
You wake up hoping today will be different. Then the ache returns. It may sit in the cheek, spread toward the jaw, drift toward the temple, or feel like pressure deep under the skin that no one can clearly explain. Your dentist says the teeth look fine. Imaging may not show an obvious cause. One clinician mentions stress. Another mentions nerve pain. You're left with the same question most patients ask by the time they reach an orofacial pain specialist: what is this, and what helps?
That experience is common in persistent idiopathic facial pain, the condition many people still know by its older name, atypical facial pain. The pain is real. The confusion around it is real too. What helps most is a careful diagnosis, a treatment plan that doesn't jump too quickly to surgery, and a broader view that includes the nervous system, muscles, jaw function, and sometimes breathing and airway mechanics.
The Search for Answers to Unexplained Facial Pain
A typical story starts with a dull ache that doesn't behave the way a toothache, sinus infection, or classic nerve attack should. The pain may move. It may be constant for part of the day, then soften, then return. It may not match any single nerve branch neatly. That's one reason people often bounce from office to office before anyone names the pattern.

Some patients arrive worried they've missed something serious. Others are exhausted because every normal test feels less reassuring when the pain doesn't stop. If you've been trying to piece together symptoms, triggers, and dead ends, a useful starting point is learning more about what causes facial pain, because the facial pain category includes several different problems that can mimic each other.
Why this pain is so frustrating
The hardest part isn't only the pain itself. It's the mismatch between symptoms and simple explanations. People often hear versions of:
- Your scan looks normal. True, but that doesn't mean the nervous system is functioning normally.
- Maybe it's stress. Stress can amplify pain, but it doesn't make the pain imaginary.
- Maybe it's your teeth. Sometimes it is. Sometimes it isn't.
Persistent, unexplained facial pain deserves a structured workup, not a shrug.
A good clinician takes the pattern seriously, validates what you're feeling, and helps sort out what this pain is and what it isn't. That's where the path becomes clearer.
Decoding Persistent Idiopathic Facial Pain
Persistent idiopathic facial pain, or PIFP, is the modern term for what was often called atypical facial pain. “Idiopathic” means the pain doesn't come with one clear structural explanation that neatly accounts for every symptom. It does not mean the pain is vague, exaggerated, or made up.
A useful analogy is a faulty car alarm. A normal alarm activates when there's a real threat. A faulty alarm becomes too sensitive and starts sounding when the trigger is minor, misread, or no longer present. In PIFP, the pain system can behave in a similar way. The nervous system keeps signaling distress even when there isn't an obvious dental infection, fracture, or compressive lesion explaining the full picture.
How it differs from other facial pain disorders
PIFP usually doesn't feel like trigeminal neuralgia. Trigeminal neuralgia is classically sharp, electric, and shock-like. PIFP is more often described as dull, aching, nagging, pressure-like, or poorly localized.
It also doesn't always behave like a TMJ disorder. Jaw joint and muscle pain often has clearer links to chewing, clenching, joint loading, or limited opening. PIFP may overlap with those issues, but it typically has a broader and less mechanical feel.
Here's a simple comparison:
| Condition | Common pain quality | Pattern |
|---|---|---|
| PIFP | Dull, aching, diffuse | Often persistent and harder to localize |
| Trigeminal neuralgia | Electric, stabbing, shock-like | Brief attacks, often triggered |
| TMJ-related pain | Sore, tight, joint or muscle pain | Often worse with jaw use |
The psychogenic label is outdated
Older content often framed atypical facial pain as mainly psychogenic. That view doesn't hold up well clinically. A modern review from Columbia Neurosurgery states that PIFP is not merely a diagnosis of exclusion and notes that while psychological treatments can help as an adjunct, “in recalcitrant cases, interventional procedures can be considered”. That's an important correction because it affirms the pain has a real physiological basis while still recognizing the mind-body connection in chronic pain care through Columbia's overview of atypical facial pain.
Clinical reality: pain can be both neurologic and emotionally burdensome at the same time.
That distinction matters. Patients do better when they're treated as people with a complex pain disorder, not as people who need to be talked out of their symptoms.
The Path to a Clear Diagnosis
Diagnosing atypical facial pain treatment needs starts like detective work. Not dramatic detective work. Careful detective work. The goal is to rule out more common and more dangerous causes first, then identify whether the remaining pattern fits PIFP, a neuropathic pain disorder, a musculoskeletal disorder, or a combination.
