
You may be reading this after an echocardiogram, a hospital visit, or a message in your patient portal that says EF 30%. In that moment, individuals often don't feel informed. They feel stunned. The number sounds precise, but it doesn't tell you, in plain language, what your heart is doing, why you may feel so tired, or what happens next.
A 30 ejection fraction is serious, but it is not the whole story of your health and it is not a verdict on your future. It's a measurement that helps your doctors understand how strongly your heart is pumping and how urgently it needs support. Once you understand what that number means, the path forward gets clearer.
What a 30% Ejection Fraction Really Means
Think of your heart's main pumping chamber, the left ventricle, like a strong hand squeezing water from a sponge. Ejection fraction, or EF, is the percentage of blood pushed out with each beat. It does not mean your heart is working only 30% overall. It means that with each squeeze, the ventricle is ejecting about 30 of every 100 milliliters of blood in that chamber.
The American Heart Association says a normal EF is 55% to 70%, 41% to 49% is mildly reduced, and values under 40% usually indicate heart failure or cardiomyopathy. A 30% EF falls into the severely reduced range, which signals a major loss of pumping efficiency (American Heart Association guidance on ejection fraction).
What that number means in everyday life
When the heart can't push blood forward efficiently, the body notices. Muscles may get less oxygen-rich blood during activity. The kidneys may hold on to more fluid. The lungs may feel the effects when blood backs up instead of moving forward smoothly.
That's why people with a 30 ejection fraction often describe a cluster of symptoms rather than one single problem. They may say:
- “I get winded faster.” Walking, climbing stairs, or carrying groceries may suddenly feel harder.
- “I'm exhausted, even when I slept.” Low output can leave you drained.
- “I don't feel like myself.” Brain fog, weakness, and reduced stamina are common ways patients describe it.
- “My body feels swollen or heavy.” Fluid retention can show up in the legs, ankles, or abdomen.
A 30% EF is a serious finding, but it also gives your care team something concrete to treat.
What it doesn't mean
It doesn't automatically tell you the cause. It doesn't tell you how you'll feel next month. And it doesn't mean nothing can improve. Many people live with a low EF while following a structured treatment plan, monitoring symptoms carefully, and making practical daily changes.
Doctors often classify a 30 ejection fraction as heart failure with reduced ejection fraction, often shortened to HFrEF. That term sounds frightening, but in clinical care it serves a useful purpose. It helps your team choose medicines, decide whether a device might help, and set up the right follow-up.
Common Causes of a Reduced Ejection Fraction
A low EF usually doesn't appear out of nowhere. It's often the result of damage, strain, or an underlying disease that weakens the heart muscle over time. Heart failure affects about 1.9% to 2.6% of U.S. adults overall, and prevalence is expected to rise to 8.5% among ages 65 to 70. Major cardiology groups classify 40% or less as reduced ejection fraction, which includes a 30 ejection fraction (2024 review in PMC on heart failure burden and EF classification).
Damage to the heart muscle
One common pathway is direct injury to the muscle itself.
A prior heart attack can leave part of the left ventricle scarred. Scar tissue doesn't squeeze like healthy heart muscle, so the pump becomes weaker. Coronary artery disease can also starve the heart of oxygen over time, especially if blood flow has been reduced for months or years.
Other forms of heart muscle disease can do the same thing. Some people develop a cardiomyopathy related to genetics, viral illness, inflammation, or past exposure to certain medications such as chemotherapy.
Long-term strain on the heart
Sometimes the muscle is not damaged first. It is overworked first.
If the heart has to push against high blood pressure for years, it can stiffen, enlarge, and eventually weaken. Faulty heart valves can also create extra workload. If blood leaks backward or the ventricle has to pump through a narrowed valve, the heart may gradually lose efficiency.
Here's a simple way to understand it:
| Pattern | What happens |
|---|---|
| Damage problem | Part of the heart muscle loses strength after injury |
| Pressure problem | The heart works against resistance for too long |
| Volume problem | The heart handles too much blood flow because of a valve issue |
Other medical contributors
A reduced EF can also show up alongside other conditions that affect the whole body. Rhythm problems, thyroid disease, heavy alcohol use, or untreated sleep-related breathing issues can complicate the picture. In some people, doctors can identify a clear cause quickly. In others, the workup takes time.
A useful question to ask early: “What does my cardiologist think caused my low EF in my case?” That answer shapes almost every treatment decision that follows.
If you've been told you have a 30 ejection fraction, the number matters. But the reason behind it matters just as much.
Recognizing Symptoms and Associated Health Risks
For many patients, the diagnosis starts making sense only after they connect the number to how they've been feeling.
