
A lot of families arrive at the same question from different directions. A parent notices a child who snores, sleeps with an open mouth, wakes up tired, struggles to focus, and also has crowded teeth. An adult comes in for jaw pain, clenching, headaches, or a bite that never feels settled, then mentions poor sleep almost as an afterthought. Those signs often seem unrelated until you look at the face, jaws, tongue posture, and breathing pattern as one system.
That's where airway focused orthodontics changes the conversation. It treats crooked teeth as part of a bigger structural and functional picture, not as an isolated cosmetic problem. Teeth don't erupt in a vacuum. They develop inside jaws, beside a tongue, under muscles, and around an airway that has to work every hour of every day.
A straight smile can be healthy. It can also hide a narrow palate, poor oral posture, chronic mouth breathing, or a sleep problem that no one has connected to the bite. When treatment focuses only on alignment, it may miss the reason the teeth became crowded in the first place.
A New Perspective on a Perfect Smile
A child who snores and has crowded teeth is not just a child with two separate issues. In many cases, the same growth pattern that leaves too little room for teeth also leaves too little room for the tongue and not enough support for easy nasal breathing.
That's the basic shift in airway focused orthodontics. Instead of asking only, “How do we line up the teeth?” the better question is, “What kind of jaw development and oral function will support healthy breathing, sleeping, swallowing, and facial growth?”
More than cosmetic alignment
Traditional orthodontic care often centers on bite fit and smile appearance. Those goals still matter. Chewing comfort, dental stability, and aesthetics are important.
But a modern airway-centered view goes further. It looks at whether the upper jaw is wide enough, whether the lower jaw is positioned in a way that supports the airway, whether the tongue rests on the palate, and whether the patient breathes through the nose or the mouth most of the time.
A healthy bite should support more than straight teeth. It should also support a tongue that fits, lips that close comfortably, and breathing that doesn't become harder at night.
When that foundation is off, the consequences can spread beyond the mouth. Sleep quality can suffer. Daytime energy can drop. Children may seem restless or unfocused because they aren't sleeping well, not because they “just need to grow out of it.”
What this approach tries to solve
Airway focused orthodontics aims to guide growth and create space where the body needs it most.
- Space for the teeth so alignment isn't forced into a small arch
- Space for the tongue so it can rest where it should
- Space for airflow through the nose and throat
- Space for healthy development so the face grows with better balance and function
This is why families often feel relief when they finally hear an airway-based explanation. It connects symptoms that previously seemed scattered: crooked teeth, open-mouth posture, snoring, restless sleep, jaw strain, and fatigue.