Atypical facial pain is rare, with an annual incidence of 3 to 4 cases per 100,000 people, and because of that rarity and complexity, accurate diagnosis matters. Neurosurgical organizations have warned that surgery can be “completely inappropriate” for AFP and may worsen the condition, as noted in this clinical review on atypical facial pain.
What a specialist is trying to rule out
Before anyone settles on PIFP, the workup usually considers conditions such as:
- Dental sources like pulp inflammation, cracked teeth, bite trauma, or post-procedure pain
- Sinus and ENT causes when symptoms fit congestion, pressure patterns, or infection
- TMJ and muscular pain involving the jaw joints, chewing muscles, neck, and oral habits
- Classic neuralgias that produce sharper, more defined nerve distributions
- Headache disorders that can refer pain into the face
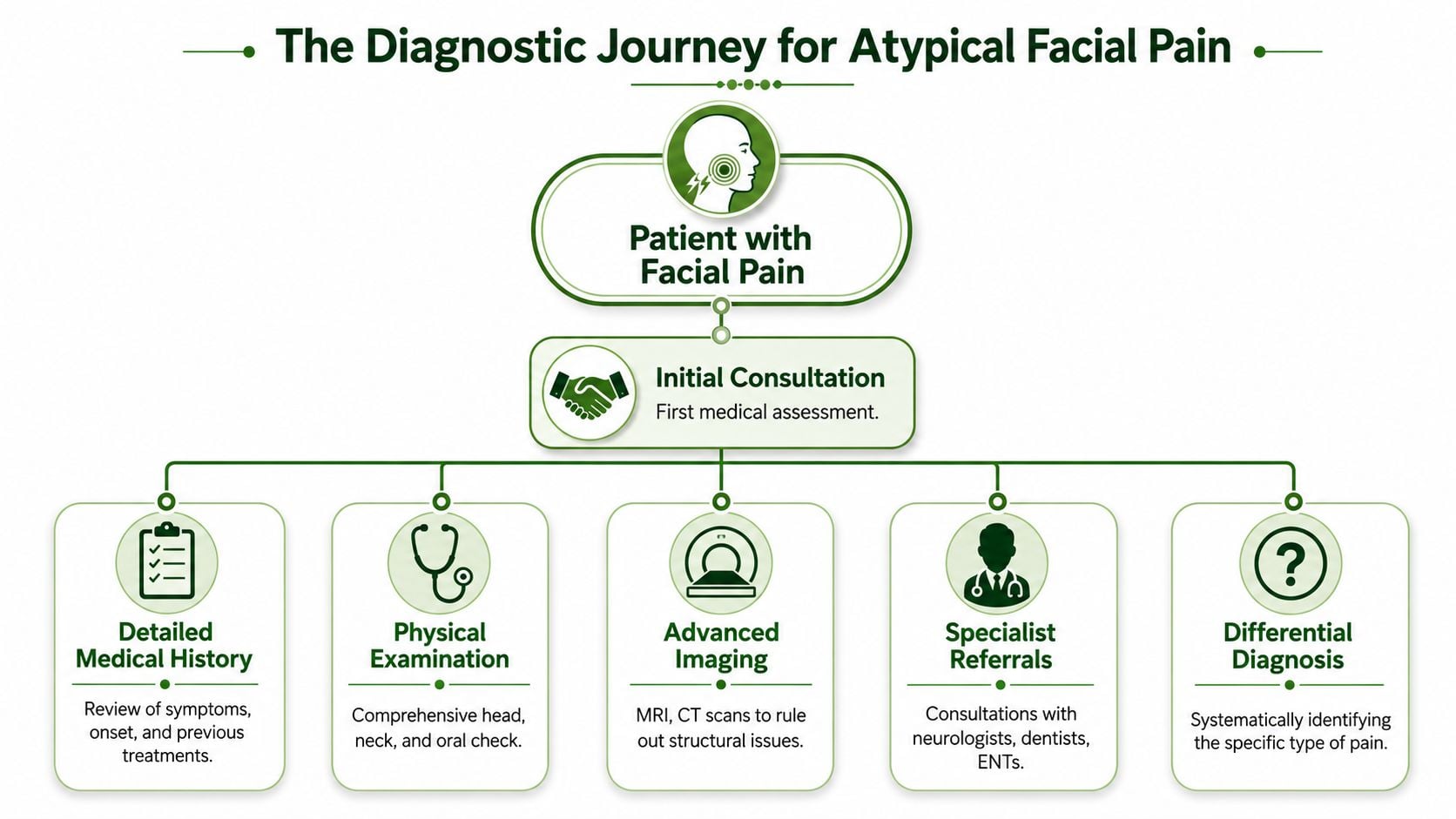
That process is called differential diagnosis. It means your clinician isn't guessing. They're sorting possibilities in a logical order.