You may have noticed that stairs feel steeper than they used to. Maybe you can still walk across a room, but carrying laundry leaves you short of breath. Maybe your shoes feel tighter by evening, or you need more pillows at night because lying flat feels uncomfortable. Some people find that pattern so common they start searching for terms like orthopnea and sleeping propped up on two pillows.
Why these symptoms happen
A weak left ventricle can create two problems at once. It may send less blood forward to the body, and it may allow pressure to build backward toward the lungs.
That combination often leads to symptoms such as:
- Shortness of breath during activity, when lying flat, or sometimes even at rest
- Fatigue and low stamina because tissues may not receive enough blood flow
- Swelling in the feet, ankles, legs, or abdomen when the body retains fluid
- Rapid or pounding heartbeat as the body tries to compensate
- Reduced exercise tolerance that feels out of proportion to your effort
Some people also develop coughing at night, poor sleep, or a restless feeling in the chest that's hard to describe.
The breathing connection many people miss
A severe reduction in pumping strength can affect breathing patterns during sleep. Severe HFrEF, as seen with an EF around 30%, often drives central sleep apnea and Cheyne-Stokes respiration because compromised pulmonary perfusion and delayed chemoreceptor feedback disrupt the body's normal breathing control.
That matters because sleep and heart function affect each other in both directions. If breathing becomes unstable overnight, sleep quality drops. Poor sleep can worsen fatigue, concentration, and quality of life. It may also make it harder to tell whether daytime exhaustion is coming from the heart, the lungs, or both.
If you're waking up gasping, noticing pauses in breathing, or feeling unrefreshed despite enough time in bed, tell your doctor. Those symptoms deserve attention, not guesswork.
Associated risks
Low EF isn't just about symptoms. It can also increase the chance of dangerous heart rhythms, fluid overload, and episodes where heart failure worsens quickly. That's one reason clinicians take a 30 ejection fraction seriously even when someone is still able to function day to day.
Call your care team promptly if breathing worsens, swelling jumps, or daily activities suddenly become much harder. Those changes often matter more than the number alone.
How Doctors Diagnose and Monitor Your Condition
Individuals typically first learn their EF from an echocardiogram, often called an echo. This is an ultrasound of the heart. It's painless, it doesn't involve surgery, and it lets doctors watch the heart chambers move in real time.
The core tests doctors use
An echo helps answer several questions at once:
- How well is the left ventricle squeezing
- Are the heart chambers enlarged
- Are the valves opening and closing properly
- Is there pressure or fluid change that suggests worsening heart failure
Sometimes doctors order a cardiac MRI, which can give very detailed images of the heart muscle. They may also use blood tests, rhythm monitoring, stress testing, or coronary imaging depending on what they suspect is causing the problem.
Why one number may differ from another
Patients often get confused when one test says one thing and another report seems slightly different. That confusion is understandable.
EF is most commonly measured by imaging, but newer ECG-based AI tools are being studied as screening aids. One 2024 study found an ECG-based model could help screen for LVEF ≤30% with a negative predictive value of 95%, which is useful for triage, but imaging remains the gold standard for diagnosis (2024 study on AI ECG screening for low LVEF).
That means an ECG-based result may help flag risk, but it doesn't replace formal imaging. It also means a small difference between tests doesn't always mean your heart suddenly changed overnight. Different methods, different views, and different readers can produce somewhat different estimates.
If your breathing feels unsatisfying or you keep noticing a sense of not getting enough air, symptoms like air hunger are worth mentioning during follow-up because they can overlap with both heart and breathing disorders.
Bring your reports to appointments and ask one simple question: “Which test should we use as the main reference point going forward?”
That question helps you and your cardiologist compare future results more clearly.
Key Medical and Device-Based Treatment Options
Treatment for a 30 ejection fraction usually has more than one layer. Doctors don't just try to improve symptoms. They also try to protect the heart, reduce strain, prevent dangerous rhythms, and help you stay stable over time.