A smile still matters. It just isn't the whole story.
Why Breathing and Jaw Structure Are Linked
The jaw and airway relationship is mechanical. If the skeletal framework is narrow or poorly positioned, the soft tissues inside that space have fewer good options. The tongue may sit low. The lips may stay apart. Breathing may shift from the nose to the mouth, especially during sleep.
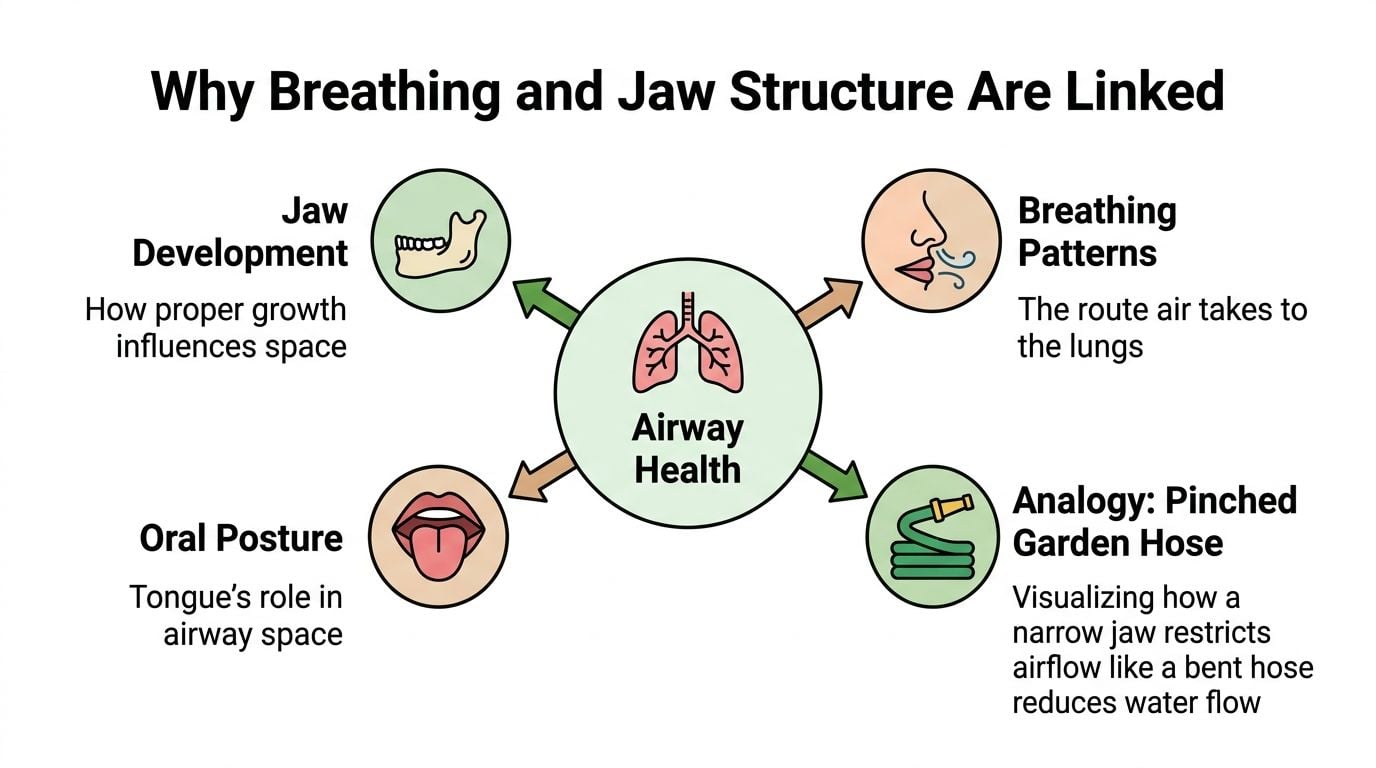
The pinched garden hose analogy
A simple way to understand this is to think of airflow like water moving through a garden hose. If the hose is open and round, flow is smooth. If the hose is pinched, bent, or compressed, flow drops and pressure changes.
The airway behaves in a similar way. A narrow upper jaw can reduce the space available for the nasal passage and the tongue. A retrusive lower jaw can leave the tongue and soft tissues farther back than ideal. During sleep, when muscles relax, that reduced space matters even more.
That doesn't mean every narrow jaw causes sleep apnea. It does mean structure can contribute to breathing strain, and structure is one piece of the overall sleep picture.
Why teeth can signal a bigger problem
Crowding is often the visible clue patients notice first. It tells you there may not be enough skeletal room for the dentition. If there isn't enough room for teeth, it's reasonable to ask whether there's enough room for the tongue and whether the upper arch is supporting healthy nasal breathing.
The clinical effects go beyond appearance. Airway-focused orthodontics has demonstrated measurable benefits on sleep-disordered breathing, and clinical data shows that children who previously snored or slept restlessly often begin sleeping soundly within weeks of treatment, with improvement in daytime energy and cognitive function as well. Research also links rapid maxillary expansion to reduced airway obstruction and improved sleep quality, lowering the Apnea-Hypopnea Index in treated patients, as described in this overview of airway orthodontics and kids' sleep apnea.
If you're trying to understand one major daily habit behind these changes, it helps to compare nasal breathing vs mouth breathing. The route air takes affects oral posture, sleep quality, and how facial structures are used over time.
Practical rule: When a patient has crowded teeth, chronic mouth breathing, and poor sleep, it's worth evaluating them as one connected pattern, not three separate complaints.
Sleep, oxygen, and the rest of the body
Nighttime breathing problems don't stay in the bedroom. Poor-quality sleep can show up as fatigue, headaches, irritability, clenching, and trouble focusing. In adults, untreated obstructive sleep apnea can overlap with broader medical concerns that require coordinated care. For clinicians or patients trying to understand one part of that bigger picture, this CPAP and CHF clinician's guide gives useful context on how sleep-disordered breathing fits into cardiovascular care.