What a complete evaluation often includes
Patients are often relieved to hear that the exam is broader than “Where does it hurt?” A strong assessment usually includes:
A detailed history
When the pain started, what it feels like, whether it migrates, what procedures came before it, and what treatments have already failed.A hands-on exam
This may include jaw movement, bite loading, palpation of facial and neck muscles, cranial nerve screening, and checks for allodynia or trigger zones.Imaging or referrals when needed
Imaging doesn't diagnose every pain disorder, but it helps rule out structural problems. Depending on the pattern, collaboration with dentistry, neurology, ENT, or sleep medicine may be appropriate.
The diagnosis often becomes clearer not because one test “proves” PIFP, but because the full pattern stops fitting simpler explanations.
Why rushing to procedures is risky
Facial pain invites over-treatment when the diagnosis is muddy. I've seen patients undergo dental work, extractions, or procedural recommendations based on location alone. That's rarely enough. In facial pain, the map can mislead you. The area that hurts isn't always the tissue generating the pain.
That's why the first win in atypical facial pain treatment is often not a procedure. It's precision.
Conventional Atypical Facial Pain Treatment Options
The foundation of atypical facial pain treatment is usually conservative care. Medication names can sound alarming at first because many were originally developed for depression, seizures, or other conditions. In this setting, they're used because they can calm pain signaling, not because the clinician thinks your pain is “just emotional.”
A helpful way to think about them is as volume knobs for an overactive pain system.
Medications that commonly help
A commonly used pharmacologic approach combines a tricyclic antidepressant such as amitriptyline at 10 to 50 mg daily with an antiepileptic such as gabapentin at 300 to 1200 mg daily, and this combination has shown better efficacy than newer SSRIs like fluoxetine in PIFP care, according to the European Academy of Oral Medicine review.
That doesn't mean every patient needs both. It means these classes are often chosen because they can reduce pain amplification in the nervous system.
- Amitriptyline can support descending pain control pathways and may also help when sleep is poor.
- Gabapentin is often used to reduce hyperexcitable nerve firing.
- Other options may be considered based on symptom pattern, side effects, and medical history.
What tends not to work well
Patients often ask whether newer antidepressants automatically work better because they're newer. Not in this condition. The evidence base for PIFP is limited, and some newer agents have shown less consistent benefit than older tricyclics in clinical practice.
A separate review of pharmacotherapy for persistent idiopathic facial pain found only a small number of randomized trials, which tells you something important. Treatment often depends on pattern recognition, careful titration, and follow-up rather than a single universally effective drug. In that same body of evidence, onabotulinum toxin A had inconsistent results, and one 2023 study found no significant reduction in average pain intensity compared with placebo during weeks 5 to 8, with a mean difference of 0.00 and a 95% confidence interval from −0.57 to 0.57, as summarized by the British and Irish Society for Oral Medicine resource on persistent idiopathic facial pain.
Non-drug treatments matter
Medication alone is often incomplete care. The best plans usually also include some combination of:
- Cognitive behavioral therapy to reduce catastrophizing, fear, and pain spirals
- Physical therapy for cervical, jaw, and facial muscle tension that keeps the system irritated
- Behavioral coaching around sleep, clenching, oral posture, and pacing
Medication can lower the alarm volume. Rehabilitation teaches the system not to keep pulling the alarm.
That's why good atypical facial pain treatment isn't just about writing a prescription. It's about changing the conditions that keep the pain circuit active.
Innovative Non-Surgical and Regenerative Therapies
When conventional care only partly helps, many patients assume the next step must be an invasive procedure. That's not the only option. There's a large middle ground between “just live with it” and surgery, a space where regenerative and functional therapies can make clinical sense.
One reason this middle ground gets missed is that standard treatment guides often lean toward medication algorithms, neurosurgical discussion, or psychological support. Yet a 2017 review noted that low-energy diode laser therapy may be a useful alternative treatment for PIFP, highlighting how non-invasive options are often under-discussed in routine patient education through this review of persistent idiopathic facial pain.