Medicines that support the heart
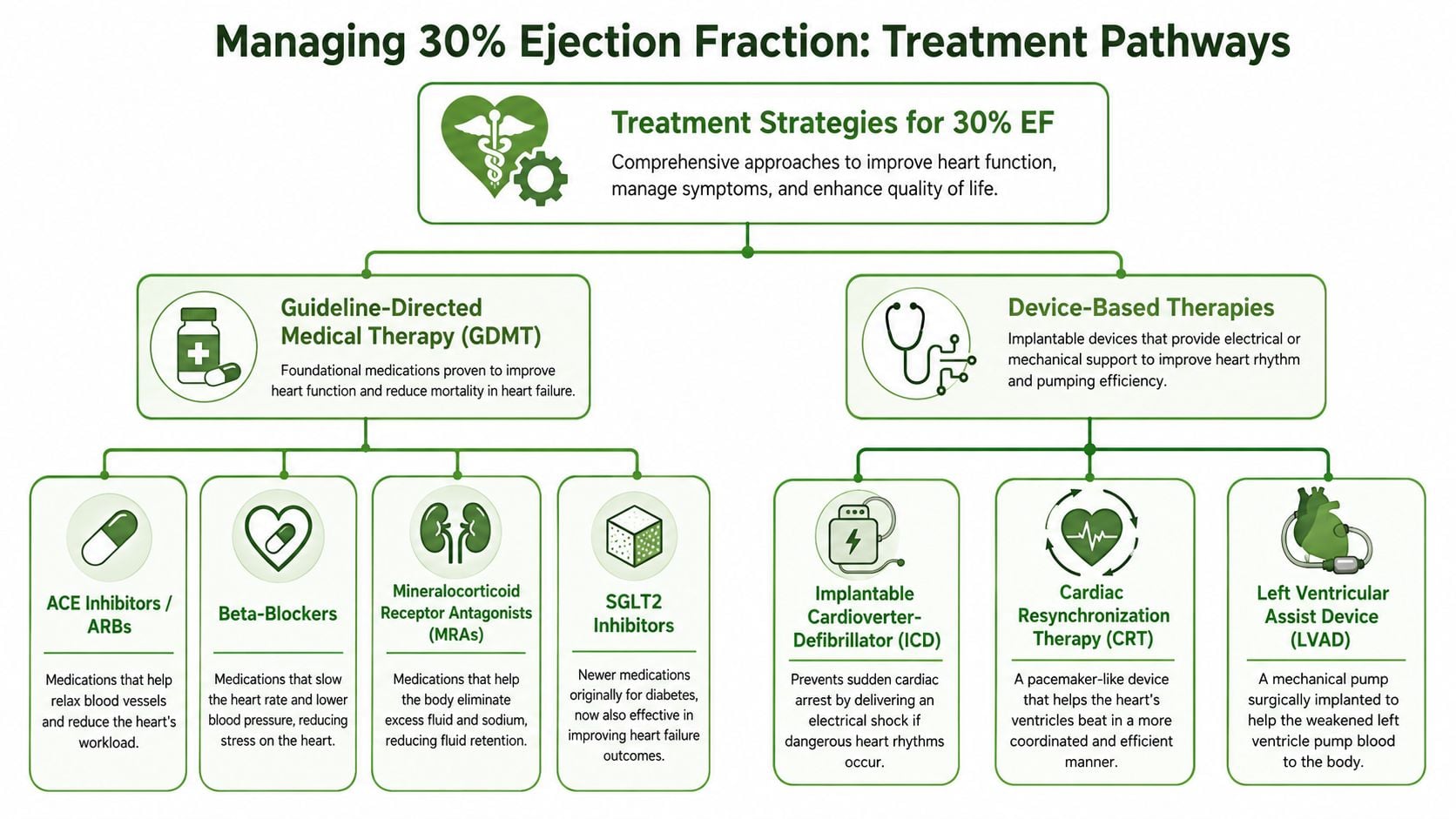
For many patients, the foundation is guideline-directed medical therapy.
Common medication groups include:
- ACE inhibitors or ARBs that relax blood vessels and reduce workload on the heart
- Beta-blockers that slow the heart rate and reduce stress on the heart muscle
- Mineralocorticoid receptor antagonists that help manage fluid and support heart failure treatment
- SGLT2 inhibitors that have become part of modern heart failure care
- Diuretics when fluid retention is a major issue
The purpose of these medicines isn't just to make you feel a little better today. The broader goal is to help the heart work under better conditions and lower the chances of decompensation, hospitalization, or rhythm-related events.
Devices that add protection or coordination
Sometimes medicine alone isn't enough.
An implantable cardioverter-defibrillator, or ICD, may be considered when the main concern is protection from dangerous ventricular rhythms. A cardiac resynchronization therapy device, or CRT, may help if the heart's electrical timing is off and the ventricles are not squeezing together efficiently.
These devices do different jobs. An ICD is mainly protective. CRT is more about improving coordination of the heartbeat in the right patient.
Advanced therapies in more severe cases
If symptoms remain difficult despite standard treatment, doctors may discuss more advanced options. These can include specialized heart failure care, evaluation for procedures, or mechanical support such as an LVAD in selected situations.