A good airway evaluation doesn't assume the teeth caused everything. It asks how structure, function, sleep, and medical health may be interacting in that specific person.
The Diagnostic Journey to Identify Airway Issues
Airway problems shouldn't be diagnosed by looking at a smile photo and making assumptions. A proper evaluation is more like assembling a map. You need the symptom history, the structural picture, and the muscle-function picture before treatment makes sense.
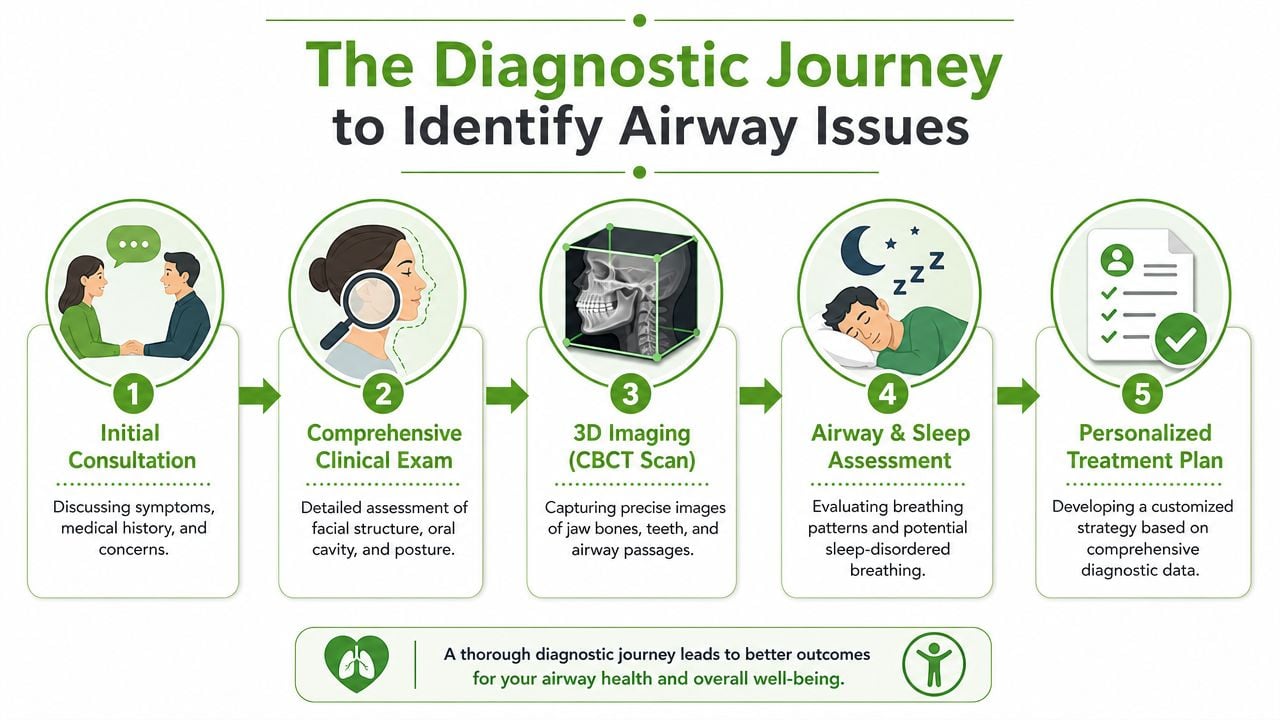
Step one looks beyond the teeth
The first clues usually come from the history. Snoring, restless sleep, dry mouth on waking, fatigue, clenching, headaches, mouth breathing, and speech or swallowing habits all matter. In children, parents often mention dark circles, behavioral concerns, open-mouth posture, or noisy sleep long before anyone suspects the bite is involved.
A thorough exam also looks at facial proportions, lip seal, tongue posture, arch form, and the way the jaws relate to each other. You're not just checking alignment. You're looking for signs that the patient has adapted to a restricted pattern.
3D imaging changes what you can see
Some airway issues are hard to appreciate with standard records alone. That's why the clinical protocol for airway-focused orthodontics mandates the use of 3D airway imaging and functional jaw orthopedics, helping clinicians assess upper airway dimensions and plan treatment that promotes adequate room for all teeth and restores proper breathing patterns early, as discussed in this clinical review on airway-focused orthodontic protocol.
