic pattern.
These treatments can work very well in the right patient. The trade-offs are real. Surgery brings recovery time and procedural risk. Lesioning procedures can reduce pain, but they may also leave numbness, altered sensation, or pain recurrence later.
A comparison that matters in real decision-making
| Treatment direction | Primary goal | Common trade-off |
|---|---|---|
| Decompression | Relieve pressure on the nerve | Surgery and recovery |
| Lesioning | Interrupt pain transmission | Risk of numbness or altered sensation |
| Regenerative injection therapy | Improve tissue environment around the nerve | Still emerging and case selection matters |
That third category is often missing from standard facial neuralgia discussions.
Where regenerative medicine fits
Regenerative treatment follows a different logic. Instead of deadening the nerve or creating a controlled injury, it aims to improve the local environment around an irritated nerve. That approach can matter for patients who cannot tolerate more medication, want to avoid destructive procedures, or still have pain after surgery.
One option is Platelet-Rich Fibrin (PRF). Early clinical interest in PRF has grown because it may help calm irritated tissue around the trigeminal nerve in carefully selected refractory cases. The appeal is straightforward. The treatment is designed to support healing biology rather than shut the nerve down.
I discuss PRF cautiously with patients. It is not a replacement for a proper diagnosis, and it is not the first answer for clear vascular compression. It may be reasonable when medication side effects are limiting, when prior interventions did not hold, or when the exam suggests a persistent inflammatory component around the nerve.
Choosing based on the pain pattern
Exhaustion pushes some patients toward the quickest procedure on the menu. Fear pushes others to delay every procedural option, even when the anatomy strongly suggests a mechanical problem. Both reactions are understandable, but neither is a sound treatment strategy.
A better match looks like this:
- Compression pattern: Microvascular decompression may deserve serious consideration.
- Signal interruption needed, surgery not ideal: Gamma Knife or rhizotomy may be discussed.
- Medication intolerance, persistent irritation, or failed prior intervention: Regenerative care may be worth reviewing as part of a broader plan.
That broader plan matters. If poor sleep, airway strain, clenching, or facial muscle guarding are still feeding the nerve, even a technically successful procedure may leave partial relief on the table. Advanced care works best when the driver of the irritation has been identified, not just the pain signal.
For readers comparing broader nerve pain strategies beyond the face, this Shawnee patients' guide to nerve pain gives a helpful plain-language framework for thinking about conservative versus interventional care.
Practical Self-Care Strategies for Daily Relief
Self-care won't replace diagnosis or specialist treatment, but it can reduce how often the nervous system gets provoked. The key is to think less about “fixing the nerve at home” and more about reducing needless triggers while your treatment plan does the heavier work.
Reduce avoidable triggers
Start by identifying what reliably sets off attacks. Many people notice patterns only after they write them down for several days.
- Cold air exposure: Use a scarf or face covering outdoors if wind triggers pain.
- Chewing load: During flares, choose softer foods and avoid hard crusts, tough meats, or wide bites.
- Touch triggers: Switch to gentler face washing, softer toothbrushes, and slower shaving or skin-care routines.
- Temperature extremes: Very hot or very cold foods can provoke some patients.
A simple symptom log helps because “random pain” often turns out to have a rhythm.
Calm the surrounding muscles
Neuralgia and muscle guarding often feed each other. Once pain starts, the jaw, temple, neck, and cheek muscles may tense up defensively. That extra tension can make the whole face feel more fragile.
Try a brief downshift routine once or twice a day:
- Let your lips rest together lightly.
- Keep your teeth apart instead of clenched.
- Place the tongue gently on the roof of the mouth behind the front teeth.
- Breathe slowly through the nose if you can do so comfortably.
This won't treat the nerve directly. It can, however, reduce the muscular “brace response” that adds another layer of pain.
Use comfort measures carefully
Heat and cold can both help, but not in the same person and not in the same way.
- Gentle warmth: Often useful when muscles around the jaw and cheek feel tight.
- Cold packs: Sometimes helpful for secondary inflammation, but they can trigger neuralgia in cold-sensitive patients.
- Short applications: Test briefly rather than committing to a long session that may backfire.
If a comfort measure makes the pain feel electrically sharper, stop. With neuralgia, more intensity isn't better therapy.
Protect sleep and daily rhythm
Because the nervous system is easier to trigger when you're run down, daily rhythm matters. Aim for regular mealtimes, consistent sleep timing, and less late-evening jaw strain from gum chewing, heavy snacking, or prolonged clenching during stress.
People often underestimate stress because they think of it as emotional only. In facial pain, stress also shows up physically. Pressed tongue posture, tight shoulders, shallow breathing, and jaw clenching all increase the background load on a sensitive system.
The goal of self-care is modest but important. Fewer avoidable flares. Less guarding. A more stable baseline between medical visits.
When and How to Consult a Facial Pain Specialist
Primary care and general dentistry can identify common causes of facial pain, but there's a point where continued trial and error becomes inefficient. If the diagnosis is unclear, the pain is escalating, or the treatment response doesn't fit the pattern, a facial pain specialist can narrow the field much faster.
Signs it's time to move beyond basic care
You should seek specialty evaluation if:
- Medication isn't working well enough: The pain breaks through, relief is short-lived, or side effects are hard to tolerate.
- The diagnosis keeps shifting: You've heard dental pain, sinus pain, TMJ, nerve pain, and stress without a clear unifying explanation.
- Sleep symptoms are present: Snoring, mouth breathing, poor sleep, or waking pain may be part of the puzzle.
- Jaw mechanics are involved: Clicking, locking, clenching, or chewing limitation may be amplifying the facial pain.
A facial pain workup should look beyond the nerve alone. It may include the bite, jaw joints, chewing muscles, oral habits, breathing pattern, and sleep history. That broader lens is often what separates temporary symptom management from a plan that fits the patient.
For patients who suspect jaw dysfunction is contributing, these dental solutions for TMJ symptoms offer a useful example of how mechanical jaw issues can overlap with head and face pain.
What a specialist visit should accomplish
A good consultation should answer practical questions:
- Is this trigeminal neuralgia or another facial pain condition?
- Are the muscles and jaw reacting to the pain, or helping drive it?
- Is poor airway function or sleep-disordered breathing worsening the pattern?
- Which options target the cause, not just the symptoms?
If you're trying to find the right level of care, this directory for a facial pain specialist near me can help you understand what to look for in a more focused evaluation.
If you're dealing with sudden shocks of facial pain, pain that resists medication, or symptoms that seem tied to sleep, jaw tension, or breathing, Pain and Sleep Therapy Center offers evaluation for facial pain, TMJ-related disorders, and sleep-related contributors in one clinical setting. The most useful next step is often not another generic pain treatment. It's a careful diagnosis that looks at the nerve, the jaw, and the airway together.