This part of the journey can feel overwhelming. It helps to keep the question practical: “What is the goal of this treatment in my case?” Sometimes the goal is symptom relief. Sometimes it is rhythm protection. Sometimes it is keeping options open for the future.
A separate issue many families worry about is affordability. Articles like ACG research on heart costs can be useful as a starting point for broader conversations about the financial side of chronic heart care, even though your own treatment plan and insurance situation will be specific to you.
Don't judge your treatment plan by whether it sounds “intense.” Judge it by whether each part has a clear purpose.
Empowering Yourself Through Lifestyle and Self-Care
A 30% ejection fraction affects more than a number on a report. It can shape how easily you breathe, how much energy you have, how well you sleep, and how steady you feel from one day to the next. The goal of self-care is to make daily life more predictable and to catch small changes before they turn into bigger problems.

What self-care looks like in real life
Good self-care is not about doing everything perfectly. It is about building a routine your heart and lungs can rely on.
- Take medications consistently. Skipping doses can make fluid balance, blood pressure, and symptoms harder to control.
- Track symptoms at home. Weight gain, ankle swelling, and breathing changes often show up before a person feels severely ill.
- Follow food and fluid guidance. Too much sodium can pull extra fluid into the body and make the heart work harder.
- Stay active within your doctor's limits. Gentle movement can support stamina, mood, circulation, and sleep.
- Protect sleep quality. Poor sleep can worsen fatigue and make breathing symptoms feel more intense the next day.
Daily monitoring involves watching for specific changes:
| Watch for | Why it matters |
|---|---|
| Shortness of breath | Can signal fluid buildup or worsening heart function |
| Swelling | May reflect fluid retention |
| Sudden change in energy | Can mean the heart is under more strain |
| Sleep disruption | May point to breathing instability or worsening symptoms |
One helpful way to approach this is to treat your notes like an early warning system. A pound or two of weight change, tighter shoes, needing more pillows, or getting winded sooner than usual may seem small on their own. Together, they can tell an important story.
Breathing, stress, and whole-body health
Many people with heart failure become highly alert to every breath. That reaction makes sense. When the heart is not pumping strongly, fluid can back up and make breathing feel harder, especially with activity or when lying flat. Stress can add another layer by making breaths faster and shallower, which increases the feeling of air hunger.
That is why whole-body care matters. Slow breathing practice, regular sleep hours, physician-approved exercise, and avoiding smoking or excess alcohol can reduce strain on both the heart and lungs. If your breathing pattern has changed, even something as basic as an abnormal respiratory rate is worth bringing up at follow-up.
This short video may help reinforce the bigger picture of heart-healthy living and symptom awareness.
Practical support outside the clinic
Living with a serious heart condition can also affect work, caregiving, transportation, and finances. Planning for those issues early can lower stress later. Some families review options like critical illness plans from Pounds Health while they are still thinking clearly, rather than waiting for an emergency.
Practical rule: make your self-care routine visible. Keep a weight log, medication list, and symptom notes where you will actually use them.
That simple system can help you notice patterns, ask better questions, and respond sooner when something changes.
Your Path Forward Questions for Your Cardiologist
The future with a 30 ejection fraction depends on the cause, your symptoms, your rhythm, your response to treatment, and how closely the condition is followed. Prognosis is personal. The most helpful mindset is to think in terms of ongoing management, not a one-time verdict.
Follow-up matters because treatment often changes over time. Medication doses may be adjusted. Repeat imaging may be ordered. New symptoms can shift the plan. The more clearly you understand your own case, the less powerless the diagnosis feels.
Questions worth bringing to your next visit
Write these down. Bring them with you. If possible, bring another person to listen and take notes.