A Cone Beam Computed Tomography scan, often called CBCT, can show:
- The width of the maxilla and whether the palate is narrow
- The position of the jaws relative to the airway space
- The airway form in three dimensions, rather than a flat estimate
- The dental and skeletal relationship that will influence treatment choices
That information matters because treatment should match anatomy. A child with active growth has different options than an adult with a mature suture pattern and longstanding compensation.
Function has to be measured too
A patient can have a beautifully planned appliance and still struggle if the muscles keep pushing in the wrong direction. That's why an orofacial myofunctional assessment is part of a serious airway workup.
This assessment looks at habits and muscle patterns such as:
Tongue rest posture
Is the tongue up against the palate, or sitting low in the mouth?Swallow pattern
Is the patient using facial muscles excessively or thrusting forward?Lip function
Can the lips stay closed comfortably at rest?Breathing behavior
Is nasal breathing easy, or has mouth breathing become the default?
A scan can show the space. A functional assessment shows how the patient is using it.
Sleep evaluation is the third major piece. If symptoms suggest sleep-disordered breathing, that history needs to be taken seriously and, when appropriate, coordinated with sleep medicine. Orthodontic planning works best when it's informed by what happens at night, not just by what the teeth look like during the day.
Common Airway Focused Orthodontic Treatments
Airway treatment is not one appliance. It's a toolkit. The right tool depends on age, growth stage, anatomy, symptoms, and whether the priority is expansion, jaw guidance, dental alignment, or stabilization.

Expansion for a narrow upper jaw
When the upper jaw is too narrow, one common goal is to create more room across the palate. In growing patients, rapid maxillary expansion, often shortened to RME, is one of the best-known orthopedic options.
Research shows that functional appliance therapy and rapid maxillary expansion produce statistically significant increases in upper airway dimensions in growing patients, and systematic reviews confirm that RME has a positive effect on reducing Respiratory Disturbance Index scores in pediatric obstructive sleep apnea cases, often lowering the Apnea-Hypopnea Index as well, according to this review of orthopedic interventions and upper airway change.
That matters because expansion is not just about making room for crooked teeth. It can also support nasal airflow and tongue posture by changing the skeletal frame those tissues occupy.
Growth guidance in children
Children still have developmental opportunity. If the lower jaw sits back or the bite pattern suggests a skeletal imbalance, functional appliances may be used to guide growth in a healthier direction.
These appliances aren't magic. They work best when the timing is appropriate and when the treatment goal is realistic. In the right child, they can help improve the relationship between the upper and lower jaws while supporting a more favorable airway environment.
Common examples in this category include:
- Functional appliances that encourage a better jaw relationship during growth
- Expansion devices that address transverse deficiency in the upper arch
- Phase-based treatment plans that prioritize structure first and detailed alignment later
Adult treatment looks different
Adults can still benefit from airway-focused care, but the mechanics are different because growth is complete. In some cases, clinicians use adult skeletal expansion approaches such as MSE or MARPE to widen narrow maxillary arches through temporary skeletal anchorage rather than dental tipping alone. The goal is true skeletal change where anatomy allows it, not just moving crowns outward.
Adults often also need a broader treatment framework. Orthodontics may be paired with sleep medicine, bite stabilization, or jaw and muscle care. For patients exploring that overlap, dental sleep medicine is often part of the larger picture.
Aligners and braces still have a role
Clear aligners and braces aren't “bad for the airway.” They are tools. Their value depends on the treatment plan behind them.
Used thoughtfully, they can refine tooth position after expansion, coordinate the arches, and stabilize a healthier bite. Used without regard to tongue space, oral posture, or airway anatomy, they may solve the cosmetic problem while leaving the functional problem untouched.
A useful way to think about treatment choices is this:
| Treatment category | Main purpose | Best fit |
|---|---|---|
| Expansion | Increase arch width and improve skeletal room | Narrow upper jaws, crowding with transverse deficiency |
| Growth modification | Guide jaw development during active growth | Children with developing skeletal imbalance |
| Aligners or braces | Refine tooth position and bite coordination | Finishing and stabilization after structural planning |
| Adult skeletal expansion options | Create skeletal widening in selected adults | Mature patients with restricted maxillary anatomy |
Good treatment creates space with intention. It doesn't just rearrange teeth inside a cramped framework.