Why regenerative care fits this condition
Not every facial pain patient is a candidate for regenerative treatment, and these therapies aren't magic. But they can be logical when there's evidence of ongoing strain, sensitized soft tissues, ligament laxity, overload in the jaw system, or chronic musculoskeletal contributors around the face and neck.
Think of symptom-masking treatment as turning down the radio. Regenerative treatment aims to repair the speaker when the hardware itself is contributing noise.
Some examples include:
Prolotherapy
Used to stimulate a healing response in irritated or unstable connective tissues.Platelet-Rich Fibrin or PRF
Best understood as a concentrated healing signal made from the patient's own blood, delivered to tissue that may need support.Cold laser or low-level laser therapy
A non-invasive approach used to support tissue healing and modulate pain in a gentler way than procedural destruction.
For readers exploring biologic options in more depth, this overview of orthobiologic therapy explains how regenerative strategies are used to support healing rather than mere symptom suppression.
Airway health and muscle balance are often overlooked
Atypical facial pain treatment also benefits from asking a broader functional question. Why is the face under strain in the first place?
When patients mouth-breathe, brace the jaw, clench during sleep, hold poor tongue posture, or compensate for airway resistance, the facial muscles and joints can stay in a constant low-grade protective state. Over time, that can feed pain, especially in a sensitized nervous system. This is why airway evaluation, nasal breathing, and orofacial myofunctional therapy deserve a place in the conversation.
That approach doesn't claim airway problems cause every case of PIFP. It recognizes that chronic facial pain often has layered contributors, and if you ignore those contributors, treatment may stall.
A short explainer can help clarify how movement and function fit into pain care:
Where supportive options fit in
Some patients also ask about wellness tools that may complement, but not replace, a medical plan. If you're curious about that category, this guide to understanding CBD oil for nerve pain offers a practical overview of questions patients commonly raise.
The key is using supportive tools carefully, within a larger plan that still addresses diagnosis, tissue health, pain processing, and daily function.
Why a Multidisciplinary Care Team Is Crucial
Treating persistent facial pain is a lot like building a house. You wouldn't ask one person to do the electrical, plumbing, framing, roofing, and finish work alone. Facial pain works the same way. The nervous system, jaw mechanics, muscles, sleep quality, breathing pattern, and emotional load all affect the final result.
That's why a single-specialty mindset often falls short.
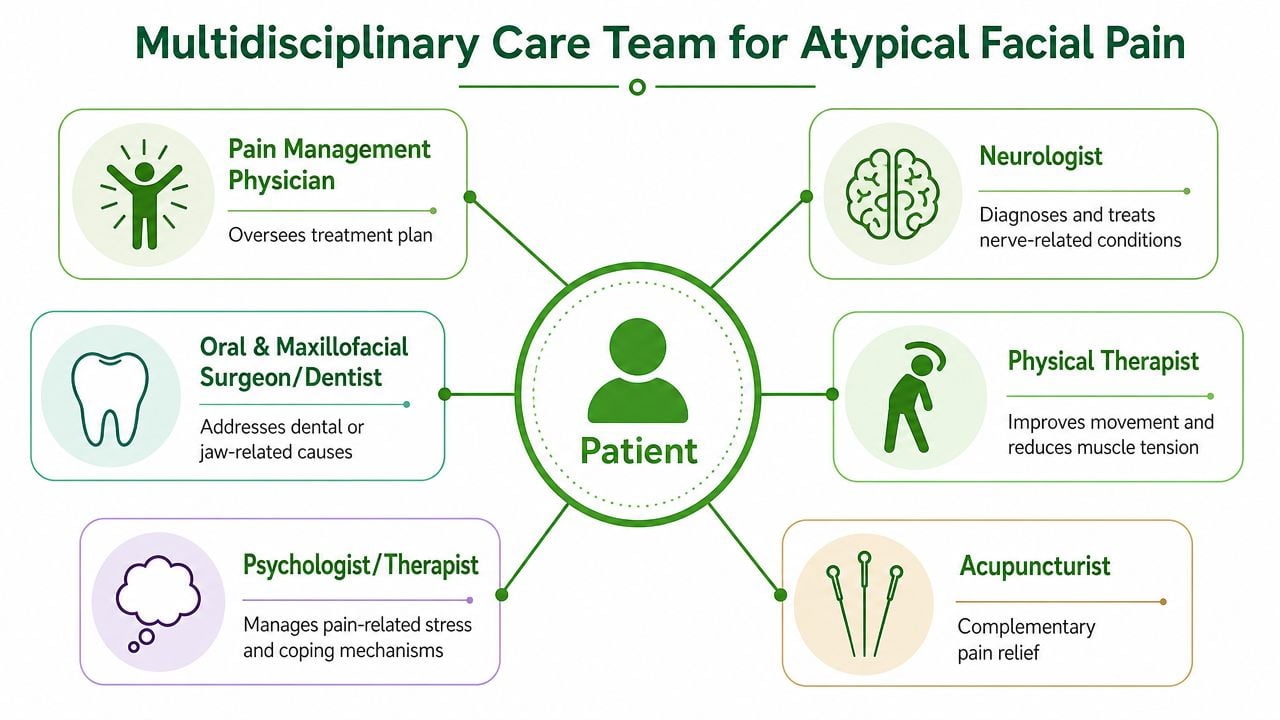
Who does what
The best outcomes usually come from coordinated care, not parallel opinions that never connect.