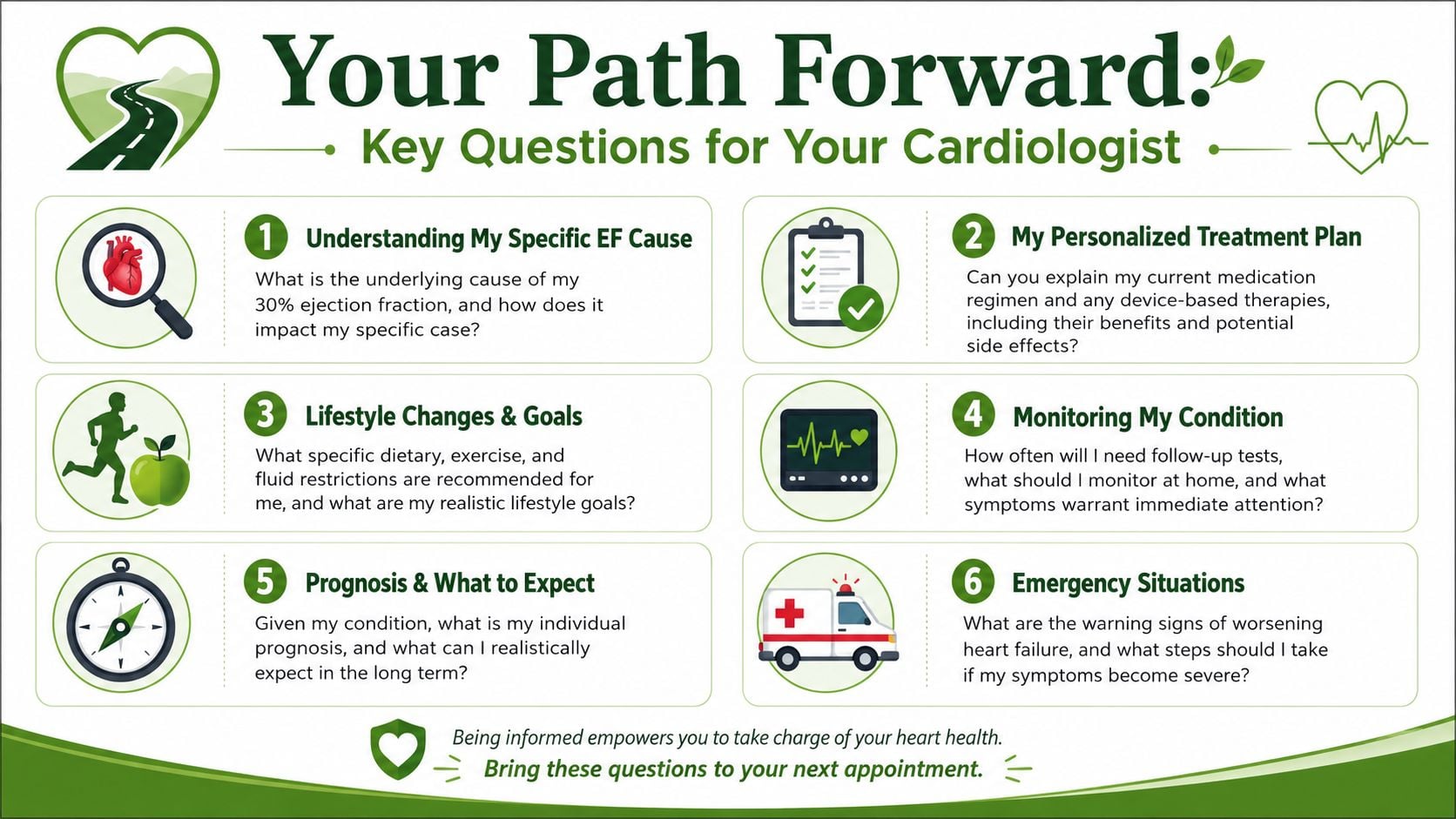
What caused my low EF
- Ask whether your doctor thinks the main issue is coronary disease, cardiomyopathy, valve disease, high blood pressure, rhythm problems, or something else.
What is the main goal of my treatment right now
- Is the priority symptom control, fluid management, rhythm protection, improving heart function, or preventing worsening?
Which medications am I taking for heart protection versus symptom relief
- That distinction helps you understand why some medicines matter even when you don't feel an immediate effect.
Am I a candidate for a device
- Ask whether an ICD or CRT is relevant in your case and what would make your doctor recommend one.
What should I monitor at home
- Ask exactly which changes should trigger a phone call, such as swelling, breathlessness, dizziness, fainting, or rapid weight change.
Could sleep-disordered breathing be part of my symptoms
- This is especially important if you snore, wake up often, stop breathing during sleep, or feel exhausted despite time in bed.
When should I seek urgent help
- Don't leave without knowing which symptoms are routine and which ones mean same-day evaluation or emergency care.
A calm way to think about the road ahead
You do not need to master heart failure in one appointment. You need a workable plan, a clear understanding of warning signs, and a team you can contact when things change.
The best patients are not the ones who never worry. They're the ones who notice changes early, ask direct questions, and stay engaged with care.
If sleep problems, breathing changes at night, jaw tension, or fatigue are part of your bigger health picture, Pain and Sleep Therapy Center offers evaluation for sleep-related breathing issues and airway-focused care. Their team helps patients understand symptoms that often overlap with poor sleep, breathing dysfunction, and overall well-being, so you can ask sharper questions and get more coordinated care.