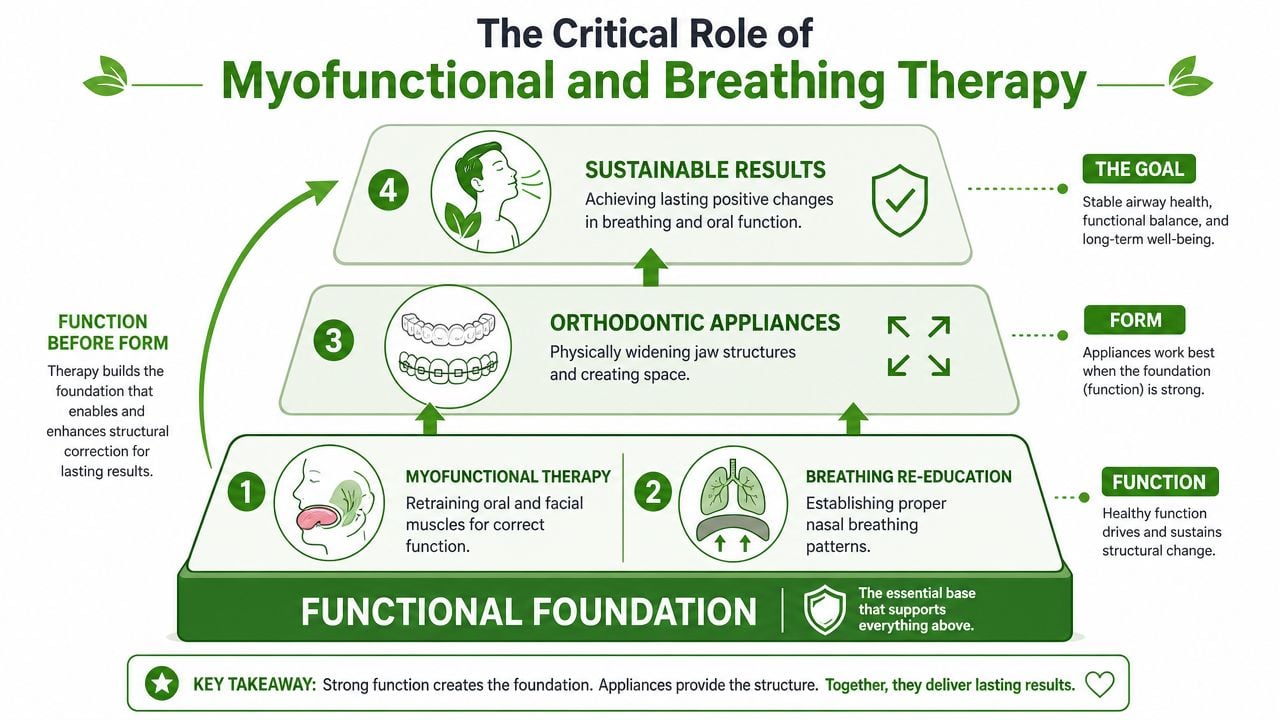
The Critical Role of Myofunctional and Breathing Therapy
An appliance can change structure. It cannot, by itself, teach the lips to stay closed, the tongue to rest on the palate, or the patient to stop using the mouth as the main airway.
That's why form without function often fails.
Why relapse happens
A critical issue in airway care is that expanding the jaw does not automatically eliminate the habits that helped create the problem. Evidence suggests that without correcting dysfunctional breathing and tongue posture, relapse is likely, and untreated compensatory behaviors are a primary cause of treatment instability, as explained in this discussion of form, function, and airway orthodontics.
That point gets missed often. Families hear about expanders, aligners, and jaw development. They hear much less about the muscular software that has to run the new hardware.
What therapy is actually doing
Orofacial myofunctional therapy retrains the muscles of the tongue, lips, cheeks, and face so they support a healthier oral posture and swallow. Breathing retraining helps patients develop more consistent nasal breathing patterns and better control of dysfunctional habits.
These therapies commonly work on:
- Tongue posture so the tongue supports the palate instead of sitting low
- Lip seal so the mouth can rest closed without strain
- Swallow mechanics so the facial muscles stop compensating
- Breathing patterns so nasal breathing becomes easier and more natural
Patients who mouth-breathe out of habit often need specific coaching, not just instructions to “breathe through your nose.” For many, myofunctional therapy for mouth breathing is the missing piece that makes orthodontic change hold.