Orofacial pain specialist
Acts like the general contractor. This clinician helps organize the diagnosis and sequence treatment logically.Physical therapist
Works on neck mechanics, jaw loading, posture, muscle guarding, and movement patterns that keep pain active.Neurologist or neurosurgeon
Helpful when the pattern raises concern for neuralgia, headache disorder, or refractory neuropathic pain.Behavioral health clinician
Supports coping, fear reduction, sleep, and the emotional exhaustion that chronic pain creates.Airway or myofunctional specialist
Addresses breathing pattern, oral posture, and functional contributors that can perpetuate tension and pain.
For patients who need a broader coordinated model, a multidisciplinary approach to pain management reflects how this kind of case is best handled.
Why team sequencing matters
In refractory cases, neurosurgical modalities such as microvascular decompression or Gamma Knife radiosurgery may enter the conversation. Even then, treatment is rarely one-step. Some specialists use a temporary stimulator trial and look for at least 50% pain reduction before moving forward with permanent implantation, which underscores how carefully these cases must be staged according to this neurosurgical discussion of atypical facial pain treatment.
Good care is collaborative. Great care is collaborative in the right order.
If a patient gets medication without rehabilitation, or counseling without structural evaluation, or procedures without diagnosis, progress often stalls. Team care closes those gaps.
Creating Your Personalized Path to Relief
Relief usually starts when the care plan becomes specific. Not generic. Not copied from someone else's jaw pain handout. Specific to your symptoms, triggers, history, sleep, bite habits, stress load, and functional findings.
A practical plan often includes a few immediate self-care steps while formal treatment is being built.
What you can do now
Choose softer foods during flares
Give irritated muscles and joints less work when chewing makes symptoms worse.Reduce jaw overuse
Limit gum chewing, nail biting, wide yawning, and resting your jaw in a clenched position.Use gentle heat or guided relaxation
This can help downshift muscle guarding around the face and neck.Track your pattern
Note where the pain starts, what time of day it worsens, whether sleep changes it, and whether stress, posture, or chewing affect it.Support mental health without dismissing the pain
Chronic facial pain can be isolating. If emotional strain is building, a resource like Canadian mental health support online may be useful as part of a broader care plan.
When to seek specialist care
Ask for an orofacial pain or facial pain specialist evaluation if any of the following apply:
- The pain has lasted longer than three months.
- Dental or routine medical treatment hasn't solved it.
- The pain pattern is diffuse, migratory, or hard to explain.
- You've been told different things by different clinicians.
- The pain is affecting sleep, eating, mood, or work.
The goal isn't to chase endless treatments. It's to build a plan in the right sequence. Diagnosis first. Conservative care second. Functional contributors addressed throughout. More advanced options only when the clinical picture supports them.
You don't need to prove your pain is real. You need a team that knows how to evaluate it properly.
Lasting improvement is possible, but it usually comes from layered care rather than a single fix. That's the mindset behind modern atypical facial pain treatment.
If you're dealing with persistent facial pain, jaw symptoms, headaches, or sleep-related contributors that no one has fully connected, Pain and Sleep Therapy Center offers specialized evaluation focused on root-cause diagnosis and non-surgical treatment options. A careful assessment can clarify what's driving your symptoms and help you move toward a practical, personalized plan for relief.