“The appliance can create the opportunity. The muscles have to learn how to keep it.”
Why multidisciplinary care works better
Airway care involves more than orthodontics alone. A patient may need an orthodontist for structure, a myofunctional therapist for oral posture, a breathing coach for nasal patterning, and a sleep provider for nighttime symptoms. If there's tongue restriction, nasal resistance, or complex sleep-disordered breathing, other specialists may need to join the plan.
That isn't overcomplication. It's precision.
A narrow palate and a low tongue are not separate stories. They're part of the same functional loop. If you only correct one side of that loop, the body often drifts back toward the old pattern.
Who Is a Candidate for This Approach
Children and adults can both be candidates for airway-focused care, but the treatment goals are not identical.
In children, the priority is often guiding growth early. The jaws are still developing, habits are still forming, and orthopedic change is generally more biologically favorable. If a child has a narrow arch, poor tongue posture, chronic mouth breathing, snoring, or restless sleep, airway-focused evaluation can help determine whether those signs are connected.
Children benefit from prevention
A child does not need to wait for all permanent teeth to erupt before someone asks whether the face is growing with enough room. Early support may help create space for teeth, encourage better oral posture, and reduce the structural patterns that contribute to disordered breathing later on.
This doesn't mean every child needs treatment. It means the right child shouldn't be overlooked because the problem was dismissed as “just crooked teeth.”
Adults need realistic expectations
Adults usually come with more established patterns. They may already have TMJ symptoms, clenching, chronic fatigue, snoring, or a diagnosis of obstructive sleep apnea. Orthodontics can improve arch form and airway space, but adults deserve honest counseling about limits as well as possibilities.
A common question is whether orthodontics alone can reverse adult OSA. The nuance matters. Orthodontics can improve airway space, but “improving” airway anatomy is not the same as “curing” OSA, which often requires a multidisciplinary approach that may include myofunctional therapy or sleep medicine, as discussed in this review of airway-focused orthodontics for adults.
The best candidates are patients willing to treat both the structure and the habits that affect breathing.
Signs that justify an evaluation
A patient may deserve a closer airway workup if they have several of these signs together:
- Crowded teeth with a narrow palate
- Habitual mouth breathing or poor lip seal
- Snoring, restless sleep, or waking unrefreshed
- Jaw tension, clenching, or chronic facial fatigue
- Low tongue posture or dysfunctional swallow patterns
The goal isn't to label everyone with an airway disorder. It's to identify who may benefit from a broader, root-cause plan instead of cosmetic alignment alone.
Your Integrated Care Pathway at Our Center
The best airway care rarely comes from one provider working in isolation. Patients do better when the diagnostic picture is shared, the treatment sequence is deliberate, and the team is looking at breathing, sleep, muscle function, and jaw mechanics together.
At our center, that process usually starts with a consultation or provider referral. The first step is listening carefully to the complaint that brought the patient in, whether that's snoring, fatigue, clenching, headaches, facial pain, crowded teeth, or a child who never seems to sleep well. From there, the evaluation broadens to include the airway, bite, oral posture, and the functional patterns that may be driving symptoms.
What coordinated care looks like
Instead of treating each issue as a separate silo, the plan is built across disciplines.
- Diagnostic review combines symptom history, exam findings, and appropriate imaging or sleep-related screening
- Orthodontic planning considers whether the arches and jaws support healthy breathing, not just alignment
- Myofunctional support helps retrain tongue posture, swallowing, and lip function
- Breathing and sleep coordination addresses nasal breathing habits and when needed involves sleep medicine principles
- TMJ and pain management input helps when jaw joints, muscles, or headaches are part of the case
This kind of care matters because a patient with airway restriction may also have muscle compensation. A patient with TMJ pain may also have poor sleep. A child with mouth breathing may also have a swallow pattern that keeps treatment unstable unless it's addressed directly.
When the plan is integrated, patients don't have to guess which symptom matters most. The team works from the full picture.
If you're looking for a root-cause approach to jaw development, sleep-disordered breathing, TMJ symptoms, or myofunctional therapy, Pain and Sleep Therapy Center offers coordinated evaluation and care designed around the whole patient, not just the teeth.



